Cirrhosis liver
Reading File
Finding Sources
Searching PubMed
"liver cirrhosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich, comprehensive content from authoritative textbooks. Let me compile the full detailed answer.
Liver Cirrhosis
Definition
Cirrhosis is the diffuse transformation of the liver into regenerative parenchymal nodules surrounded by fibrous bands. It represents the end stage of any chronic liver disease and is the morphologic change most often associated with chronic liver disease. Importantly, not all chronic liver disease ends in cirrhosis, and not all cirrhosis leads to end-stage liver failure.
- Robbins & Kumar Basic Pathology, p. 598
Normal vs. Cirrhotic Liver
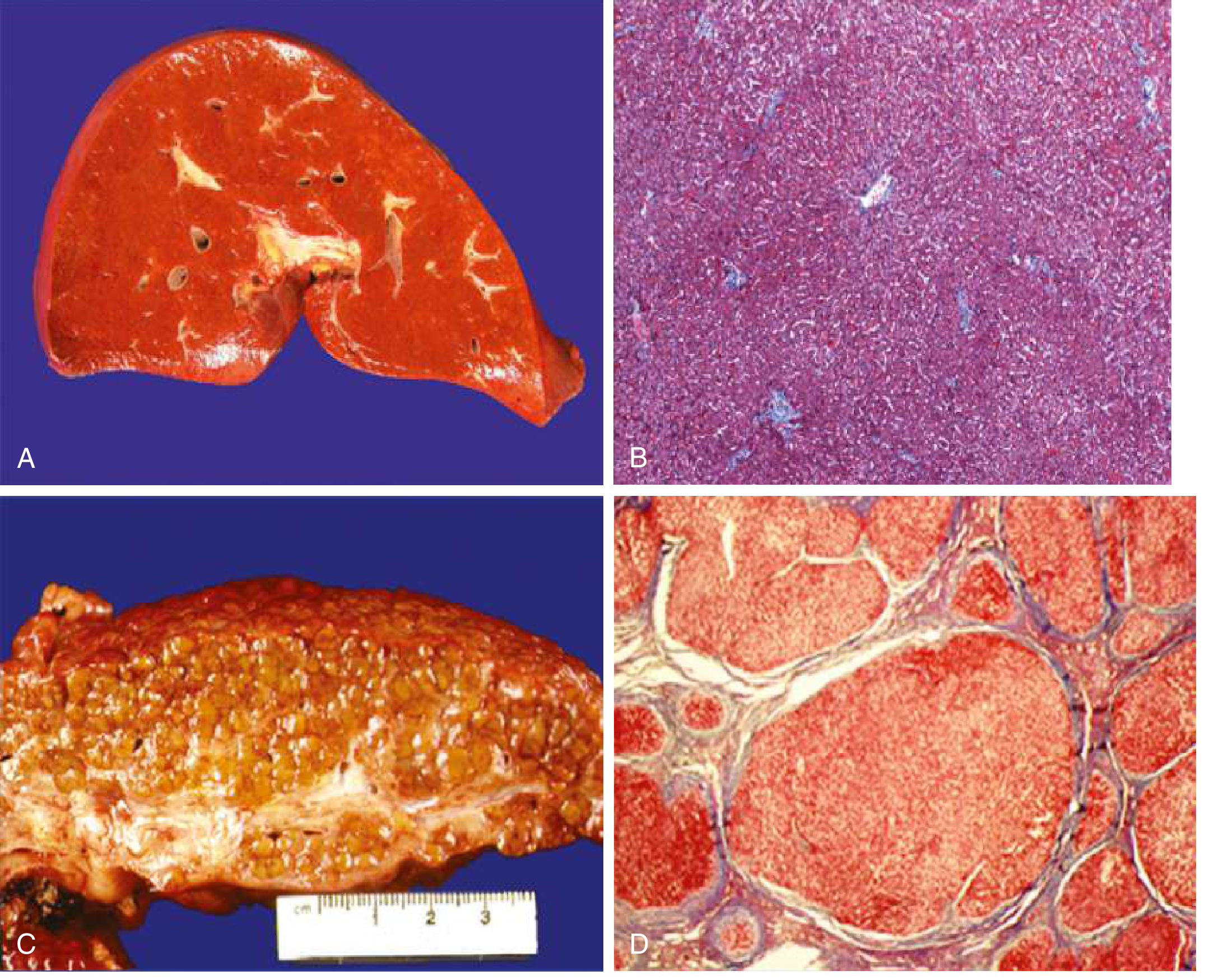
(A) Normal liver - smooth surface, homogeneous texture. (B) Normal hepatic sinusoids with organized architecture. (C) Cirrhotic liver - orange-tawny color, irregular nodular surface. (D) Microscopic cirrhosis - disorganized architecture with regenerative nodules surrounded by fibrous bands (Masson trichrome stain).
Etiology / Causes
Major Causes
| Cause | Notes |
|---|---|
| Alcoholic liver disease | Leading cause in Western countries |
| Non-alcoholic fatty liver disease (NAFLD/MASLD) | Increasingly prevalent globally |
| Chronic hepatitis B | Major cause worldwide |
| Chronic hepatitis C | Previously major; now largely treatable |
Other Causes (each ≤2% of cases)
-
Cholestatic/autoimmune: Primary biliary cirrhosis, primary sclerosing cholangitis, autoimmune hepatitis
-
Biliary obstruction: Mechanical obstruction, biliary atresia, cystic fibrosis
-
Metabolic: Hemochromatosis, Wilson disease, α1-antitrypsin deficiency, glycogen storage diseases, porphyria
-
Vascular: Budd-Chiari syndrome, veno-occlusive disease, right-sided heart failure
-
Cryptogenic cirrhosis: No identifiable cause
-
Goldman-Cecil Medicine, Table 139-1
Pathogenesis
Key Cellular Mechanism - Hepatic Stellate Cell Activation
- Hepatic stellate cells (Ito cells / perisinusoidal cells) reside in the space of Disse between hepatocytes and sinusoidal endothelial cells
- Normally quiescent - serve as the main vitamin A storage site
- In response to liver injury, they become activated:
- Lose vitamin A stores
- Proliferate
- Develop prominent rough ER
- Secrete extracellular matrix (collagen types I and III, sulfated proteoglycans, glycoproteins)
- Transform into contractile myofibroblasts
Sinusoidal Capillarization
-
Normal hepatic sinusoids lack a basement membrane and contain large fenestrae (100-200 nm), allowing passage of large molecules up to 250,000 daltons
-
Collagen deposition in the space of Disse causes defenestration ("capillarization" of sinusoids)
-
Alters plasma-hepatocyte exchange and reduces sinusoidal diameter (worsened by stellate cell contraction)
-
Goldman-Cecil Medicine, p. 1615
Morphology
Gross: The entire liver is transformed into regenerative parenchymal nodules separated by fibrous bands. The liver surface is nodular and irregular.
Microscopic: Nodular parenchyma surrounded by fibrous septa. The pattern of scarring (portal-portal vs. portal-central linking), degree of parenchymal loss, and extent of vascular thrombosis vary by etiology.
Ductular reactions: Stem cell activation gives rise to ductlike structures that increase with disease progression and are most prominent in cirrhosis.
Reversibility: Fibrosis and even established cirrhosis may partially regress after disease remission or cure. Scars become thinner, fragment, and adjacent nodules coalesce into larger islands.
Staging: Compensated vs. Decompensated
Cirrhosis is classified into two main prognostic stages:
| Stage | Definition | Prognosis |
|---|---|---|
| Compensated | No ascites, variceal hemorrhage, encephalopathy, or jaundice | Median survival >12 years |
| Decompensated | Development of any of the above | Median survival ~2 years |
Ascites is the most common first sign of decompensation (present in 80% of decompensated patients).
Scoring Systems
Child-Turcotte-Pugh (CTP) Score (Range 5-15)
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Ascites | None | Grade 1-2 (easy to treat) | Grade 3-4 (refractory) |
| Hepatic encephalopathy | None | Grade 1-2 | Grade 3-4 (spontaneous) |
| Bilirubin (mg/dL) | <2 | 2-3 | >3 |
| Albumin (g/dL) | >3.5 | 2.8-3.5 | <2.8 |
| PT (sec > control)/INR | <4 / <1.7 | 4-6 / 1.7-2.3 | >6 / >2.3 |
- Child A: Score 5-6 (well-compensated)
- Child B: Score 7-9
- Child C: Score 10-15 (severe decompensation)
MELD Score
Uses serum bilirubin, INR, and creatinine. Primary tool for liver transplant prioritization.
Complications (Pathophysiology)
The two main pathophysiologic consequences are portal hypertension and liver insufficiency.
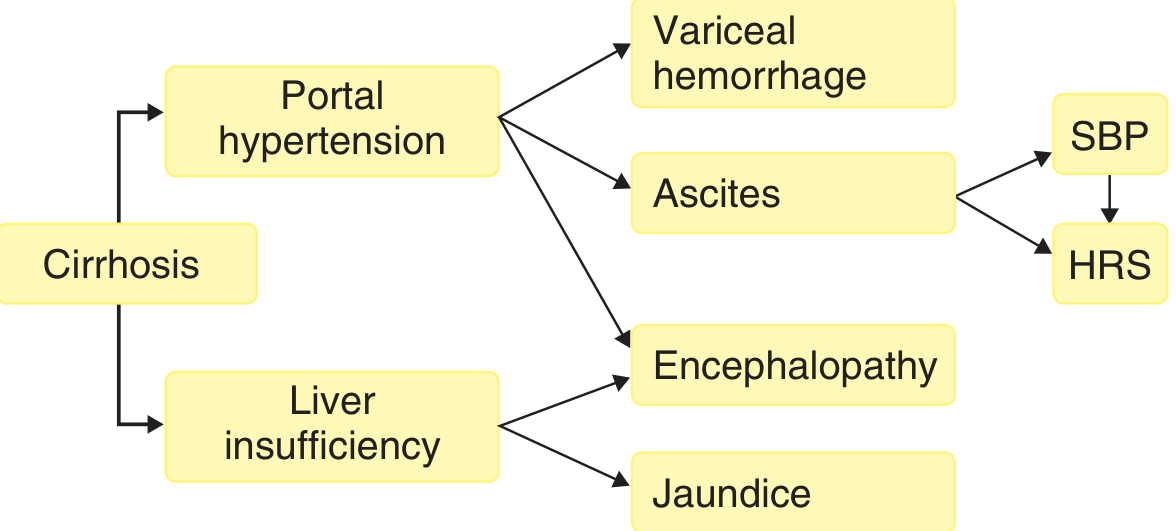
1. Portal Hypertension
Caused by:
- Fixed component: Fibrosis + regenerative nodule compression of sinusoids
- Functional component: Active vasoconstriction from intrahepatic nitric oxide deficiency + enhanced vasoconstrictors
Results in:
- Portosystemic shunts - most importantly, esophagogastric varices (develop in ~40% of advanced disease) - risk of massive fatal hematemesis
- Splenomegaly - can cause hypersplenism (thrombocytopenia, pancytopenia)
- Ascites - transudate (<3 g/dL protein); serum-ascites albumin gradient ≥1.1 g/dL; ~85% of all ascites cases are due to cirrhotic portal hypertension
2. Liver Insufficiency
- Jaundice - impaired bilirubin excretion
- Coagulopathy - reduced clotting factor synthesis
- Hypoalbuminemia - reduced plasma proteins → contributes to ascites and edema
- Hyperestrogenemia (in males) - impaired estrogen catabolism → palmar erythema, spider angiomas, gynecomastia, hypogonadism
- Hepatic encephalopathy - result of both portal shunting and liver insufficiency
3. Ascites Complications
- Spontaneous bacterial peritonitis (SBP)
- Hepatorenal syndrome (HRS) - functional renal failure
4. Renal Consequences (Guyton physiology)
- Reduced plasma protein → reduced colloid osmotic pressure → fluid leakage into peritoneum
- Portal hypertension impedes portal blood flow → raises capillary pressure in portal vascular bed
- Kidney retains salt and water (RAAS activation) in attempt to restore plasma volume
- Vascular capacity may actually increase (portal vein distension), worsening the cycle
5. Hepatocellular Carcinoma (HCC)
Most chronic liver diseases with cirrhosis predispose to HCC development.
Clinical Features
About 40% of individuals with cirrhosis are asymptomatic until advanced disease.
Symptoms
- Anorexia, weight loss, weakness (nonspecific)
- Pruritus - severe jaundice causes bile salt accumulation; may be severe enough to cause skin excoriation
- Abdominal distension (ascites)
Signs
| System | Finding |
|---|---|
| Skin | Jaundice, palmar erythema, spider angiomas, excoriations |
| Endocrine (males) | Gynecomastia, testicular atrophy, loss of body hair |
| Abdomen | Hepatomegaly (early), shrunken liver (late), splenomegaly, ascites, caput medusae |
| Neurological | Asterixis (hepatic flap), confusion (encephalopathy) |
| Hematologic | Bruising, bleeding (coagulopathy) |
Variceal Hemorrhage
- Gastroesophageal varices in ~50% of newly diagnosed cirrhosis
- Prevalence: 40% in Child A → 85% in Child C
- Varices develop/grow at 7-8% per year
- First bleed rate: ~5%/year (small varices), ~15%/year (medium/large varices)
- Risk factors for bleeding: large varices, severe liver disease, red wale markings
Laboratory Findings
| Test | Finding in Cirrhosis |
|---|---|
| Bilirubin | Elevated (conjugated + unconjugated) |
| ALT/AST | Elevated (may normalize in end-stage) |
| Albumin | Low |
| PT/INR | Prolonged |
| Platelets | Low (hypersplenism) |
| Sodium | May be low (dilutional hyponatremia, <130 mEq/L in ~25%) |
| Creatinine | Elevated if HRS develops |
Management Overview
Treat the Underlying Cause
- Alcohol cessation
- Antiviral therapy for hepatitis B (tenofovir/entecavir) or hepatitis C (direct-acting antivirals - cure possible even with established cirrhosis)
- Weight loss/metabolic control for NAFLD/MASLD
Compensated Cirrhosis
- Surveillance for varices (endoscopy) and HCC (ultrasound every 6 months)
- Non-selective beta-blockers (propranolol/carvedilol) for variceal prophylaxis if varices present
Decompensated Cirrhosis
| Complication | Management |
|---|---|
| Ascites | Salt restriction + diuretics (spironolactone ± furosemide); large-volume paracentesis for tense ascites + IV albumin |
| SBP | IV cefotaxime/ceftriaxone; prophylaxis with norfloxacin |
| Variceal hemorrhage | IV terlipressin or octreotide + endoscopic band ligation; TIPS if refractory |
| Hepatic encephalopathy | Lactulose ± rifaximin; identify and treat precipitants |
| HRS | Terlipressin + IV albumin; TIPS; ultimately liver transplant |
| Hyponatremia | Fluid restriction; vaptans in select cases |
Liver Transplantation
- Definitive treatment for end-stage disease
- MELD score used for waitlist prioritization
- 5-year survival post-transplant: ~75-80%
Prognosis
- Compensated: Median survival >12 years; decompensation develops at 5-7% per year
- Decompensated: Median survival ~2 years without transplant
- Leading causes of death: liver failure, HCC, variceal hemorrhage, sepsis
- Cirrhosis may partially regress if the underlying cause is eliminated (most dramatically seen after HCV cure or alcohol abstinence), though portal hypertension may persist due to irreversible shunts
Sources:
- Robbins & Kumar Basic Pathology, pp. 598-600
- Goldman-Cecil Medicine International Edition, pp. 1614-1620
- Guyton and Hall Textbook of Medical Physiology, p. 390
Cirrhosis liver
I just covered liver cirrhosis in detail in my previous response above. Here's a quick summary of what was covered:
Definition: Diffuse transformation of the liver into regenerative parenchymal nodules surrounded by fibrous bands - the end stage of chronic liver disease.
Key Topics Covered:
- Etiology (alcohol, NAFLD, hepatitis B/C, metabolic diseases)
- Pathogenesis (hepatic stellate cell activation, sinusoidal capillarization)
- Morphology with gross and microscopic images
- Compensated vs. decompensated staging
- Child-Turcotte-Pugh and MELD scoring
- Complications (portal hypertension, ascites, varices, encephalopathy, HRS, SBP, HCC)
- Clinical features and lab findings
- Management of each complication
- Prognosis
Is there a specific aspect of cirrhosis you'd like me to go deeper on? For example:
- Pathology - detailed histology, fibrosis grading
- Complications - management of ascites, varices, or hepatic encephalopathy in detail
- Scoring/prognosis - MELD score calculation, transplant criteria
- Specific etiology - alcoholic vs. viral vs. NAFLD cirrhosis
- Pharmacology - drugs used in management
Just let me know what you need!
This is a shared conversation. Sign in to Orris to start your own chat.