Notes on tubercolosis
Reading File
Finding Sources
Searching PubMed
"tuberculosis"[MeSH Terms] AND "treatment"[MeSH Terms]
Finding Sources
Searching PubMed
tuberculosis AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here are comprehensive notes on tuberculosis, compiled from authoritative medical textbooks:
Tuberculosis (TB) - Clinical Notes
1. Etiology and Transmission
- Caused by Mycobacterium tuberculosis (MTB), an aerobic, acid-fast bacillus
- Transmitted via airborne droplet nuclei from close contact with infectious patients (e.g., household contact with active pulmonary TB)
- Only ~5% of newly infected individuals develop significant disease; 95% are controlled by cell-mediated immunity
- Robbins & Kumar Basic Pathology; Textbook of Family Medicine 9e, p. 323
2. Epidemiology
- One of the most common causes of fatal respiratory infection worldwide
- 80% of cases come from 22 high-burden nations
- WHO estimated 8.8 million new cases/year; 1.7 million deaths attributed to TB
- TB in North America was rising in the 1980s but has been declining since 1992
- Multidrug-resistant (MDR) TB is a rising problem: 3% of newly diagnosed cases worldwide; 15% of previously treated cases
- High-risk groups: children, elderly, immunocompromised, HIV-positive, residents of long-term care facilities
- Textbook of Family Medicine 9e, p. 323–324
3. Pathogenesis
3a. Primary TB
- Occurs in a previously unexposed, unsensitized patient
- Inhaled bacilli implant in the distal air spaces of the lower part of the upper lobe or upper part of the lower lobe, close to the pleura
- A 1–1.5 cm gray-white consolidation develops - called the Ghon focus - with central caseous necrosis
- Bacilli travel via lymphatics to hilar/regional lymph nodes, which also caseate
- Ghon complex = parenchymal Ghon focus + involved lymph nodes
- After fibrosis and calcification = Ranke complex (visible on X-ray)
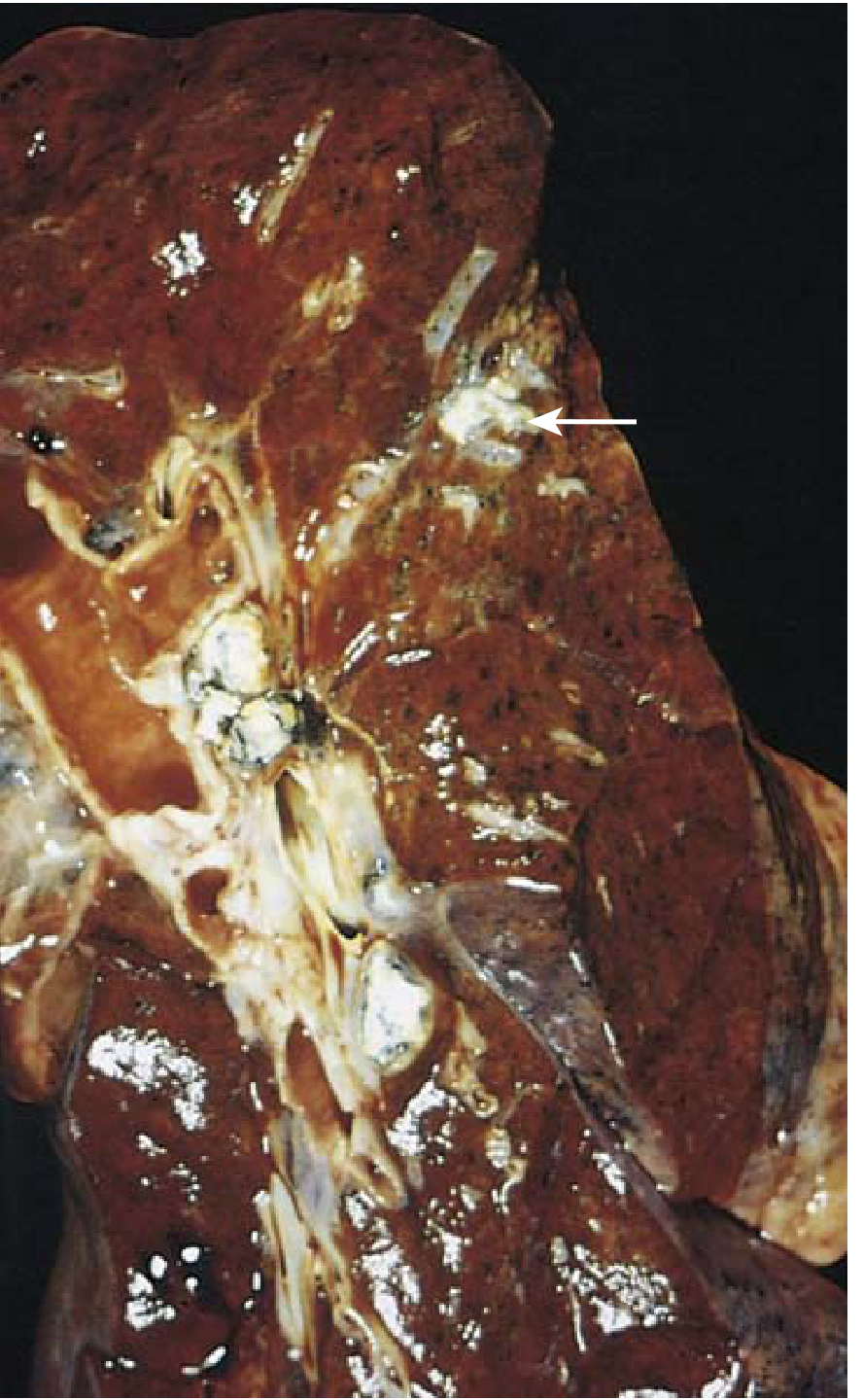
FIG. Primary pulmonary tuberculosis, Ghon complex. (Robbins & Kumar Basic Pathology)
- Cell-mediated immunity controls the infection in ~95% of cases
- Progressive primary TB occurs in overtly immunocompromised patients (especially HIV+ with CD4+ <200 cells/μL) - granulomas may be absent; sheets of macrophages packed with bacilli instead
3b. Secondary (Reactivation) TB
- Arises in a previously sensitized host - reactivation of dormant lesions (often decades later) or reinfection
- Classically localized to the apex of one or both upper lobes (possibly due to high O₂ tension)
- Preexisting hypersensitivity → prompt tissue response → walling off of focus
- Less lymph node involvement than primary, but cavitation is common and is a major source of infectivity
- HIV patients with mild immunosuppression (CD4 >300) present with apical cavitary disease; those severely immunocompromised (CD4 <200) present like progressive primary TB
- Robbins & Kumar Basic Pathology, pp. 476–477
3c. Histopathology
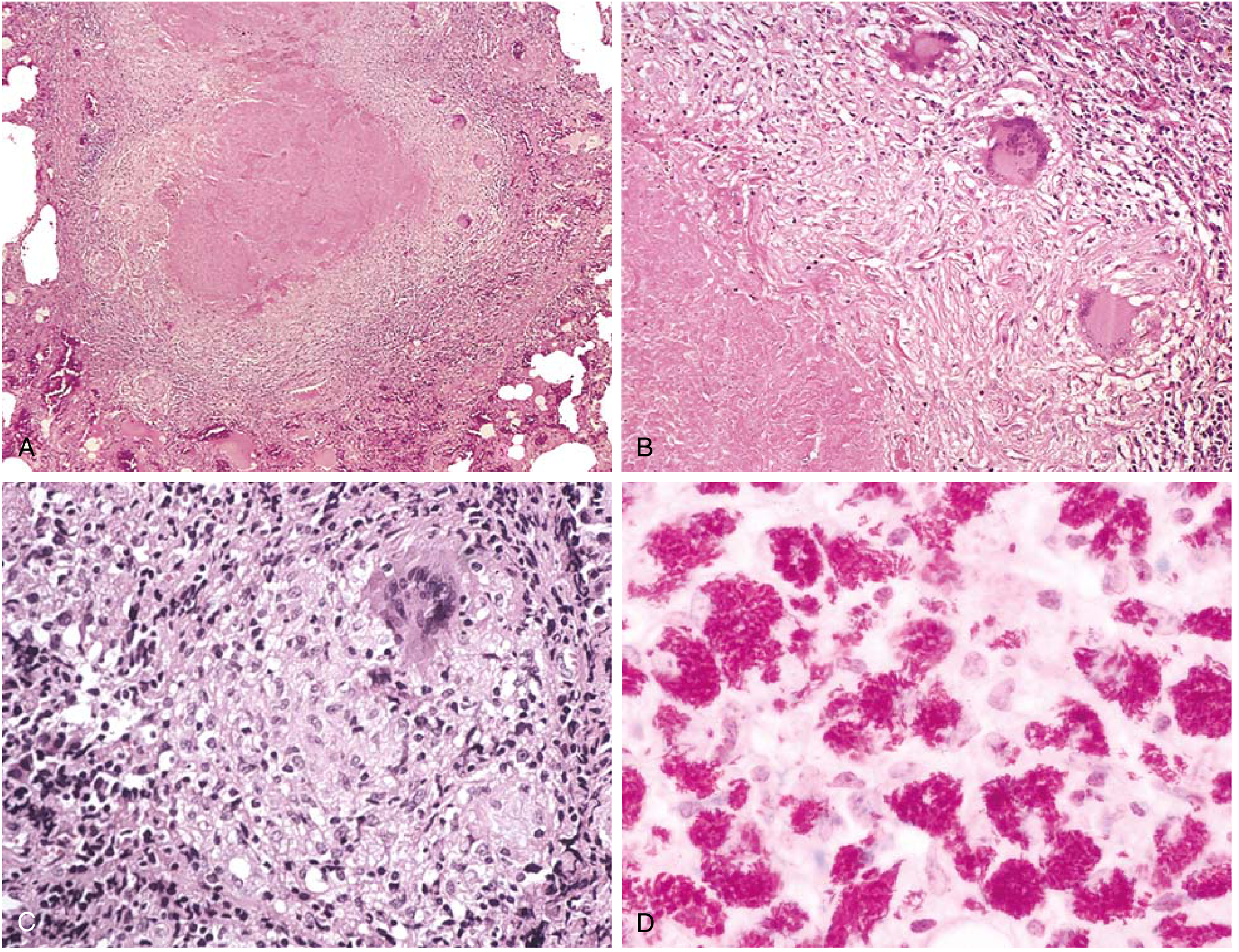
FIG. Morphologic spectrum of tuberculosis. (Robbins & Kumar Basic Pathology)
- Caseating granulomas with epithelioid macrophages and Langhans multinucleate giant cells = hallmark
- Even without central caseation, granulomas warrant acid-fast staining for mycobacteria
- Immunocompromised patients: granulomas may be absent - only sheets of macrophages with bacilli
3d. The Three-Population Model of Chemotherapy
MTB exists as three populations with differing metabolic activity:
- Actively multiplying extracellular bacilli - targeted by INH (greatest early bactericidal effect)
- Slowly multiplying in acidic compartments - targeted by PZA
- Sporadically multiplying bacilli - targeted by rifampin (sterilizing activity)
- Murray & Nadel's Textbook of Respiratory Medicine
4. Clinical Presentation
Pulmonary TB
- Cough, fever, dyspnea, night sweats, anorexia, weight loss, hemoptysis (in ~50%)
- Physical findings: wheezes, rales, signs of consolidation
- Sputum becomes purulent as cavitation occurs
- Low-grade remittent afternoon fever with night sweats is characteristic
Extrapulmonary TB (10–25% of cases worldwide)
- Disseminated (miliary) TB - lymphohematogenous spread; millet-seed granulomas in liver, spleen, bone marrow, adrenals, meninges, kidneys, fallopian tubes; more common in children and immunosuppressed
- "Serosal" TB - pleurisy, pericarditis, peritonitis, arthritis with effusion
- TB of solid organs - osteomyelitis, adrenal TB (Addison disease), renal TB
- TB lymphadenitis - most frequent extrapulmonary form; usually cervical ("scrofula")
- TB meningitis - most dangerous serosal form; can cause permanent brain damage; diagnosis difficult
- Pott disease - vertebral TB; paraspinal "cold" abscesses may present as abdominal/pelvic mass
- Intestinal TB - ileal involvement common; mucosal ulceration
- Textbook of Family Medicine 9e, pp. 297–298; Robbins & Kumar, p. 478
5. Diagnosis
Tuberculin Skin Test (TST / PPD)
Intradermal 5 tuberculin units (0.1 mL) PPD; read at 48–72 hours:
| Induration | Risk Group |
|---|---|
| >5 mm | HIV+ patients; recent contacts of active TB; fibrotic chest X-ray consistent with prior TB; organ transplant/immunosuppressed patients |
| >10 mm | Recent immigrants from high-prevalence countries; injection drug users; residents/employees of high-risk settings (prisons, nursing homes, hospitals, homeless shelters); mycobacteriology lab personnel; silicosis, DM, chronic renal failure, some hematologic disorders, weight loss >10%, gastrectomy, children <4 yr exposed to high-risk adults |
| >15 mm | Persons with no risk factors for TB |
- BCG-vaccinated patients can still be accurately tested with PPD
- PPD/TST is NOT recommended as routine screening in low-risk populations
Interferon-γ Release Assays (IGRAs)
- QuantiFERON-TB Gold (QFT) and T-SPOT.TB: single-time blood sample; greater specificity for MTB; no anamnestic response on repeat testing; no cross-reaction from BCG
- A positive QFT percentage >15 is moderately correlated with a positive TST in high-risk populations
Sputum Smear & Culture
- AFB smear (acid-fast staining or fluorescent auramine) - most common initial method
- Culture: takes 2–8 weeks standard; rapid methods (liquid media) detect growth in 5–14 days
- Cultures also essential for drug susceptibility testing (DST)
- In infants/young children: gastric aspirates (3 consecutive mornings) + sputum - only ~50% sensitivity
Molecular Tests (PCR / Xpert MTB/RIF)
- PCR sensitivity: 95–98% for smear-positive + culture-positive; 57–78% for smear-negative + culture-positive
- PCR on CSF: multiplex PCR has 94% sensitivity and 100% specificity for culture-confirmed TB meningitis (small series)
- Rapid molecular DST can detect rifampin resistance within hours and is strongly recommended for HIV+ patients
- Textbook of Family Medicine 9e, p. 324
6. Chest Radiograph Findings
| Pattern | Suggests |
|---|---|
| Upper lobe cavitary lesion | Reactivation (secondary) TB |
| Consolidation in apex of lower lobe / base of upper lobe | Primary TB |
| Miliary pattern (diffuse millet-seed nodules) | Disseminated TB |
| Hilar/mediastinal lymphadenopathy | Primary TB |
| Pleural effusion | TB pleuritis |
| Apical scarring / fibrocalcific nodules | Healed/old TB |
- HIV patients: findings may be atypical; chest X-ray occasionally normal
7. Latent TB Infection (LTBI)
- Defined by positive TST or IGRA without evidence of active disease
- Treatment options:
- Isoniazid (INH) x 6–9 months (standard; clinical hepatitis in ~0.6%)
- Rifampin x 4 months (effective alternative)
Rifampin + PZA x 2 months- no longer recommended due to increased liver toxicity
- Treatment indicated even in BCG-vaccinated patients and HIV co-infected patients
8. Treatment of Active TB
Standard 6-Month Regimen (Drug-Susceptible TB)
Intensive phase (2 months): INH + RIF + PZA + EMB
Continuation phase (4 months): INH + RIF
| Regimen | Intensive Phase | Continuation Phase | Notes |
|---|---|---|---|
| 1 (preferred) | INH RIF PZA EMB daily x 8 wk | INH RIF daily x 18 wk | Preferred for new pulmonary TB |
| 2 | INH RIF PZA EMB daily x 8 wk | INH RIF 3x/wk x 18 wk | When daily DOT is difficult |
| 3 | INH RIF PZA EMB 3x/wk x 8 wk | INH RIF 3x/wk x 18 wk | Caution in HIV/cavitary disease |
| 4 (lesser) | INH RIF PZA EMB daily x 2 wk then 2x/wk x 6 wk | INH RIF 2x/wk x 18 wk | Avoid in HIV or smear-positive/cavitary disease |
- Extended 9-month course indicated for: cavitary lesions OR persistent positive cultures at 2 months
- Repeat cultures after 2 months: 80% should be negative by then
- Daily dosing superior to twice-weekly in RCTs
- Treatment should be supervised by local/state health department
Drug Mechanisms
| Drug | Mechanism | Activity |
|---|---|---|
| INH | Prodrug (activated by KatG); inhibits mycolic acid synthesis | Bactericidal (concentration-dependent); greatest early bactericidal effect |
| Rifampin | Inhibits bacterial DNA-dependent RNA polymerase | Bactericidal; best sterilizing activity (slowly & sporadically multiplying bacilli) |
| PZA | Prodrug → pyrazinoic acid; inhibits fatty acid synthesis (multiple targets) | Bacteriostatic; effective in acidic environments; shortens treatment from 9 to 6 months |
| EMB | Inhibits arabinogalactan synthesis of mycobacterial cell wall | Bacteriostatic; protects against emergence of RIF resistance |
| Streptomycin | First effective anti-TB drug (1946); single-drug therapy leads to resistance | Historical; still used in MDR-TB regimens |
Directly Observed Therapy (DOT)
- Recommended for patients at high risk of treatment failure due to noncompliance
- RCTs have not clearly shown benefit over traditional public health strategies alone, but enhanced DOT with social supports and incentives is more effective
- WHO reports 82% treatment success rate worldwide
- Murray & Nadel's Textbook of Respiratory Medicine; Textbook of Family Medicine 9e, p. 325
9. Drug-Resistant TB
- MDR-TB: resistant to at least INH and RIF (the two most potent first-line drugs)
- Cause: inadequate or poorly administered regimens allow resistant mutants to become the dominant strain
- Treatment requires expert consultation and second-line agents (fluoroquinolones, bedaquiline, linezolid, etc.)
- DST should be performed on all previously treated TB patients
- Rapid molecular DST (Xpert MTB/RIF) can detect RIF resistance within hours
10. HIV and TB
- TB risk elevated at all stages of HIV disease
- CD4+ >300: typical secondary TB (apical, cavitary)
- CD4+ <200: resembles progressive primary TB (lower/middle lobe consolidation, hilar lymphadenopathy, noncavitary); extrapulmonary >50%
- Chest radiographic findings can be atypical or normal
- Rapid molecular DST strongly recommended for all HIV+ TB patients
- Pulmonary TB treated for 6 months regardless of HIV status
11. Prevention and Control
Infection Control (Four Categories)
- Clinician awareness and prompt, appropriate responses
- Administrative controls
- Environmental controls
- Personal protective equipment
BCG Vaccine
- Live attenuated Mycobacterium bovis
- Protection estimated at ~50% in meta-analyses
- Decreases severity of disease, especially in children (protective against miliary TB and meningitis)
- Widely used intradermally in high-burden countries
Contact Tracing
- In low-burden countries: evaluate contacts, treat highest-risk contacts for LTBI
- Community-wide Xpert screening in high-burden settings reduced TB prevalence by 44% in one cluster-randomized trial
- Murray & Nadel's Textbook of Respiratory Medicine
12. Key Summary Points
- 80% of TB comes from 22 high-burden nations
- Sputum cultures confirm diagnosis AND identify drug resistance; PCR provides faster results
- Latent infection (positive TST, normal CXR, asymptomatic): treat with INH x 6–9 months or RIF x 4 months
- Active pulmonary TB: RIPE x 2 months → IR x 4 months (total 6 months)
- Cavitary lesion or culture-positive at 2 months → extend to 9 months
- Extrapulmonary sites in order of frequency: lymph nodes > pleura > genitourinary > bone/joint > meningitis
- MDR-TB is defined by resistance to both INH and rifampin; requires expert management
Sources: Robbins & Kumar Basic Pathology; Textbook of Family Medicine 9e; Murray & Nadel's Textbook of Respiratory Medicine; Park's Textbook of Preventive and Social Medicine; Katzung's Basic and Clinical Pharmacology 16e
This is a shared conversation. Sign in to Orris to start your own chat.