teach me all about full mouth rehabilitation teachniches like hobos , twin stage when to use which and create decision making check list
Hobo twin stage technique full mouth rehabilitation occlusal vertical dimension
https://www.cureus.com/articles/158715-reclaiming-the-smile-…
full mouth rehabilitation techniques comparison Hobo Pankey Mann Schuyler Dawson decision making indications
https://pmc.ncbi.nlm.nih.gov/articles/PMC9709868
https://www.cureus.com/articles/219649-full-mouth-rehabilita…
"full mouth rehabilitation" AND "Hobo" AND occlusion
Full Mouth Rehabilitation (FMR) - Complete Guide
1. What Is Full Mouth Rehabilitation?
2. Indications for FMR
- Generalized tooth wear (attrition, erosion, abrasion, abfraction)
- Reduced Occlusal Vertical Dimension (OVD)
- Severely compromised aesthetics across both arches
- Multiple missing teeth with collapsed occlusion
- Amelogenesis imperfecta / dentinogenesis imperfecta
- Bruxism with extensive wear
- Trauma from occlusion causing periodontal damage
- Unacceptable function (tilted/over-erupted teeth disrupting occlusion)
- Lack of interocclusal space for individual restorations
3. Pre-Treatment Assessment Essentials
- Centric Relation (CR) - must be accurately recorded; mount study casts in CR
- Current OVD - measure with Willis gauge, Niswonger's method, or phonetics
- Freeway space (FWS) - normally 2-4 mm; if >4 mm, VDO can be increased
- Occlusal plane - evaluate using Broadrick's flag or Fox plane
- TMJ status - rule out active disc displacement, arthritis, or muscle pain
- Periodontal status - all active disease must be controlled before prosthodontic phase
- Diagnostic wax-up - mandatory; confirms space, aesthetics, and occlusal scheme
- Provisional restorations - test the new OVD and guidance for 4-8 weeks minimum
4. Turner & Missirlian Classification of Occlusal Wear (1984)
| Category | Description | Space Available |
|---|---|---|
| Category 1 | Excessive wear WITH loss of OVD | Yes - OVD must be restored |
| Category 2 | Excessive wear WITHOUT loss of OVD, but with space | Yes - space exists between CR and ICP |
| Category 3 | Excessive wear WITHOUT loss of OVD and WITHOUT space | No - most challenging; Dahl/reorganized approach needed |
5. The Major FMR Philosophies/Techniques
A. Hobo's Twin-Table Technique (Earlier Version)
B. Hobo & Takayama Twin-Stage Procedure (Main Technique)
Core Principle
- Condylar path and incisal path show deviation and are unreliable
- Cusp angle does NOT deviate - it is 4x more reliable
- A standard effective cusp angle is predetermined to ensure adequate posterior disclusion
- No need for pantograph or fully adjustable articulator
The Two Conditions (Stages)
- Anterior segment is removed from the cast
- Posterior teeth are waxed/restored using the standard cusp angle
- Cusp morphology is built to produce the standard amount of posterior disclusion
- Equal simultaneous contacts in centric; posterior disclusion in all eccentric movements
- Anterior segment is replaced onto the cast
- Anterior tooth morphology is established to create definitive disclusion
- Incisor contact in protrusion; canine contact on working side in lateral excursion
- The anterior guidance is harmonized with the pre-set posterior cusp angles
Occlusal Scheme
- Canine-guided occlusion (canine disclusion on working side)
- Posterior disclusion in ALL eccentric movements
- NO group function
- NO freedom in centric (unlike PMS)
Instrumentation Required
- Semi-adjustable articulator (e.g., Denar, Hanau)
- Facebow transfer
- CR record (any standard technique - leaf gauge, Lucia jig)
- Standard cusp angle table (provided by Hobo)
- NO pantograph required
Step-by-Step Clinical Procedure
- Thorough diagnosis + study casts mounted in CR
- Diagnostic wax-up to confirm new OVD and tooth form
- Provisional restorations - test for 4-8 weeks
- Confirm patient adaptation; adjust anteriors and posteriors in provisionals
- Prepare posterior teeth first (or one quadrant at a time)
- Fabricate posterior crowns using Condition 1 (standard cusp angle, no anterior guidance yet)
- Cement posterior restorations; verify contacts
- Prepare anterior teeth
- Establish anterior guidance using Condition 2 (harmonize with posterior cusp angles)
- Cement anterior restorations
- Final occlusal check and equilibration
Indications - Use Hobo Twin-Stage When:
- Turner-Missirlian Category 1 (loss of OVD; must restore VDO)
- Generalized attrition with reduced freeway space
- Amelogenesis imperfecta with VDO loss
- Patient has healthy periodontium (FGP cannot be used in weak periodontium, but Hobo can)
- Clinician wants a simpler, reproducible system without fully adjustable articulators
- Cases involving single crowns, FPDs, implants, or full arch reconstructions
- TMD patients (Hobo is suitable for TMD cases)
- When canine-guided occlusion is the goal
Contraindications:
- Severe skeletal malocclusion (Class II div 2, Class III) - standard cusp angles may not apply
- Severely abnormal Wilson curve or curve of Spee
- Abnormally tilted or rotated posterior teeth
- Cases where group function is mandated clinically
C. Pankey-Mann-Schuyler (PMS) Philosophy
Core Principle
- Based on Monson's spherical theory of occlusion (all teeth lie on an 8-inch sphere)
- Group function on the working side (canine + posterior teeth contact simultaneously)
- Long centric (freedom in centric) - essential feature
- Protrusive movement: only anterior teeth contact
PMS Sequence (The "Cross the Arch" Rule)
- Restore maxillary anterior teeth first - establish aesthetics, phonetics, incisal length
- Restore mandibular posterior teeth - using Broadrick occlusal plane analyzer
- Restore maxillary posterior teeth - using FGP technique against mandibular posteriors
- Restore mandibular anterior teeth last
FGP (Functionally Generated Path) Technique
- Wax is placed on the posterior crown preparations
- Patient performs functional movements (chew, slide, protrude)
- The opposing dentition carves the occlusal morphology directly into the wax
- This generates a "physiologically true" occlusal surface for that patient
- Limitation: wax can distort - significant potential for errors
Broadrick Occlusal Plane Analyzer
- Establishes the ideal curve of Spee for the mandibular arch
- Helps determine correct occlusal plane for mandibular posteriors
- Based on the 4-inch radius from condyle to occlusal plane
Indications - Use PMS When:
- Turner-Missirlian Category 2 (no OVD loss, space available between CR and ICP)
- Patient where group function is the desired or pre-existing occlusal scheme
- Cases where customized occlusal morphology via FGP is preferred
- When Broadrick occlusal plane analysis is needed to set posterior occlusal plane
- Cases with complex mandibular posterior needs
- When long centric is clinically indicated
Contraindications:
- Periodontally weak teeth - FGP cannot be accurately recorded on mobile teeth
- Cases requiring canine-protected occlusion
- When condylar path cannot be accurately recorded
- Active TMD or muscle dysfunction
D. Dawson's Approach (Centric Relation Based)
- Absolute foundation: all treatment planned from verified centric relation (bi-manual manipulation)
- Anteriors restored first to establish correct anterior guidance and phonetics
- Posteriors follow, with stable contacts in CR
- Diagnostic wax-up and provisionalization are non-negotiable
- Works well with most articulators
E. Gnathologic Approach
- Most precise but most demanding
- Uses fully adjustable articulator + pantograph for exact condylar recordings
- Canine-protected occlusion with immediate posterior disclusion
- Used for complex cases where condylar path deviation cannot be ignored
6. Comparison Table: Hobo Twin-Stage vs PMS
| Feature | Hobo Twin-Stage | PMS |
|---|---|---|
| Occlusal scheme | Canine-guided occlusion | Group function |
| Freedom in centric | No | Yes (long centric) |
| Condylar path recording | Not required | Required for FGP |
| Articulator needed | Semi-adjustable | Semi-adjustable |
| Pantograph | Not required | Not required |
| FGP technique | Not used | Central feature |
| Periodontal requirement | Healthy periodontium preferred but not mandatory | Requires stable, non-mobile teeth for FGP |
| OVD loss | Handles OVD loss well (Cat 1) | Better for Cat 2 (no OVD loss) |
| Posterior sequence | Posteriors first, then anteriors | Anteriors first, then posteriors |
| Learning curve | Simpler, more reproducible | Moderately complex |
| Error potential | Low (no wax FGP) | Higher (wax distortion in FGP) |
| TMD cases | Suitable | Less suitable during active TMD |
| OHRQoL outcome | Better pain/disability scores during tx | Better functional limitation + handicap scores overall |
7. Other Techniques Worth Knowing
| Technique | Key Feature | Best Use |
|---|---|---|
| Youdelis Scheme | Canine wear drops into group function automatically | Advanced periodontitis cases |
| Hobo Twin-Table | Original version; uses twin-table device | Predecessor to twin-stage; historical |
| BioJAK / Lucia Jig + Kois deprogrammer | Neuromuscular deprogramming first | High muscle hypertonicity/bruxism |
| Dahl Appliance / Localized Composite | Opens space by intrusion/extrusion (relative axial tooth movement) | Cat 3 (no space, no OVD loss) - minimally invasive |
8. Decision-Making Checklist
STEP 1 - Establish Diagnosis
- Identify cause of wear: attrition? erosion? abrasion? abfraction? mixed?
- Address etiology first (acid reflux, bruxism, diet)
- Complete periodontal charting - treat all active disease before prosthodontic phase
- TMJ evaluation - rule out active disc displacement, effusion, or myofascial pain
- Radiographic survey (FMX or CBCT if needed)
STEP 2 - Classify the Case (Turner-Missirlian)
- Is OVD reduced? Measure with Willis gauge + phonetic assessment
- What is freeway space? (Normal: 2-4 mm)
- Is there a CR-to-ICP slide? How large?
- Category 1 = OVD loss + adequate freeway space → restore OVD
- Category 2 = No OVD loss + space exists (CR-ICP slide) → use space without raising OVD, or raise minimally
- Category 3 = No OVD loss + no space → Dahl/localized approach first to create space
STEP 3 - Assess Occlusal Scheme
- Is existing occlusion canine-guided or group function?
- Is canine protected occlusion achievable (canine position, height adequate)?
- Is there skeletal malocclusion? (Class II Div 2, Class III - may preclude Hobo)
- Are posterior teeth normally angulated (no severe tipping or rotation)?
- Are curves of Spee and Wilson within normal limits?
STEP 4 - Assess Periodontal Foundation
- All pockets ≤3 mm (or stable with maintenance)?
- No pathological mobility?
- Adequate attached gingiva?
- Biologic width intact or corrected by crown lengthening?
- If mobility present → PMS/FGP is contraindicated; choose Hobo or Gnathologic approach
STEP 5 - Technique Selection
- Category 1 + healthy periodontium + canine guidance desired → Hobo Twin-Stage
- Category 2 + stable teeth + group function acceptable → PMS
- Category 3 + minimal intervention preferred → Dahl approach (composites/localized overlay)
- TMD present → Stabilization splint 4-12 weeks, then reassess; Hobo is preferred once stable
- Skeletal malocclusion → Orthodontic or surgical correction first, then reassess
- Fully edentulous arches involved → Complete denture prosthodontics principles apply
STEP 6 - Provisional Phase (Mandatory)
- Diagnostic wax-up completed?
- Provisionals fabricated at new OVD?
- Patient monitoring period: minimum 4-6 weeks; ideally 3 months for OVD changes >3 mm
- No muscle pain, TMJ pain, or speech issues during provisional phase?
- Phonetics acceptable (/s/ sound, /f/ and /v/ sounds, /m/ - freeway space check)?
- Patient satisfied with aesthetics at provisional stage?
STEP 7 - Final Restoration Sequencing
- Prepare and restore posterior teeth first (Condition 1 - without anterior guidance)
- Cement posteriors; verify equal contacts in CR
- Prepare and restore anterior teeth (Condition 2 - establish anterior guidance)
- Verify canine guidance on working side; anterior guidance in protrusion
- Confirm complete posterior disclusion in all eccentric movements
- Restore maxillary anteriors first (establish incisal edge position, aesthetics)
- Restore mandibular posteriors using Broadrick occlusal plane analyzer
- Restore maxillary posteriors using FGP technique
- Restore mandibular anteriors last
- Verify group function on working side; anterior contact in protrusion
STEP 8 - Final Occlusal Verification
- Equal simultaneous contacts in CR (shimstock check all quadrants)
- No deflective contacts in CR
- Correct guidance pattern (canine or group function per plan)
- All posterior teeth disclude in protrusion
- Balancing side free of contacts
- Check under magnification or T-scan if available
STEP 9 - Review and Maintenance
- Occlusal splint provided (especially for bruxers)?
- 1-week, 1-month, 3-month, 6-month review scheduled
- Periodontal maintenance ongoing every 3-4 months
- Patient instructions on occlusal splint use, diet, oral hygiene
9. Quick Reference: When to Use Which Technique
PATIENT PRESENTS WITH TOOTH WEAR
|
↓
Is OVD REDUCED?
| |
YES NO
| |
Cat 1 Is there CR-ICP slide / interocclusal space?
| | |
↓ YES (Cat 2) NO (Cat 3)
HOBO PMS DAHL / localized composite
Twin-Stage (if perio OK) (create space first)
OR HOBO
(if canine
guidance
preferred)
|
↓
Is there MALOCCLUSION or ABNORMAL TOOTH POSITION?
→ Orthodontics/Surgery FIRST, then reassess
Is there ACTIVE TMD?
→ Splint therapy first, then Hobo once stable
Is periodontium COMPROMISED (mobile teeth)?
→ Avoid PMS/FGP; use Hobo or Gnathologic approach
10. Key Concepts Summary
| Term | Definition |
|---|---|
| OVD (Occlusal Vertical Dimension) | Lower face height when teeth are in contact |
| Freeway space | Gap between teeth at rest position (OVD minus RVD); normal 2-4 mm |
| Centric Relation (CR) | Condyles in most superior, anterior position in glenoid fossa |
| Disclusion | Separation of posterior teeth during eccentric movements |
| Cusp angle | Angle of cusp incline to horizontal; Hobo's key variable |
| FGP | Functionally Generated Path - wax records patient's own eccentric movements |
| Broadrick's Analyzer | Establishes ideal occlusal plane radius for mandibular posteriors |
| Long centric | Horizontal freedom (0.5-1 mm) in centric - feature of PMS |
| Anterior guidance | Influence of anterior tooth contact on mandibular movement |
Create a decision-making flowchart poster for FMR technique selection
A professional clinical decision-making flowchart poster titled "Full Mouth Rehabilitation: Technique Selection Guide" for dental prosthodontics. Clean, medical/dental style with white background and color-coded decision boxes. Layout: vertical flowchart with branching paths START at top: Blue rounded rectangle "PATIENT WITH TOOTH WEAR - Begin FMR Assessment" Arrow down to: Orange diamond "STEP 1: Is OVD (Occlusal Vertical Dimension) REDUCED?" Two branches: LEFT branch (YES): Green box "Category 1 - OVD Loss Present - Freeway space available" RIGHT branch (NO): Purple diamond "Is there CR-ICP Slide or Interocclusal Space?" RIGHT branch splits: - YES → Teal box "Category 2 - No OVD loss but space exists" - NO → Red box "Category 3 - No OVD loss, NO space" From Category 1 → Diamond "Is periodontium healthy? Normal tooth angulation? No skeletal malocclusion?" - YES → HOBO TWIN-STAGE box (dark blue, bold): "★ HOBO TWIN-STAGE TECHNIQUE - Posterior first (Condition 1) then Anterior (Condition 2) - Canine-guided occlusion - Posterior disclusion in all eccentric movements" - NO → Orange box "Orthodontics/Surgery/Perio treatment FIRST → Reassess" From Category 2 → Diamond "Are teeth periodontally stable? (No mobility)" - YES → Split into two: PMS box (green, bold): "★ PMS TECHNIQUE - Maxillary anteriors first - Broadrick plane analyzer - FGP for posteriors - Group function occlusion" AND HOBO box (blue, smaller): "OR HOBO (if canine guidance preferred)" - NO → HOBO box only From Category 3 → Purple bold box: "★ DAHL APPROACH - Localized composite overlays - Create interocclusal space by relative axial tooth movement - Reassess after space created" Bottom section: Three colored side boxes side by side: - Red box: "⚠ ACTIVE TMD? → Splint therapy 4-12 weeks first → Then reassess with Hobo" - Yellow box: "⚠ ACTIVE PERIODONTAL DISEASE? → Complete perio treatment first → Recheck → Then proceed" - Orange box: "⚠ SKELETAL MALOCCLUSION? → Ortho/Orthognathic surgery first → Then FMR" Footer bar: Dark navy "MANDATORY FOR ALL CASES: Diagnostic wax-up → Provisionals (min 4-6 weeks) → Patient approval → Final restorations" Small legend bottom right showing color codes: Blue=Hobo, Green=PMS, Purple=Dahl, Orange=Prerequisites Title font large and bold at top. Professional dental poster style, clean lines, clear arrows with labels YES/NO on decision diamonds.
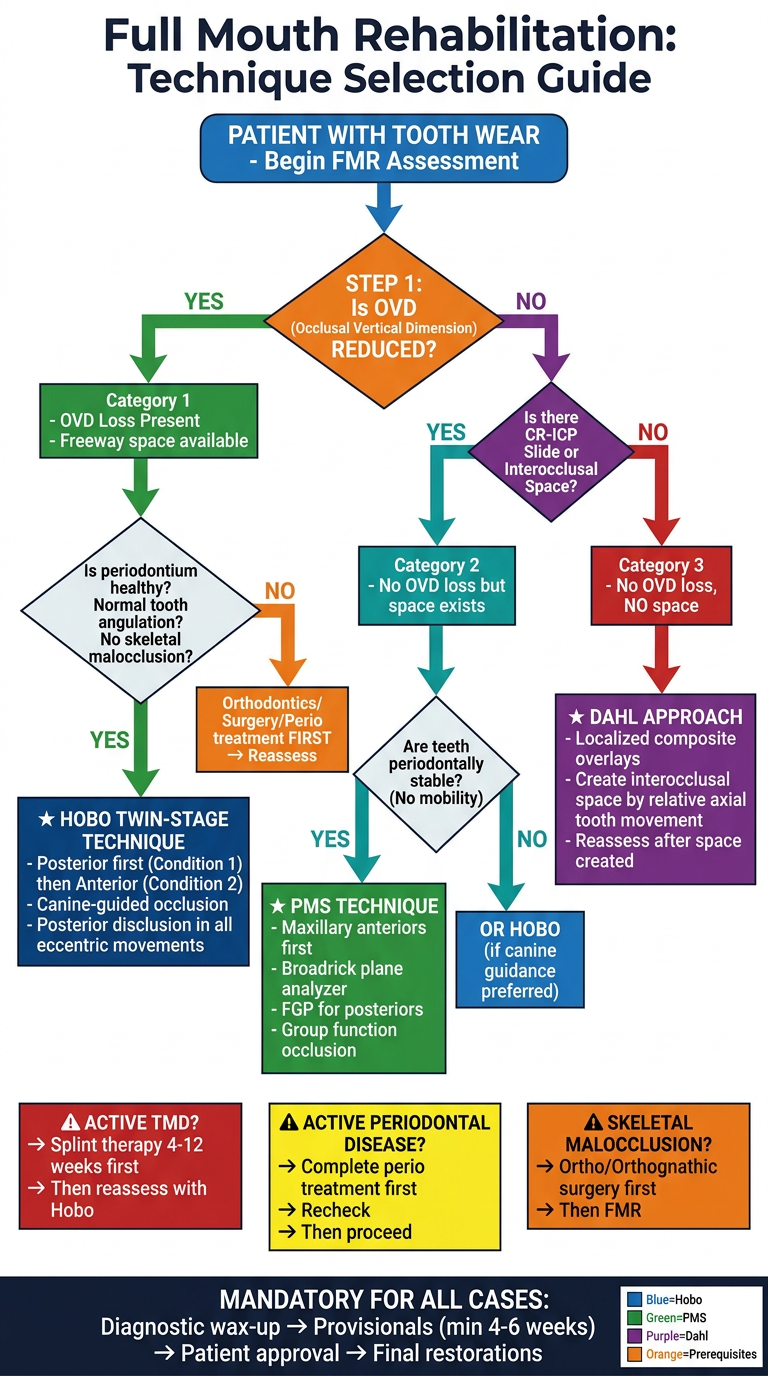
- Starting point - patient with tooth wear requiring FMR assessment
- Primary branch - OVD reduced or not (Turner-Missirlian classification)
- Three technique pathways:
- Hobo Twin-Stage for Category 1 (OVD loss) with healthy periodontium and normal tooth angulation
- PMS for Category 2 (space available, no OVD loss) with stable teeth - or Hobo if canine guidance is preferred
- Dahl Approach for Category 3 (no space, no OVD loss) to create interocclusal space first
- Three prerequisite flags for active TMD, active periodontal disease, and skeletal malocclusion - all requiring treatment before FMR
- Universal footer reminding that diagnostic wax-up and provisionalization are mandatory for every case regardless of technique