Lung abscess explain in detail
Reading File
Finding Sources
Searching PubMed
"lung abscess"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, detailed content from 6 authoritative textbooks. Let me compile the full detailed answer.
Lung Abscess - A Detailed Overview
Definition
A lung abscess is a localized area of suppuration (pus formation) and necrosis within the pulmonary parenchyma, resulting in the formation of one or more cavities, typically >2 cm in diameter. It represents the end result of microbial destruction of lung tissue.
- Harrison's Principles of Internal Medicine 22E, p. 1076
- Robbins & Kumar Basic Pathology, p. 512
Classification
| Type | Criteria |
|---|---|
| Primary (~80%) | Aspiration-related; arises in otherwise normal host; typically anaerobic |
| Secondary (~20%) | Underlying condition present - obstruction (tumor, foreign body), immunosuppression, septic emboli |
| Acute | Duration <4-6 weeks |
| Chronic | Duration >4-6 weeks (~40% of cases) |
| Putrid | Foul odor; strongly associated with anaerobic organisms |
- Fishman's Pulmonary Diseases and Disorders, p. 2242
- Tintinalli's Emergency Medicine, p. 491
Etiology and Predisposing Conditions
Risk Factors for Primary Abscess (Aspiration-driven)
The key predisposing condition is aspiration, particularly in:
- Altered mental status: alcoholism, drug overdose, seizures, anesthesia, coma
- Neuromuscular disease: bulbar dysfunction, prior stroke, cerebrovascular disease
- Esophageal pathology: dysmotility, strictures, tumors, gastroesophageal reflux
- Poor oral hygiene: gingivitis and periodontal disease are major risk factors - gingival crevices are colonized by anaerobes that serve as the bacterial source
- Recumbent positioning (hospital/nursing home patients)
Middle-aged men are more commonly affected than women. Lung abscesses are considered extremely rare in edentulous patients - the absence of teeth as a nidus for anaerobic colonization is highly protective.
- Harrison's Principles of Internal Medicine 22E, p. 1076-1077
- Fishman's Pulmonary Diseases and Disorders, p. 2242
Microbiology
| Clinical Setting | Key Pathogens |
|---|---|
| Primary abscess (aspiration) | Anaerobes: Peptostreptococcus spp., Prevotella spp., Bacteroides spp. (usually not B. fragilis), Fusobacterium spp., microaerophilic streptococci (Streptococcus milleri group) |
| Secondary abscess (immunocompromised) | S. aureus (MRSA/MSSA), P. aeruginosa, Klebsiella pneumoniae, Nocardia spp., Aspergillus spp., Cryptococcus spp. |
| Septic emboli | S. aureus (endocarditis), Fusobacterium necrophorum (Lemierre's syndrome) |
| Endemic/granulomatous | M. tuberculosis, Coccidioides spp., Histoplasma capsulatum, Blastomyces spp., parasites (Entamoeba histolytica, Paragonimus westermani, Echinococcus) |
| Nosocomial aspiration | Gram-negative organisms with hospital-acquired resistance |
Key microbiologic facts:
-
Anaerobes are recoverable in up to 93% of patients with lung abscess
-
In ~46% of cases, only anaerobes are isolated; in another 43%, a mixed anaerobic/aerobic flora is found
-
Metronidazole is not effective as a single agent because it does not cover microaerophilic streptococci, which are invariably part of the polymicrobial flora
-
Fishman's Pulmonary Diseases and Disorders, p. 2243
-
Murray & Nadel's Textbook of Respiratory Medicine
-
Harrison's Principles of Internal Medicine 22E, p. 1078
Pathogenesis
- Aspiration of oropharyngeal/gastric contents delivers a polymicrobial inoculum (including anaerobes) to dependent lung segments
- Initial pneumonitis/consolidation occurs in the dependent region
- Progressive tissue necrosis and suppuration from the combined effect of bacterial toxins, proteases, and the inflammatory response
- A cavity forms, usually within 1-2 weeks
- The cavity ruptures into an airway, creating partial drainage - produces an air-fluid level on imaging
- Surrounding lung develops fibrosis and scarring with chronic infection; cavity walls become thickened and eventually lined with regenerated epithelium
In pre-existing cavitary disease (e.g., emphysematous bullae, old TB cavities), infection may proceed without frank necrosis.
- Fishman's Pulmonary Diseases and Disorders, p. 2242
- Robbins & Kumar Basic Pathology, p. 512
Location and Morphology (Anatomy)
The location of abscesses is determined by the route of infection:
- Aspiration-related (most common): Posterior segment of the right upper lobe and the apical segments of the right lower lobe - the most dependent positions in the recumbent patient. Right-sided predominance reflects the more vertical orientation of the right main bronchus.
- Hematogenous/septic emboli: Multiple, bilateral, may affect any region
- Secondary to pneumonia/bronchiectasis: Multiple, basal, scattered
Size and gross appearance:
- Range from a few millimeters to 5-6 cm cavities
- When the cavity communicates with a bronchiole, an air-fluid level develops
- Rupture into the pleural cavity creates a bronchopleural fistula, empyema, or pneumothorax
Histology:
-
Central suppurative necrosis surrounded by granulation tissue and progressive fibrosis
-
In chronic abscesses, the cavity wall may become lined with regenerated bronchial-type epithelium (pseudomembrane)
-
Robbins & Kumar Basic Pathology, p. 512
-
Fishman's Pulmonary Diseases and Disorders, p. 2242
Clinical Features
Lung abscess typically follows an indolent course - patients present after 2-4 weeks of symptoms:
Symptoms
- Cough (productive or non-productive)
- Fever (may be low-grade; tachycardia and tachypnea are often absent given the slow progression)
- Pleuritic chest pain
- Hemoptysis
- Putrid/foul-smelling sputum - nearly diagnostic of anaerobic abscess
- Constitutional symptoms: night sweats, weight loss, fatigue, anemia (especially with anaerobic/chronic abscesses)
Physical Examination Findings
- Poor dentition / gingival disease (major clue)
- Amphoric or cavernous breath sounds on auscultation over the cavity
- Digital clubbing (chronic cases)
- Absent/diminished gag reflex
- Dullness to percussion over consolidation
Note: Abscesses caused by non-anaerobic organisms (S. aureus) may present with a more fulminant course - high fevers, rapid progression, and cavitation within a shorter timeframe.
- Harrison's Principles of Internal Medicine 22E, p. 1078
- Sabiston Textbook of Surgery, p. 2457
- Tintinalli's Emergency Medicine, p. 492
Diagnosis
Imaging
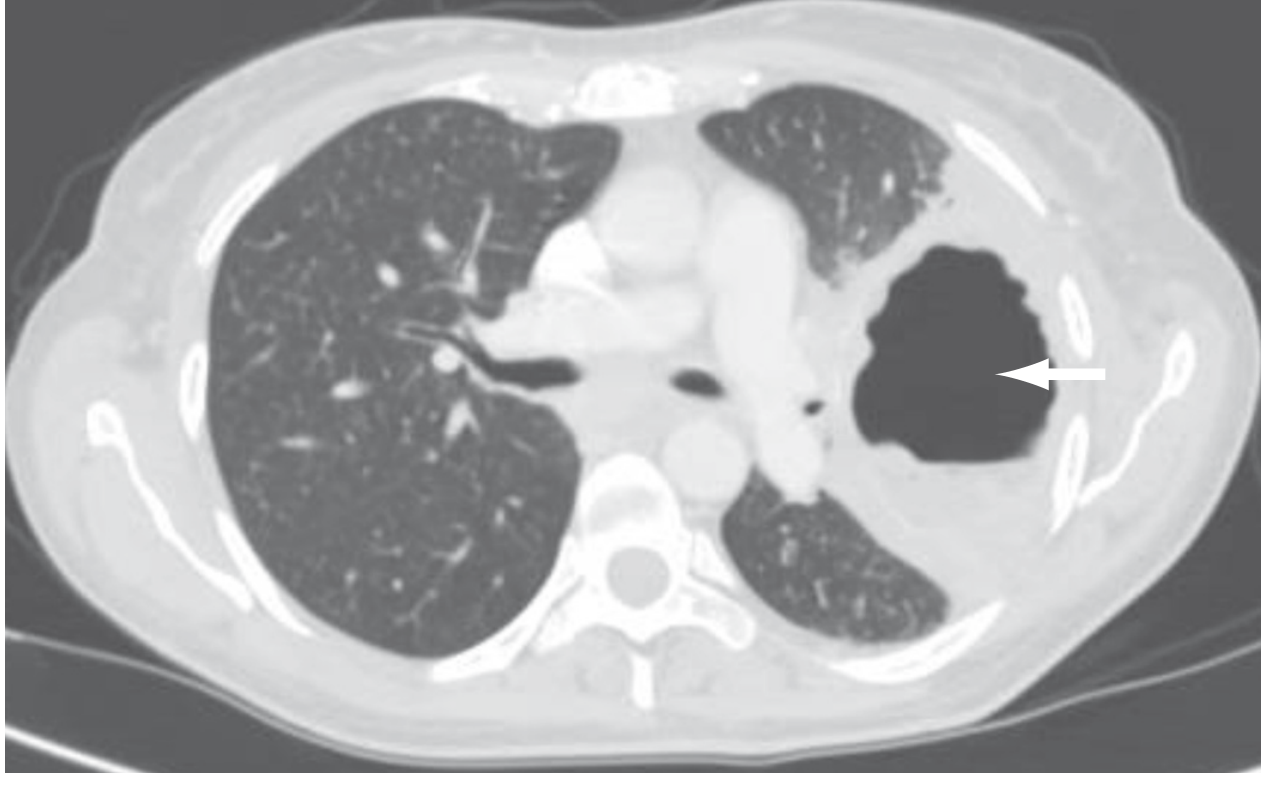
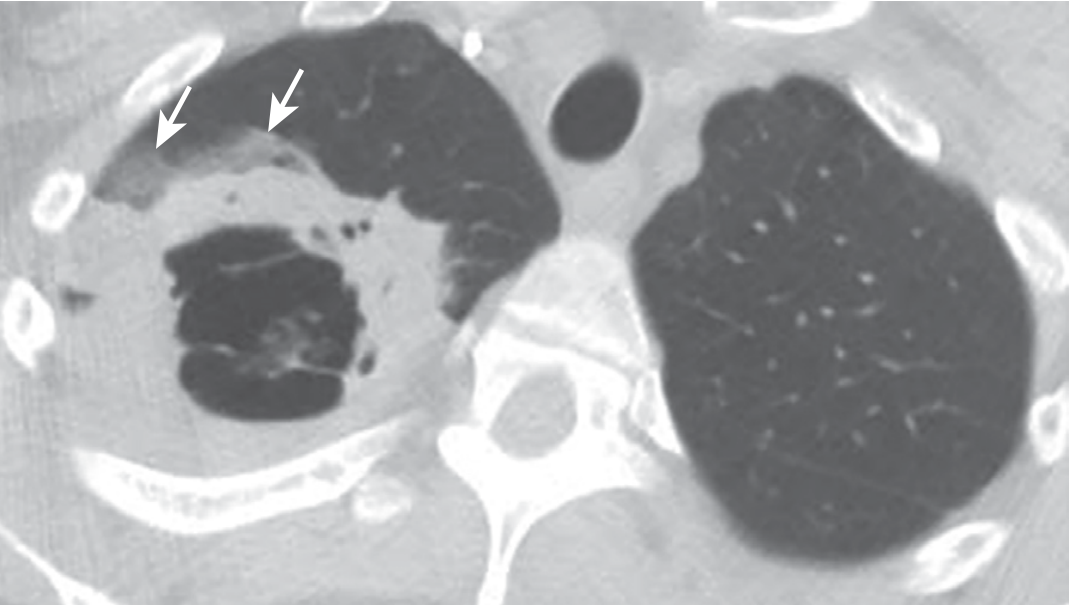
Chest X-ray (CXR):
- Thick-walled cavity with an air-fluid level (most classic finding - indicates communication with the bronchial tree)
- Dense consolidation or infiltrate in a dependent segment
- Single dominant lesion in right upper or lower lobe (aspiration-type)
CT Chest (preferred):
- Better anatomic definition; can detect cavitation earlier
- Distinguishes parenchymal abscess from pleural collection (empyema) - this distinction is critical because management differs completely
- Can identify underlying obstructing lesions (malignancy)
- Guides percutaneous drainage
Laboratory
- Leukocytosis (neutrophilia)
- Elevated inflammatory markers (CRP, ESR, procalcitonin)
- Anemia (chronic infection)
- Blood cultures (especially for hematogenous/secondary abscesses)
- Lab values are generally nonspecific
Microbiologic Workup
-
Sputum Gram stain and culture (non-invasive; limited by oral contamination; may not yield anaerobes)
-
Foul-smelling sputum is essentially diagnostic of anaerobic etiology
-
Bronchoscopy with protected brush specimen / BAL - for secondary/immunocompromised cases to target therapy; also to rule out obstructing lesion
-
Molecular diagnostics (16S rRNA gene amplification) - increasingly used for more precise pathogen identification
-
When no pathogen is isolated (~40% of primary abscesses), the abscess is termed a nonspecific lung abscess and anaerobes are presumed
-
Harrison's Principles of Internal Medicine 22E, p. 1079
-
Tintinalli's Emergency Medicine, p. 492
Differential Diagnosis of Cavitary Lung Lesion
| Category | Conditions |
|---|---|
| Infectious | TB, NTM (M. avium, M. kansasii), actinomycosis, nocardiosis, fungal (aspergillosis, histoplasmosis, coccidioidomycosis, mucormycosis), parasitic (Entamoeba, Echinococcus), infected bulla |
| Neoplastic | Bronchogenic carcinoma (squamous cell most commonly cavitates), metastatic cancer (colorectal, renal), lymphoma |
| Vascular | Pulmonary infarct, septic emboli (tricuspid endocarditis) |
| Inflammatory | Granulomatosis with polyangiitis (GPA/Wegener's), sarcoidosis, cryptogenic organizing pneumonia |
| Structural | Lung cysts/bullae with fluid, sequestration, bronchiectasis |
- Tintinalli's Emergency Medicine, p. 491 (Table 66-2)
- Harrison's Principles of Internal Medicine 22E, p. 1079
Treatment
1. Antibiotic Therapy (Primary Approach)
Empirical therapy should cover both strict anaerobes and facultatively anaerobic streptococci. Antibiotic therapy is continued until imaging shows complete resolution or reduction to a small scar.
| Agent | Dose | Notes |
|---|---|---|
| Ampicillin-sulbactam (preferred first-line) | 3 g IV q6h → oral amoxicillin-clavulanate once stable | Good anaerobic + streptococcal coverage |
| Clindamycin | 600 mg IV TID → 300 mg PO QID once stable | Alternative; superior to penicillin in clinical trials; avoid due to C. difficile risk |
| Carbapenem (imipenem, meropenem) | Standard IV dosing | Broad coverage; note meropenem monotherapy may lack streptococcal activity |
| Moxifloxacin | 400 mg PO daily | Small study showed equivalence to ampicillin-sulbactam |
Special situations:
- MSSA abscess (e.g., post-influenza): cefazolin, nafcillin, or oxacillin
- MRSA abscess: linezolid (preferred) or vancomycin; daptomycin is contraindicated (inactivated by lung surfactant - poor pulmonary bioavailability)
- Metronidazole alone is NOT adequate (misses microaerophilic streptococci)
Duration: 4-6 weeks on average; some sources recommend at least 6 weeks for better outcomes; continue until imaging shows resolution. Complex or secondary cases may require up to 14 weeks.
Expected response: Clinical improvement within 3-4 days, defervescence in 7-10 days with appropriate therapy.
2. Drainage
- Spontaneous drainage through the bronchial tree occurs in most patients - the development of an air-fluid level signals this
- Postural drainage (positioning) aids spontaneous drainage
- 85-95% of patients respond to medical management with cavity closure over 3-4 months
3. Bronchoscopy
- Indicated to exclude endobronchial obstruction (neoplasm, foreign body)
- Can be used for direct or transbronchial catheter drainage
- Risk: spillage of pus to unaffected lung
4. Percutaneous Drainage
Indications:
- Abscess >4 cm
- Peripherally located lesions
- Inadequate spontaneous drainage
- Failure of antibiotics (especially in poor surgical candidates)
Technique: CT or ultrasound guided; affected lung placed down to minimize spillage; daily saline irrigation; catheter removed once drainage stops and cavity shrinks
Success rate: ~84%; complication rate ~16% (hemoptysis, pneumothorax, hemothorax, bronchopleural fistula, catheter obstruction)
~11-21% of all lung abscesses require surgical or percutaneous drainage.
5. Surgical Resection
Indicated in approximately 10% of cases. Indications include:
- Persistent cavity ≥2 cm with thick walls after 8-12 weeks of medical therapy
- Failure to clear sepsis after 8 weeks
- Large cavity size (>6 cm)
- Life-threatening hemoptysis
- Bronchopleural fistula or empyema
- Suspected or confirmed obstructing malignancy
- Exclusion of cancer not possible by other means
Procedure: Lobectomy is preferred over segmentectomy (prevents incomplete removal and risk of reinfection). Video-assisted thoracoscopy (VATS) preferred for peripheral lesions without pleural adhesions. Double-lumen endotracheal tube used to protect the contralateral lung.
- Sabiston Textbook of Surgery, p. 2457
- Murray & Nadel's Textbook of Respiratory Medicine
- Tintinalli's Emergency Medicine, p. 492-493
- Harrison's Principles of Internal Medicine 22E, p. 1079-1080
Reasons for Medical Treatment Failure
- Bronchial obstruction (neoplasm, foreign body)
- Nonbacterial etiology (fungi, mycobacteria, vasculitis, pulmonary sequestration)
- Large cavity size (>6 cm)
- Empyema
- Resistant organisms
(Tintinalli's Emergency Medicine, Table 66-3)
Complications
| Complication | Notes |
|---|---|
| Empyema | Rupture of abscess into pleural space |
| Bronchopleural fistula | Communication between bronchial tree and pleural space |
| Hemoptysis | Bronchial arteries are the major source; minor hemoptysis is common; life-threatening hemoptysis is rare but may require emergent surgery |
| Pneumatoceles | Persistent cystic changes, especially with large cavities |
| Bronchiectasis | From local airway obstruction and recurrent infection |
| Mediastinitis | Rare; can follow surgical intervention |
| Brain abscess | CNS seeding via systemic circulation; lung abscess associated with brain abscess with OR 8.2 (95% CI 3.6-18.5) in a population-based study |
| Stroke | From clots/bacteria bypassing pulmonary filter |
| Massive aspiration | Flooding of airways with abscess contents |
| Recurrence | Despite adequate initial therapy |
- Murray & Nadel's Textbook of Respiratory Medicine
- Harrison's Principles of Internal Medicine 22E, p. 1080
Prognosis
| Factor | Mortality Impact |
|---|---|
| Primary abscess | 2-15% (antibiotic era) |
| Secondary abscess | Up to 75% in some series |
| Pre-antibiotic era | 32-34% regardless of treatment approach |
| Age >60 | Poor prognosis |
| Malignancy-related | High mortality |
| Aerobic bacteriology | Worse than anaerobic |
| Sepsis at presentation | Poor prognostic sign |
| Symptom duration >8 weeks | Worse outcomes |
| Abscess size >6 cm | Higher mortality; less likely to respond to antibiotics |
| Immunocompromised + obstruction + large abscess | Mortality up to 75% despite therapy |
Overall reported mortality: 1% to 38.2% in community-acquired lung abscess; secondary abscess mortality often >50%.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1157
- Tintinalli's Emergency Medicine, p. 491
- Harrison's Principles of Internal Medicine 22E, p. 1080
Prevention
- Minimize aspiration risk: head-of-bed elevation, careful sedation management, airway protection
- Optimize oral hygiene and treat periodontal disease
- Early mobilization of at-risk patients
- Pathogen-specific prophylaxis in at-risk immunosuppressed patients (e.g., antifungal prophylaxis post-transplant)
Recent Evidence Note (PubMed 2023-2026)
A 2025 review in FP Essentials (PMID: 40094493) covers current management approaches for lung abscess and pleural effusion in adults. Recent literature also highlights the role of next-generation sequencing for identifying unusual pathogens like Parvimonas micra (PMID: 39055980), particularly in culture-negative cases - this may shift future diagnostic workflows toward molecular methods over conventional cultures.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025)
- Robbins & Kumar Basic Pathology (Robbins Pathology)
- Sabiston Textbook of Surgery
- Murray & Nadel's Textbook of Respiratory Medicine
- Fishman's Pulmonary Diseases and Disorders
- Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.