Patient with watery stools a/w blood and mucous and abdominal cramps
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content. Let me compile the full clinical answer.
Watery Stools with Blood & Mucus + Abdominal Cramps - Clinical Approach
This triad - bloody/mucoid diarrhea + abdominal cramps - defines dysentery, which signals large bowel (colonic) inflammation. The key task is distinguishing infectious from non-infectious causes and identifying the specific pathogen.
Pathophysiology
Stools that contain blood or mucus indicate ulceration of the large bowel. Bloody stools in dysentery arise from mucosal invasion - organisms penetrate the colonic epithelium, trigger an inflammatory response, and cause mucosal abscesses, erosions, and the release of blood and mucus into the intestinal lumen.
- Harrison's Principles of Internal Medicine 22E, p. 1122
Differential Diagnosis
Infectious Causes (Most Common)
| Organism | Key Features |
|---|---|
| Shigella spp. | Most common bacterial cause; 1-3 day incubation; fever, cramps, bloody mucoid stools (dysentery); tenesmus; fecal-oral spread |
| Entamoeba histolytica | Protozoal; gradual onset; profuse bloody diarrhea, tenesmus; risk of hepatic abscess; endemic in developing countries |
| Campylobacter jejuni | Fever, bloody diarrhea; can mimic UC endoscopically; risk of reactive arthritis |
| Salmonella spp. | Fever, bloody diarrhea; zoonotic source (poultry, eggs) |
| EHEC (E. coli O157:H7) | Bloody diarrhea without fever; risk of HUS; Shiga toxin-producing; NO antibiotics |
| Yersinia enterocolitica | Bloody diarrhea with mucus, fever, RLQ pain (pseudoappendicitis) |
| Clostridioides difficile | Post-antibiotic use; watery/bloody diarrhea; pseudomembranous colitis |
- Goldman-Cecil Medicine, Table 285; Tintinalli's Emergency Medicine
Non-Infectious Causes
- Ulcerative Colitis (UC): Insidious or abrupt onset; bloody diarrhea, tenesmus, abdominal pain/fever; mucosal involvement; can flare after stopping smoking. Campylobacter and amebiasis can mimic UC endoscopically - stool studies are essential.
- Ischemic colitis: Sudden onset crampy LLQ pain with bloody diarrhea; usually older patients with vascular disease.
- Crohn's disease: Can present with bloody diarrhea but more commonly involves small bowel too.
Stages of Shigellosis (Prototype Dysentery)
From Goldman-Cecil Medicine, Table 285:
| Stage | Timing | Symptoms | Pathology |
|---|---|---|---|
| Prodrome | Earliest | Fever, chills, myalgias, anorexia | Early colitis, cytokine response |
| Watery diarrhea | 0-3 days | Loose stools, cramps, fever | Mild colitis with fecal leukocytes |
| Bloody diarrhea | 1-3 days | Frequent bloody mucoid stools, cramps, fever | Colitis with leukocytes and RBCs |
| Dysentery | 1-5 days | Frequent small-volume blood/mucus/pus stools, severe cramps, tenesmus | Extensive colitis, crypt abscesses, mucosal ulcerations |
| Acute complications | 3-7 days | Seizures, bacteremia, perforation, peritonitis | Severe colitis |
| S. dysenteriae type 1 complications | 3-7 days | Toxic megacolon, leukemoid reaction, HUS | Shiga toxin expression |
| Post-infectious | 1-3 weeks | Reactive arthritis (urethritis + conjunctivitis if HLA-B27+) | Autoimmune response |
Diagnostic Approach
Clinical algorithm (Harrison's 22E):
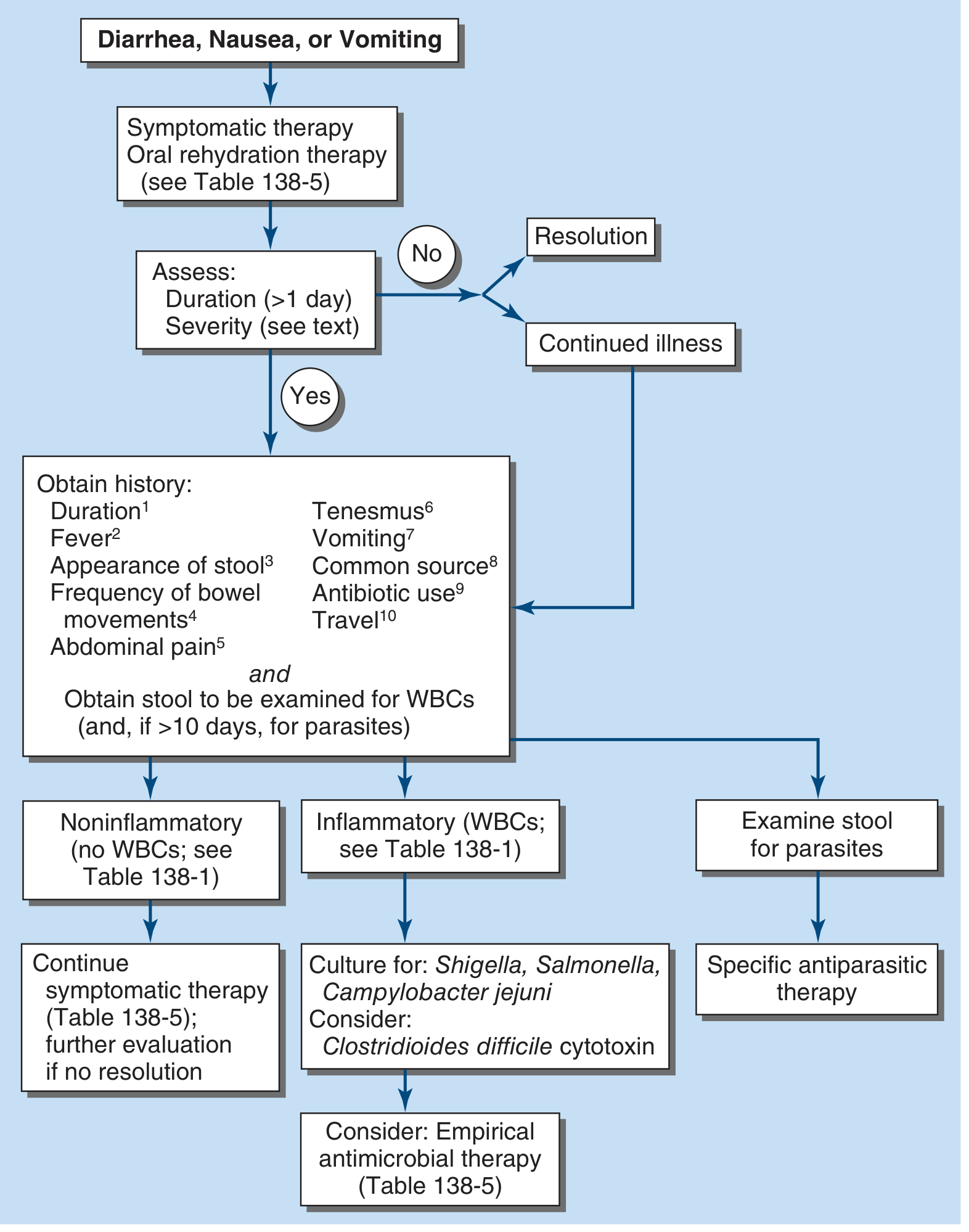
History key points to elicit:
- Duration (>1 day suggests further evaluation)
- Fever - implies invasive/inflammatory disease
- Stool appearance - blood/mucus = large bowel ulceration
- Tenesmus - suggests proctitis (Shigella, amebiasis)
- Recent antibiotic use - suggests C. difficile
- Travel history (traveler's diarrhea)
- Common source exposure (foodborne outbreak)
Stool Examination:
- Fecal leukocytes (methylene blue stain) - positive in inflammatory disease (Shigella, Campylobacter, C. diff)
- Stool microscopy for RBCs, cysts, trophozoites (E. histolytica - look for trophozoites with ingested RBCs)
- Stool culture: Shigella, Salmonella, Campylobacter jejuni
- PCR (stool): More sensitive than culture; preferred modern approach for Shigella
- C. difficile toxin assay (if recent antibiotic exposure)
- Rectal swab culture if stool culture not possible
If diarrhea >10 days: Examine specifically for parasites (E. histolytica, Giardia, Cryptosporidium).
- Harrison's Principles of Internal Medicine 22E, p. 1122
Management
Step 1: Assess Dehydration Severity
- Mild: Thirst, dry mouth, decreased urine output
- Moderate: Orthostatic hypotension, skin tenting, sunken eyes
- Severe: Lethargy, feeble pulse, hypotension, shock
Step 2: Rehydration
- ORS (Oral Rehydration Solution): First-line for mild-moderate dehydration
- IV fluids (glucose + saline): Reserved for severe dehydration or inability to tolerate oral intake
- Zinc sulfate 20 mg: Supplement with ORS - reduces duration of shigellosis
- Antimotility agents (e.g., loperamide): CONTRAINDICATED in dysentery - prolongs symptoms and bacterial shedding
Step 3: Antimicrobials
Shigella Dysentery:
| Setting | Drug | Dose |
|---|---|---|
| Adults (empirical) | Ciprofloxacin | 500 mg orally once daily × 3 days |
| Ciprofloxacin-resistant | Azithromycin | 500 mg twice daily × 1 day |
| Ciprofloxacin-resistant | Cefixime | 400 mg once daily × 3 days |
| Ciprofloxacin-resistant | TMP-SMX | 160/800 mg twice daily × 5 days |
| Severe/vomiting/unconscious | Ceftriaxone IV/IM | 1 g daily × 3 days (adults); 50-100 mg/kg/day × 3 days (children) |
| Children (1st line oral) | Ciprofloxacin | 15 mg/kg twice daily × 3 days |
Note: Antibiotics are routinely recommended for dysentery, severe illness, and immunocompromised patients. NOT routinely needed for non-febrile watery diarrhea.
- Goldman-Cecil Medicine (Shigellosis chapter), p. 3157
Amebic Dysentery (E. histolytica):
-
Metronidazole 750 mg every 8 hours (mixed amebicide of choice) - acts by forming cytotoxic compounds that bind to DNA and proteins of trophozoites
-
Always follow with a luminal amebicide (iodoquinol or paromomycin) to eliminate intestinal cysts and prevent relapse - combination provides >90% cure rates
-
Metronidazole alone leaves luminal cysts untreated
-
Rosen's Emergency Medicine; Lippincott Pharmacology
C. difficile:
- Stop offending antibiotic if possible
- Oral vancomycin or fidaxomicin (preferred over metronidazole for most cases)
EHEC (E. coli O157:H7):
- Antibiotics are contraindicated - increase risk of HUS by triggering Shiga toxin release
- Supportive care only
Red Flags Requiring Urgent Management
- High fever + toxic appearance
- Signs of dehydration/shock
- Rectal prolapse (especially in children with Shigella)
- Abdominal distension (toxic megacolon)
- Bloody diarrhea + oliguria/anuria/thrombocytopenia (HUS - especially with EHEC or S. dysenteriae type 1)
- Peritoneal signs (perforation)
Key Differentiating Points: Infectious vs UC
| Feature | Infectious Dysentery | Ulcerative Colitis |
|---|---|---|
| Onset | Acute | Chronic/relapsing |
| Fever | Common | Less prominent (unless severe) |
| Stool culture | Positive | Negative |
| Fecal leukocytes | Present | Present |
| Response to antibiotics | Yes (bacterial) | No |
| Endoscopy | Patchy ulcers | Continuous mucosal involvement from rectum |
Note: Campylobacter and amebiasis can produce endoscopic appearances identical to UC - stool cultures are essential before attributing symptoms to IBD.
- Goldman-Cecil Medicine, IBD chapter
This is a shared conversation. Sign in to Orris to start your own chat.