Teach me epilepsy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"epilepsy" AND "classification"
Reading File
Reading File
Finding Sources
Searching Images
epilepsy seizure classification types diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have everything needed for a comprehensive teaching response. Let me synthesize it all.
Epilepsy — A Comprehensive Overview
1. Definition
Epilepsy is a chronic neurological disorder defined by a predisposition to generate spontaneous, recurrent epileptic seizures. The ILAE 2014 practical definition requires:
- ≥2 unprovoked seizures >24 hours apart, or
- 1 unprovoked seizure with ≥60% probability of recurrence over the next 10 years (e.g., after a stroke, brain tumor, or abnormal EEG), or
- Diagnosis of an epilepsy syndrome
A seizure is a transient occurrence of signs/symptoms due to abnormal, excessive, or synchronous neuronal activity in the brain.
2. Epidemiology
- Prevalence: ~1–2% of the global population (~50 million people worldwide)
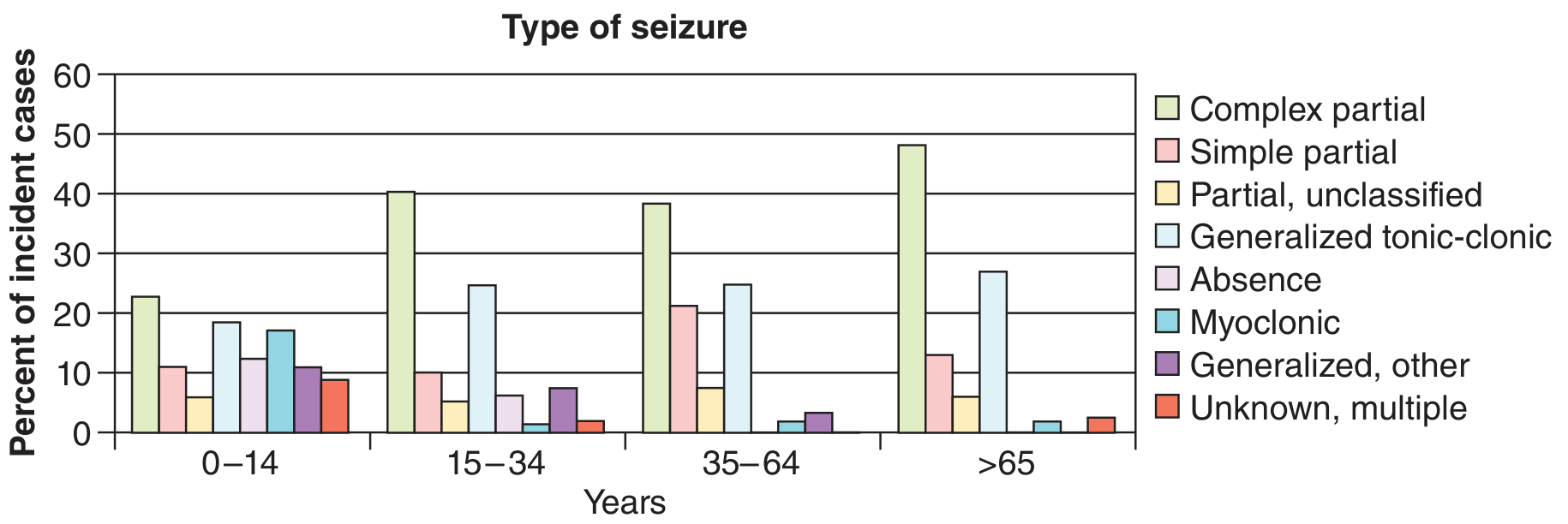
- Incidence is bimodal: peaks in early childhood and again after age 65
- ~70% of patients achieve seizure control with appropriate medications; ~30% are treatment-resistant
3. Etiology
Etiology categories (ILAE 2017):
| Category | Examples |
|---|---|
| Structural | Stroke, tumor, traumatic brain injury, cortical malformations, hippocampal sclerosis |
| Genetic | SCN1A (Dravet), KCNQ2, juvenile myoclonic epilepsy |
| Infectious | Neurocysticercosis, meningitis/encephalitis, HIV |
| Metabolic | Hypoglycemia, hyponatremia, pyridoxine deficiency |
| Immune | Autoimmune encephalitis (anti-NMDAR, LGI1, CASPR2) |
| Unknown | No identifiable cause after full workup |
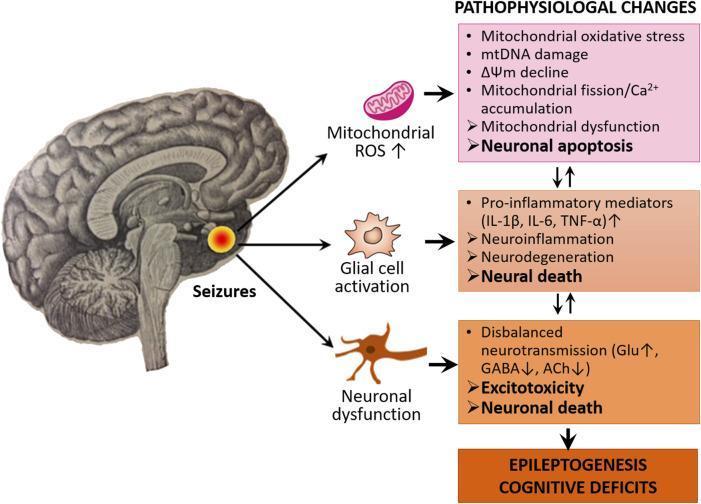
4. Pathophysiology
The core mechanism is an imbalance between excitatory (glutamatergic) and inhibitory (GABAergic) neurotransmission, resulting in abnormal synchronous neuronal firing.
At the cellular level:
- Ion channel dysfunction: Mutations in Na⁺, K⁺, Ca²⁺, and Cl⁻ channels alter neuronal excitability
- Burst firing: Neurons fire in high-frequency bursts (paroxysmal depolarization shifts, PDS) driven by voltage-gated Na⁺ and Ca²⁺ channels
- Loss of inhibition: Reduced GABA-A receptor function or GABAergic interneuron loss lowers the seizure threshold
- Excitotoxicity: Excess glutamate → excessive Ca²⁺ influx → neuronal injury
Epileptogenesis (the process of becoming epileptic):
After an initial brain insult (trauma, febrile seizure, stroke), a latent period of synaptic remodeling, mossy fiber sprouting, and neuroinflammation may transform normal brain into epileptic brain.
5. Classification (ILAE 2017)
Step 1 — Seizure Type
A. Focal Onset
Originate in one hemisphere. Subdivided by awareness:
- Focal aware (previously "simple partial"): Consciousness preserved; symptoms depend on focus location (motor, sensory, autonomic, psychic/aura)
- Focal impaired awareness (previously "complex partial"): Altered/lost awareness; often with automatisms (lip-smacking, hand-wringing)
- Focal to bilateral tonic-clonic: Focal onset that spreads to both hemispheres
B. Generalized Onset
Both hemispheres involved from onset — always impair consciousness:
| Type | Key Features |
|---|---|
| Tonic-clonic (grand mal) | Tonic phase (10–20 s rigidity, cyanosis, cry) → clonic phase (rhythmic jerks) → postictal confusion/sleep |
| Absence (petit mal) | 3–4 sec blank stare, subtle eye blinking; abrupt onset/offset; no postictal phase; 3 Hz spike-wave on EEG |
| Myoclonic | Brief, shock-like muscle jerks; often bilateral, no loss of consciousness |
| Tonic | Sudden muscle rigidity, no clonic phase |
| Atonic | Sudden loss of muscle tone → drop attack; high injury risk |
| Clonic | Rhythmic jerking without tonic phase |
C. Unknown Onset
Epileptic spasms (e.g., West syndrome in infants) fall here if onset is unclear.
Step 2 — Epilepsy Type
- Focal epilepsy (structural, immune, infectious, metabolic, genetic causes)
- Generalized epilepsy (largely genetic; associated with generalized spike-wave on EEG)
- Combined generalized and focal (e.g., Dravet syndrome)
- Unknown
Step 3 — Epilepsy Syndrome
A cluster of features (seizure type + EEG + imaging + age of onset + prognosis) that define a recognizable condition:
| Syndrome | Age | Key Features |
|---|---|---|
| West syndrome | Infancy | Infantile spasms, hypsarrhythmia EEG, intellectual disability |
| Dravet syndrome | Infancy | SCN1A mutation, febrile/prolonged seizures, cognitive decline |
| Childhood absence epilepsy | 4–12 yrs | Frequent brief absences, 3 Hz spike-wave, usually remits |
| Benign Rolandic epilepsy (BECTS) | 3–13 yrs | Centrotemporal spikes, nocturnal focal motor seizures, self-limited |
| Juvenile myoclonic epilepsy (JME) | Adolescence | Morning myoclonus, GTC seizures, lifelong |
| Lennox-Gastaut syndrome | Childhood | Multiple seizure types, slow spike-wave, severe intellectual disability |
| Temporal lobe epilepsy (TLE) | Any age | Focal impaired awareness, hippocampal sclerosis, most common drug-resistant epilepsy |
6. Clinical Presentation
Generalized Tonic-Clonic Seizure (GTCS) — the classic convulsion
- Prodrome (hours before, non-specific): mood change, irritability, myoclonic jerks on awakening
- Tonic phase (~10–20 s): sudden loss of consciousness; opisthotonos; vocalization ("epileptic cry"); cyanosis; pupils dilated and unreactive
- Clonic phase (~30 s): rhythmic, bilateral flexor spasms; autonomic surge (tachycardia, hypertension, salivation, sweating); possible tongue biting, urinary incontinence
- Postictal phase (minutes–hours): deep coma → confusion → drowsiness → headache; Todd's paralysis (transient focal weakness) may occur with focal onset
Temporal Lobe Seizure (most common focal seizure)
- Aura (focal aware portion): rising epigastric sensation (most common), déjà vu, fear, olfactory/gustatory hallucinations
- Impaired awareness phase: motionless stare, oro-alimentary automatisms (lip-smacking, chewing), hand automatisms
- Duration: 1–3 minutes
- Postictal confusion lasting minutes
Absence Seizure
- Abrupt onset: blank stare, subtle eyelid fluttering, cessation of activity
- Lasts 3–30 seconds; patient resumes immediately with no postictal period
- Can occur dozens to hundreds of times per day
- EEG: classic 3 Hz generalized spike-and-wave
7. EEG
The EEG is the most important diagnostic test. Key findings:
- Interictal epileptiform discharges (IEDs): spikes and sharp waves — present in ~90% of epilepsy patients on repeated EEGs (only ~2% of non-epileptic people show these)
- Ictal recording: capturing a seizure is the gold standard
- Photoparoxysmal response: generalized spike-wave triggered by photic stimulation (photosensitive epilepsy)
- Absence EEG: 3 Hz spike-wave with abrupt onset/offset
- Hypsarrhythmia: chaotic high-amplitude multi-focal spikes in West syndrome
- Normal interictal EEG does NOT exclude epilepsy
— Bradley & Daroff's Neurology in Clinical Practice
8. Diagnosis & Workup
| Test | Purpose |
|---|---|
| EEG (routine ± sleep-deprived) | Confirm epileptiform activity, classify seizure type |
| MRI brain (structural protocol) | Identify structural cause (hippocampal sclerosis, tumor, dysplasia) |
| Labs | Glucose, Na⁺, Ca²⁺, Mg²⁺, CBC, LFTs, toxicology |
| Prolonged video-EEG monitoring | Gold standard for pre-surgical evaluation; capture ictal event |
| Genetic testing | If onset in infancy or suspected genetic syndrome |
| Autoimmune panel | Anti-NMDAR, LGI1, CASPR2, GABA-B if autoimmune suspected |
| Lumbar puncture | If meningitis/encephalitis suspected |
First seizure evaluation: Rule out acute symptomatic causes (provoked seizures — do NOT require AED treatment); identify underlying etiology.
9. Antiepileptic Drugs (AEDs)
General Principles
- Start with monotherapy; ~50% of patients become seizure-free on first agent
- If first drug fails (efficacy or tolerability), try a second monotherapy
- After two adequate drug trials fail → drug-resistant epilepsy
- Drug choice depends on seizure/syndrome type, sex, age, comorbidities, teratogenicity
Major Drugs by Mechanism
| Drug | Mechanism | Indications | Key Limitations |
|---|---|---|---|
| Valproate | Na⁺ channel, GABA potentiation, NMDA inhibition, T-type Ca²⁺ channel | Broad-spectrum: focal, generalized, absence, JME | Teratogenicity (neural tube defects), weight gain, hepatotoxicity, PCOS; avoid in women of childbearing age |
| Phenytoin/Fosphenytoin | Na⁺ channel inhibitor | Focal and generalized; IV for status epilepticus | Nonlinear (saturable) pharmacokinetics, enzyme inducer, gingival hyperplasia, hirsutism, skin hypersensitivity (SJS) |
| Carbamazepine | Na⁺ channel inhibitor | Focal seizures, TLE | Enzyme inducer, hyponatremia, SJS (especially HLA-B*1502 in Asian patients), not for generalized epilepsy |
| Levetiracetam | SV2A (synaptic vesicle protein) binding | Broad-spectrum adjunctive | Behavioral side effects (irritability, aggression) |
| Lamotrigine | Na⁺ channel, glutamate release inhibition | Focal and generalized; safe in pregnancy | Slow titration required; SJS risk; reduced by enzyme inducers, doubled by valproate |
| Ethosuximide | T-type Ca²⁺ channel inhibitor | Absence seizures only | Narrow spectrum |
| Oxcarbazepine | Na⁺ channel inhibitor | Focal seizures | Less enzyme induction than carbamazepine; hyponatremia |
| Lacosamide | Na⁺ channel (slow inactivation enhancer) | Focal seizures | PR interval prolongation |
| Topiramate | Multiple: Na⁺ channel, GABA-A, AMPA/kainate inhibition | Focal, generalized; migraine prophylaxis | Cognitive dulling ("dope-a-max"), kidney stones, weight loss |
| Phenobarbital | GABA-A potentiation | Broad-spectrum; neonatal seizures; status epilepticus | Sedation, enzyme inducer, dependence |
| Perampanel | AMPA receptor antagonist | Focal and generalized (adjunctive) | Psychiatric side effects |
— Adams & Victor's Principles of Neurology, 12th ed., Table 15-5
Treatment-Resistant Epilepsy
~30% of patients fail to respond to adequate trials of ≥2 AEDs. Options:
- Ketogenic diet (especially children with Lennox-Gastaut, Dravet)
- Vagus nerve stimulation (VNS) — ~50% seizure reduction
- Surgical resection (best results: temporal lobectomy → 64% seizure-free)
- Responsive neurostimulation (RNS), deep brain stimulation (DBS)
10. Status Epilepticus (SE)
Definition: Seizure activity without return to baseline:
- GTCS: ≥5 minutes (previously 30 min, but brain injury begins earlier)
- Focal impaired awareness SE: ≥10 minutes
Most common cause: Acute brain insult in a person without epilepsy (also: AED non-compliance, autoimmune encephalitis, metabolic derangements)
Management (stepwise)
| Time | Stage | Treatment |
|---|---|---|
| 0–5 min | Premonitory | Airway, IV access, glucose, labs |
| 5–20 min | Early SE | Benzodiazepines: lorazepam 0.1 mg/kg IV, OR IM midazolam 10 mg (preferred prehospital); diazepam 5–10 mg IV |
| 20–40 min | Established SE | Second line: fosphenytoin 15–20 mg/kg, OR valproate 30–40 mg/kg, OR levetiracetam 30–60 mg/kg |
| >40 min | Refractory SE | ICU: continuous midazolam 0.1–0.4 mg/kg/h, propofol 1–3 mg/kg/h, pentobarbital 0.5–3 mg/kg/h; EEG monitoring |
— Goldman-Cecil Medicine, International Edition
11. Special Situations
Febrile Seizures
- Most common neurologic disorder in children < 5 years (4% incidence)
- Simple: brief, generalized, single episode per febrile illness; benign, minimal future risk
- Complex: focal, prolonged (>15 min), or repeated in one illness → increased risk of later epilepsy
- Temperature typically >38°C; herpesvirus 6 is a common trigger
- Prophylactic AEDs are NOT recommended for simple febrile seizures
Women with Epilepsy
- Catamenial epilepsy: seizure clustering around menstruation due to estrogen/progesterone fluctuations
- Valproate causes neural tube defects (risk ~1–2% if taken in first trimester), polycystic ovary syndrome, and intellectual disability in offspring — avoid in women of childbearing age
- Lamotrigine and levetiracetam are preferred in pregnancy
- Enzyme-inducing AEDs reduce efficacy of hormonal contraceptives
Driving and Social Restrictions
Patients must be seizure-free (jurisdiction-dependent, typically 3–12 months) before driving. Complete seizure control removes restrictions; physicians may have mandatory reporting obligations.
12. Prognosis
- ~70% achieve seizure freedom with medications
- ~50% of newly diagnosed epilepsy patients respond to the first AED
- Adding a second AED after first failure yields ~15% additional response
- After two drug failures: only ~5% respond to additional drugs → surgery should be considered
- ~65% of surgical candidates achieve long-term seizure freedom after resection
- Epilepsy carries a ~2–3× increased risk of premature death (SUDEP — sudden unexpected death in epilepsy; risk ~1/1000 per year)
Key Points Summary
| Concept | High-Yield Fact |
|---|---|
| 3 Hz spike-wave | Childhood absence epilepsy |
| Temporal lobe sclerosis | Most common cause of drug-resistant focal epilepsy |
| JME | Morning myoclonus + GTC; lifelong; valproate first-line (unless female) |
| Status epilepticus | ≥5 min GTCS; Rx: benzos → fosphenytoin/valproate/LEV → ICU sedation |
| Febrile seizure | Benign if simple; complex febrile seizures → increased epilepsy risk |
| AED + pregnancy | Avoid valproate; prefer lamotrigine or levetiracetam |
| Drug-resistant epilepsy | Failure of ≥2 adequate AED trials → surgery evaluation |
| SUDEP | Leading cause of death in young epilepsy patients; ~1/1000/year |
Primary sources: Adams & Victor's Principles of Neurology, 12th ed.; Bradley & Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.