Carcinoid tumor pathology
Reading File
Finding Sources
Finding Sources
Searching PubMed
carcinoid tumor neuroendocrine pathology
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the full answer.
Carcinoid Tumor Pathology
Definition and Terminology
Carcinoid tumors are well-differentiated neuroendocrine neoplasms (NETs) arising from neuroendocrine cells distributed throughout multiple organs, primarily the GI tract, lungs, and bronchi. The term "carcinoid" (literally "carcinoma-like") was coined because these tumors grow more slowly than true carcinomas. The current WHO classification designates them as low- or intermediate-grade neuroendocrine tumors; high-grade variants are termed neuroendocrine carcinoma and histologically resemble small cell carcinoma of the lung.
- Robbins & Kumar Basic Pathology, p. 560
- Harrison's Principles of Internal Medicine 22E
Cell of Origin
Carcinoids arise from enterochromaffin (APUD) cells distributed in the GI tract, lung, ovary, and pancreas. These cells produce a variety of vasoactive hormones including serotonin, histamine, dopamine, kallikrein, bradykinin, and tachykinins.
- Yamada's Textbook of Gastroenterology, 7th ed.
- Maingot's Abdominal Operations
Epidemiology
- Peak incidence is in the sixth decade, though any age can be affected.
- >40% occur in the small intestine (most commonly ileum).
- The tracheobronchial tree and lungs are the next most common sites.
- Rectal NETs show striking geographic variation: up to 14% of all NETs in Europe vs. up to 90% in some Asian series.
Gross Pathology
- Appear as intramural or submucosal masses, forming small polypoid lesions.
- Grossly yellow or tan in color.
- Elicit an intense desmoplastic reaction that can cause kinking of the bowel and obstruction.
Histopathology
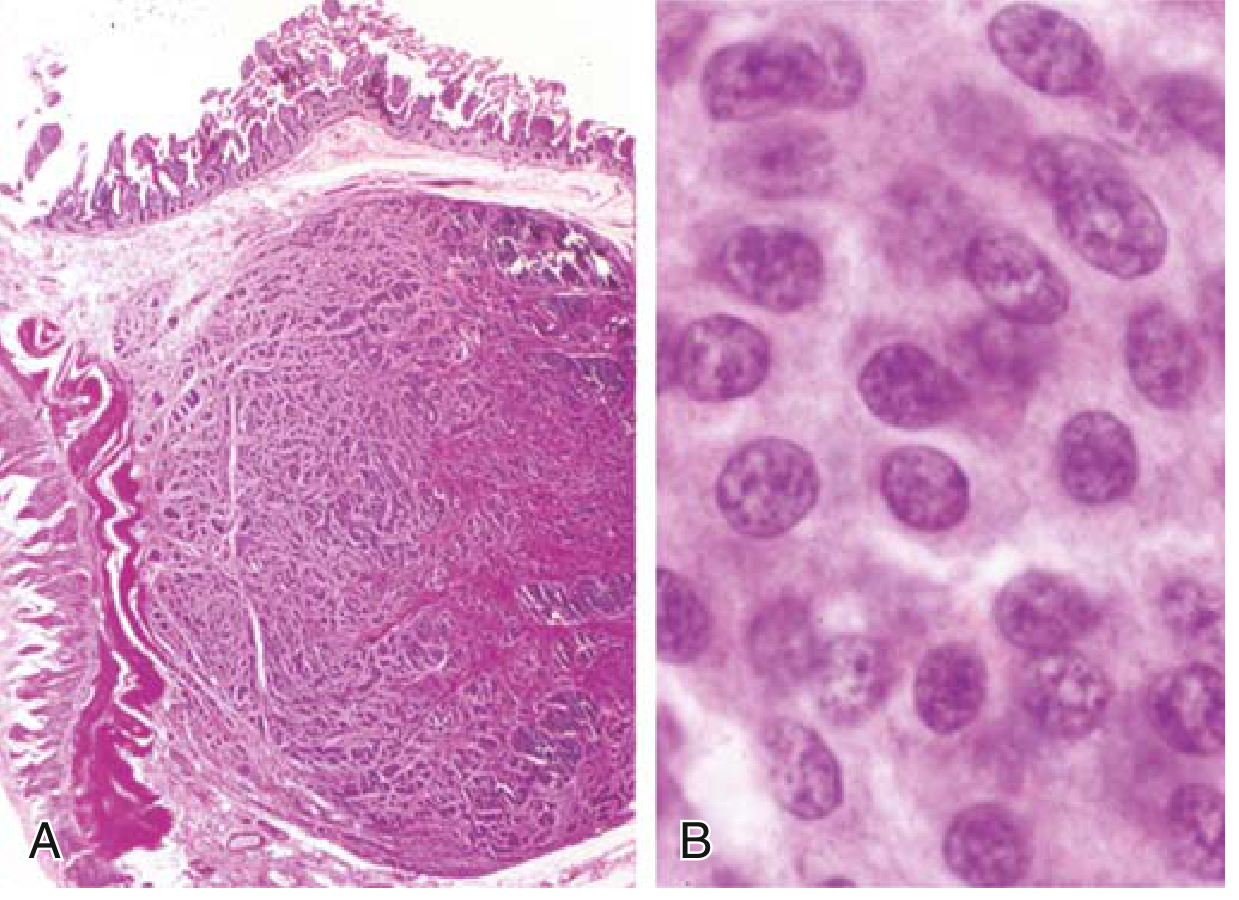
(A) Low power: submucosal nodule of tumor cells embedded in dense fibrous tissue.
(B) High power: bland uniform cells with scant pink granular cytoplasm and round-to-oval nuclei showing the classic "salt-and-pepper" chromatin pattern (fine and coarse clumps).
Architectural patterns include islands, trabeculae, strands, glands, or sheets of monomorphic cells with minimal atypia. Mitotic figures are scarce in well-differentiated tumors.
- Robbins & Kumar Basic Pathology, p. 560
WHO Grading (GI NETs)
| Grade | Mitotic rate | Ki-67 index |
|---|---|---|
| G1 (low) | <2/10 HPF | <3% |
| G2 (intermediate) | 2-20/10 HPF | 3-20% |
| G3 (high) / Neuroendocrine carcinoma | >20/10 HPF | >20% |
The 2021 WHO classification for pulmonary NETs includes: typical carcinoid, atypical carcinoid, large cell neuroendocrine carcinoma, and small-cell carcinoma. - Fishman's Pulmonary Diseases and Disorders
Immunohistochemistry
- Chromogranin A - widely used marker; elevated in metastatic disease (though not highly specific).
- Synaptophysin - another neuroendocrine marker.
- Hormone products (serotonin, gastrin, glucagon, somatostatin) depending on tumor type.
Location-Based Behavior (Most Important Prognostic Factor)
| Location | Behavior |
|---|---|
| Foregut (stomach, duodenum proximal to ligament of Treitz, esophagus) | Rarely metastasize; generally cured by resection. May produce gastrin (Zollinger-Ellison syndrome). |
| Midgut (jejunum, ileum) | Often multiple; tend to be aggressive. Depth of invasion, size, and necrosis/mitoses predict outcome. |
| Hindgut (appendix, colorectum) | Usually discovered incidentally. Appendiceal tumors: almost uniformly benign course. Rectal tumors: metastasis uncommon if small (<1 cm). |
- Robbins & Kumar Basic Pathology, p. 560-561
- Harrison's Principles of Internal Medicine 22E
Carcinoid Syndrome
Occurs in <10% of patients - only when vasoactive substances bypass the liver's first-pass metabolism, typically in hepatic metastatic disease or retroperitoneal lesions.
Clinical features:
- Cutaneous flushing - sudden-onset, deep red or violaceous erythema of the face and neck, lasting 2-5 min initially, later hours
- Diarrhea - watery, can be >10 episodes/day
- Bronchospasm / wheezing
- Colicky abdominal pain
- Right-sided cardiac valvular fibrosis (carcinoid heart disease)
Mediators: The main product is serotonin (5-HT). Up to 50% of dietary tryptophan is diverted into serotonin synthesis by tumor cells - this can cause niacin (pellagra-like) deficiency. Other mediators include histamine, tachykinins (substance P), kallikrein, and bradykinin.
Diagnosis: Elevated urinary 5-HIAA (24-hour collection) - the serotonin metabolite. False positives can occur with serotonin-rich foods (salmon, eggs).
- Harrison's Principles of Internal Medicine 22E, p. 725
- Robbins & Kumar Basic Pathology
Carcinoid Heart Disease (Hedinger Syndrome)
-
Occurs in patients with carcinoid syndrome (chronic serotonin excess).
-
Glistening white, plaque-like endocardial thickenings on right-sided cardiac chambers and valves.
-
Histology: smooth muscle cells embedded in an acid mucopolysaccharide-rich matrix with sparse collagen.
-
Predominant right-sided involvement: tricuspid insufficiency + pulmonic stenosis (left side is spared because lungs inactivate serotonin before it reaches the left heart).
-
In carcinoid syndrome patients, 70% of dietary tryptophan is converted to serotonin (vs. 1% normally).
-
Comparable lesions are seen with fenfluramine and ergot alkaloids, both of which affect serotonin metabolism or bind 5-HT receptors on valves.
-
Robbins & Kumar Basic Pathology, p. 379
Imaging and Localization
- CT/MRI - primary modalities; liver metastases from carcinoids are typically hypervascular.
- 68Ga-DOTATATE PET - highly sensitive for both primary NETs and metastases; exploits the fact that >90% of NETs express somatostatin receptors.
- FDG-PET - often negative in well-differentiated NETs (low metabolic activity); more useful for high-grade tumors.
- Angiographic findings of mesenteric involvement: retraction, kinking, and occlusion of mesenteric arteries.
Carcinoid Crisis
A potentially life-threatening complication occurring spontaneously or precipitated by hepatic artery embolization. Manifestations include sudden flushing, sweating, hypotension or hypertension, and cardiac arrest. Octreotide (Sandostatin) is used both prophylactically and for emergency management. - Yamada's Textbook of Gastroenterology, 7th ed.
Treatment Highlights
- Resection is curative for localized disease.
- Somatostatin analogs (octreotide, lanreotide): block release of serotonin and other bioactive peptides; prevent flushing in 20-30% of cases; also have antiproliferative effects.
- Telotristat ethyl: inhibits tryptophan hydroxylase (the rate-limiting enzyme in serotonin synthesis); used for refractory carcinoid syndrome diarrhea.
- 68Ga-DOTATATE-guided PRRT (peptide receptor radionuclide therapy) for metastatic disease.
- Hepatic artery chemoembolization for liver-dominant metastases with carcinoid syndrome.
Key summary points:
- Well-differentiated NETs with "salt-and-pepper" nuclear chromatin, pink granular cytoplasm, in islands/trabeculae.
- Most common in small intestine; appendiceal tumors are almost always benign.
- Carcinoid syndrome requires hepatic metastases to bypass first-pass metabolism.
- Right-sided carcinoid heart disease is mediated by chronic serotonin excess.
- Diagnose with urinary 5-HIAA; image with 68Ga-DOTATATE PET.
Carcinoid tumor pathology definition pathogenisis clinical features , morphology
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
I now have all the content needed for a focused, well-structured answer on definition, pathogenesis, clinical features, and morphology. Let me compose the final response.
Carcinoid Tumor - Complete Pathology
1. Definition
A carcinoid tumor (now formally termed a well-differentiated neuroendocrine tumor / NET) is a neoplasm arising from neuroendocrine cells (specifically enterochromaffin/APUD cells) distributed throughout many organs - predominantly the gastrointestinal tract, but also the lungs, bronchi, ovary, and pancreas.
The term "carcinoid" (meaning "carcinoma-like") was coined because these tumors grow more slowly than carcinomas. The current WHO classification calls them:
- Low-grade (G1) or Intermediate-grade (G2) neuroendocrine tumors for well-differentiated forms
- Neuroendocrine carcinoma (G3) for high-grade variants that histologically resemble small cell carcinoma of the lung
More than 40% of all carcinoid tumors occur in the small intestine. The tracheobronchial tree and lungs are the next most common sites.
- Robbins & Kumar Basic Pathology, p. 560
2. Pathogenesis
Cell of Origin
Carcinoids arise from enterochromaffin (EC) cells and related APUD cells. These cells are part of the diffuse neuroendocrine system and possess:
- Dense-core neurosecretory granules containing biogenic amines
- The ability to perform amine precursor uptake and decarboxylation (APUD)
Hormonal Drive to Hyperplasia
In some settings, hormonal stimulation triggers neuroendocrine cell hyperplasia that precedes tumor formation. A classic example:
- Autoimmune gastritis → achlorhydria → hypergastrinemia → ECL (enterochromaffin-like) cell hyperplasia → gastric carcinoid tumors
Serotonin Synthesis Pathway (Key Pathogenetic Mechanism)
In typical carcinoid syndrome:
- Tryptophan → (tryptophan hydroxylase) → 5-Hydroxytryptophan (5-HTP)
- 5-HTP → (aromatic L-amino acid decarboxylase) → Serotonin (5-HT)
- Serotonin stored in neurosecretory granules or released into circulation
- Platelets take up circulating 5-HT
- 5-HT → (MAO + aldehyde dehydrogenase) → 5-HIAA → excreted in urine
In atypical carcinoid syndrome: tumor lacks aromatic L-amino acid decarboxylase, so 5-HTP itself accumulates and is secreted (associated with foregut tumors, e.g., gastric carcinoids).
Up to 50% of dietary tryptophan is diverted into the serotonin synthesis pathway by tumor cells - depriving the body of tryptophan for niacin synthesis, which can cause pellagra.
Other bioactive products secreted: histamine, kallikrein, bradykinin, substance P, prostaglandins, dopamine, tachykinins
- Sleisenger and Fordtran's GI and Liver Disease
- Harrison's Principles of Internal Medicine 22E, p. 725
3. Morphology
Gross Pathology
- Intramural or submucosal masses forming small polypoid lesions
- Grossly yellow or tan in color
- Elicit an intense desmoplastic reaction - this fibrous stroma is so pronounced it can cause kinking and obstruction of the bowel
Histopathology
(A) Low power: Submucosal nodule of tumor cells embedded in dense fibrous tissue. The overlying mucosa may be intact.
(B) High power: Classic features:
- Uniform, monotonous cells - bland cytology
- Scant, pink granular cytoplasm (due to neurosecretory granules)
- Round-to-oval stippled ("salt-and-pepper") nucleus - fine and coarse chromatin clumps
- Arranged in islands, trabeculae, strands, glands, or sheets
- Low mitotic activity in well-differentiated (G1/G2) tumors
- No significant nuclear pleomorphism or necrosis (in low/intermediate grade)
Immunohistochemistry
| Marker | Significance |
|---|---|
| Chromogranin A | Most widely used; confirms neuroendocrine differentiation |
| Synaptophysin | Pan-neuroendocrine marker |
| Ki-67 | Defines grade (G1: <3%, G2: 3-20%, G3: >20%) |
| Serotonin | Positive in enterochromaffin-cell tumors |
- Robbins & Kumar Basic Pathology, p. 560
4. Clinical Features
Epidemiology
- Peak incidence: sixth decade (can occur at any age)
- Most are asymptomatic initially - often found incidentally on imaging or endoscopy
Symptoms Determined by Tumor Location and Hormone Production
Non-functional tumors (majority): present with:
- Abdominal pain (from desmoplastic kinking/obstruction)
- Intestinal bleeding
- Weight loss (large tumors)
Carcinoid Syndrome
Occurs in <10% of patients overall (approximately 8% of all GI-NETs) because:
- When tumors are confined to the intestine, vasoactive substances are metabolized by the liver (first-pass effect)
- Syndrome develops only when hepatic metastases (or retroperitoneal lesions) allow vasoactive amines to bypass the liver and enter systemic circulation
Clinical features of carcinoid syndrome (from table data):
| Feature | At Presentation | During Disease Course |
|---|---|---|
| Flushing | 70% | 78% |
| Diarrhea | 69% | 78% |
| Carcinoid heart disease | 26% | 30% |
| Wheezing/asthma | 11% | 12% |
| Pellagra | 2% | 1% |
Data from Sleisenger and Fordtran's GI and Liver Disease
Details of each feature:
Flushing:
- Sudden onset, deep red/violaceous erythema of the face and upper trunk/neck
- Initially lasts 2-5 minutes, later can persist for hours
- Precipitated by: stress, alcohol, exercise, cheese
- Mediated by: serotonin, histamine, tachykinins (substance P), bradykinin
Diarrhea:
- Watery; may be up to >10 episodes/day
- Caused by: serotonin-stimulated intestinal secretion + increased colonic motility + shortened intestinal transit time
Wheezing/bronchospasm: due to bronchoconstricting mediators
Carcinoid heart disease (Hedinger syndrome):
- Right-sided: tricuspid insufficiency + pulmonic stenosis
- Glistening white, plaque-like endocardial fibrotic thickenings
- Composed of smooth muscle cells in an acid mucopolysaccharide-rich matrix
- Left heart spared because the lungs inactivate serotonin before blood enters the left heart
- In affected patients, 70% of dietary tryptophan is converted to serotonin (vs. 1% normally)
Pellagra (rare): from niacin deficiency because tryptophan is diverted away from niacin synthesis
Location-Based Prognosis
| Location | Behavior |
|---|---|
| Foregut (stomach, duodenum, esophagus) | Rarely metastasize; curative resection possible. May produce gastrin (Zollinger-Ellison syndrome) or histamine (atypical flush). |
| Midgut (jejunum, ileum) | Often multiple; tend to be aggressive. Size, depth of invasion, mitoses predict outcome. Most likely to cause carcinoid syndrome when metastatic. |
| Hindgut - Appendix | Almost uniformly benign; discovered incidentally |
| Hindgut - Rectum | Usually small (<1 cm) and benign; those >2 cm metastasize in >70% |
Diagnosis
- Urinary 5-HIAA (24-hour collection): most reliable marker; elevated in carcinoid syndrome (false positives with serotonin-rich foods)
- Chromogranin A (serum): used to screen for NETs and monitor disease progression
- 68Ga-DOTATATE PET scan: highly sensitive imaging; exploits somatostatin receptor overexpression (>90% of NETs)
Key points to remember:
- Arise from enterochromaffin (APUD) cells; secrete serotonin, histamine, and kinins.
- Morphology: submucosal, yellow-tan, desmoplastic; histology shows bland "salt-and-pepper" nuclei in islands/trabeculae.
- Carcinoid syndrome requires hepatic metastases to bypass the liver's first-pass inactivation.
- Classic triad: flushing + diarrhea + right-sided heart disease.
- Diagnose biochemically with urinary 5-HIAA; the tryptophan diversion to serotonin can cause pellagra.
This is a shared conversation. Sign in to Orris to start your own chat.