Pathogenesis of hashimoto thyroiditis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Hashimoto thyroiditis" AND pathogenesis
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, well-sourced content. Let me compile the full answer.
Pathogenesis of Hashimoto Thyroiditis
Hashimoto thyroiditis (chronic autoimmune/lymphocytic thyroiditis) is the most common cause of hypothyroidism in iodine-sufficient regions. It was first described in 1912 by Hakaru Hashimoto as "struma lymphomatosa." It predominantly affects women (female:male ratio 10:1 to 20:1), peaking between 45-65 years.
Core Mechanism: Breakdown of Self-Tolerance
The central event is a breakdown in immune self-tolerance to thyroid autoantigens. The inciting events are not fully elucidated but likely involve:
- Abnormalities in regulatory T cells (Tregs) that normally suppress autoreactive clones
- Exposure of normally sequestered thyroid antigens to the immune system
This triggers progressive autoimmune destruction of thyrocytes. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis Diagram
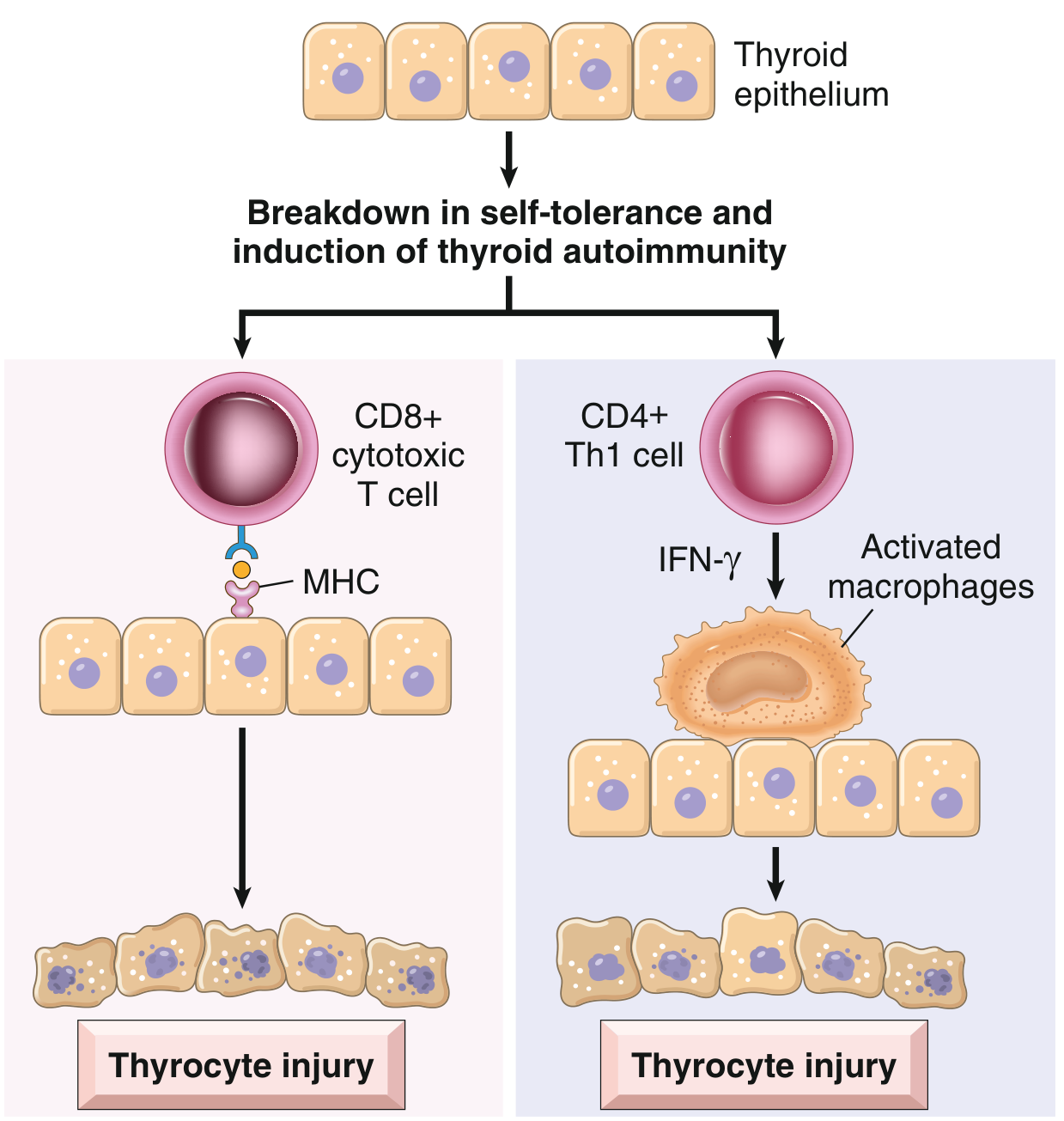
Fig. 18.4 - Pathogenesis of Hashimoto thyroiditis. Breakdown of immune tolerance to thyroid autoantigens results in progressive autoimmune destruction of thyrocytes by infiltrating cytotoxic T cells, locally released cytokines, and other mechanisms. (Robbins & Kumar Basic Pathology)
Four Major Immunologic Mechanisms of Thyrocyte Destruction
1. CD8+ Cytotoxic T Cell-Mediated Killing
- Activated CD4+ T (helper) cells recognize thyroid antigens and recruit CD8+ cytotoxic T cells to the gland
- These cytotoxic T cells directly kill thyroid follicular epithelial cells via MHC-I-restricted antigen recognition
- This is considered the primary effector mechanism
2. Cytokine-Mediated Cell Death (Th1 Pathway)
- Activated CD4+ Th1 cells secrete IFN-γ in the thyroid microenvironment
- IFN-γ recruits and activates macrophages
- Activated macrophages cause bystander damage to thyroid follicles
- This inflammatory milieu sustains progressive follicular destruction
3. Antibody-Mediated Mechanisms
Three main antibody targets:
- Anti-thyroid peroxidase (anti-TPO) antibodies - present in ~95% of patients
- Anti-thyroglobulin (anti-Tg) antibodies - present in ~60% of patients
- Anti-TSH receptor (anti-TSH-R) antibodies - present in ~60% (blocking type, contributing to hypothyroidism)
- Less commonly: anti-sodium/iodine symporter antibodies (~25%)
These antibodies may damage follicular cells via:
- Antibody-dependent cell-mediated cytotoxicity (ADCC) - NK cells kill antibody-coated thyrocytes
- Complement-dependent cytotoxicity - complement fixation leads to membrane attack
- TSH receptor blockade - blocking antibodies impair TSH signaling, reducing thyroid function
Note: It remains debated whether these antibodies are the primary cause or merely a consequence of thyroid injury. - Robbins & Kumar Basic Pathology, Schwartz's Principles of Surgery
4. Apoptosis (Programmed Cell Death)
- Fas-FasL interactions have been implicated as an additional mechanism of thyrocyte destruction
- Apoptosis of thyroid epithelial cells contributes to the progressive loss of functional parenchyma - Schwartz's Principles of Surgery, 11th Edition
Genetic Susceptibility
Hashimoto thyroiditis has a strong genetic component:
- ~40% concordance in monozygotic twins
- ~50% of asymptomatic siblings of affected patients have circulating antithyroid antibodies
Key susceptibility gene polymorphisms include:
| Gene | Function |
|---|---|
| CTLA4 (cytotoxic T lymphocyte-associated antigen-4) | Encodes a T-cell response inhibitor; loss-of-function favors autoimmunity |
| PTPN22 (protein tyrosine phosphatase non-receptor type 22) | Regulates T-cell activation thresholds |
| IL2RA (interleukin-2 receptor α chain, CD25) | Regulates Treg function and T-cell proliferation |
All three are regulators of T-cell responses, confirming that dysregulated T-cell immunity is the central defect. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Environmental Triggers and Associations
- Excess iodine intake - associated with increased incidence of chronic thyroiditis
- Medications: interferon-α, lithium, amiodarone can precipitate or worsen thyroiditis
- Postpartum state - postpartum thyroiditis shares mechanistic parallels (TPOAb positive, preceded by thyrotoxic phase)
- Familial clustering and co-occurrence with Graves' disease and other autoimmune diseases (type 1 diabetes, pernicious anemia, Addison's disease)
Morphological Consequences of the Pathogenesis
The immune-mediated destruction produces characteristic histological changes:
- Diffuse lymphocytic infiltration - lymphocytes, plasma cells, macrophages with germinal center formation
- Hurthle (Oxyphil/Oncocytic) cell metaplasia - follicular epithelial cells develop abundant eosinophilic cytoplasm packed with mitochondria; a metaplastic response to chronic injury
- Follicular atrophy - destruction of normal follicular architecture
- Interstitial fibrosis - connective tissue replacement of destroyed parenchyma (especially in the fibrosing variant)
Unlike Riedel thyroiditis, the fibrosis in Hashimoto thyroiditis does not extend beyond the thyroid capsule. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Summary Flow
Genetic predisposition (CTLA4/PTPN22/IL2RA polymorphisms)
+
Environmental trigger (iodine, drugs, viral?)
↓
Breakdown of Treg-mediated self-tolerance
↓
Autoreactive CD4+ T helper cell activation against thyroid antigens
↙ ↘
CD8+ CTL recruitment Th1 cytokines (IFN-γ)
(direct killing) → macrophage activation
+
Autoantibodies (anti-TPO, anti-Tg, anti-TSHR)
→ ADCC, complement, TSH-R blockade
+
Apoptosis (Fas-FasL)
↓
Progressive thyrocyte destruction → Hurthle cell metaplasia + fibrosis
↓
Hypothyroidism (in ~20-85% depending on population)
Sources:
- Robbins & Kumar Basic Pathology (p. 731) - Primary reference
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Detailed molecular mechanisms
- Schwartz's Principles of Surgery, 11th Edition - Apoptosis and antibody targets
- Current Surgical Therapy, 14th Edition - Clinical correlations
Various types of thyroiditis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from all major sources. Let me compile the full, well-organized answer.
Types of Thyroiditis
Thyroiditis refers to a diverse group of disorders characterized by some form of thyroid inflammation. They are best classified by onset/duration and etiology:
Classification Overview
| Type | Duration | Etiology | Thyroid Pain | Functional Outcome |
|---|---|---|---|---|
| Acute (suppurative) | Days-weeks | Bacterial/fungal infection | Severe | Usually euthyroid |
| Subacute granulomatous (de Quervain) | Weeks-months | Viral | Yes, severe | Transient hyper → hypo → recovery |
| Subacute lymphocytic (silent/painless) | Weeks-months | Autoimmune | No | Transient hyper → hypo → recovery |
| Postpartum thyroiditis | Weeks-months | Autoimmune | No | Transient hyper → hypo → often recovery |
| Hashimoto (chronic autoimmune) | Chronic, permanent | Autoimmune | No | Progressive hypothyroidism |
| Riedel's thyroiditis | Chronic | IgG4-related disease | No | Variable; may cause hypothyroidism |
| Drug-induced | Variable | Drugs (amiodarone, interferon, ICIs) | Sometimes | Variable |
| Radiation thyroiditis | Days-weeks after RAI | Radiation injury | Yes | Transient, then usually hypothyroid |
- Harrison's Principles of Internal Medicine, 22nd Edition; Current Surgical Therapy, 14th Edition
1. Acute (Suppurative) Thyroiditis
Etiology: Bacterial infection - most commonly Staphylococcus, Streptococcus, Enterobacter. Fungal (Aspergillus, Candida, Histoplasma, Pneumocystis) and mycobacterial infections can occur, especially in immunocompromised patients.
Predisposing factors:
- Children/young adults: piriform sinus fistula (remnant of 4th branchial pouch, predominantly left-sided)
- Elderly: pre-existing goiter, degenerating thyroid malignancy
Clinical features:
- Acute onset with fever, severe thyroid pain referred to the throat or ears
- Tender, asymmetric goiter; erythema over the gland
- Dysphagia, lymphadenopathy, systemic illness
- ESR and WBC elevated; thyroid function usually normal
Investigations: FNA showing polymorphonuclear leukocytes; Gram stain and culture guide therapy
Complications: Abscess formation, tracheal obstruction, septicemia, retropharyngeal abscess, mediastinitis, jugular venous thrombosis
Treatment: Antibiotics; surgical drainage of abscess if required
2. Subacute Granulomatous Thyroiditis (de Quervain / Viral / Giant Cell Thyroiditis)
Etiology: Triggered by viral infection. Viruses implicated: mumps, coxsackievirus, influenza, adenoviruses, echoviruses, SARS-CoV-2. Also reported after COVID-19 vaccination.
Peak incidence: 30-50 years; women affected 3-4x more than men
Pathogenesis: Virus-induced host tissue damage stimulates a cytotoxic T-lymphocyte response against thyroid antigens. Unlike autoimmune thyroiditis, the immune response is virus-initiated and not self-perpetuating, hence self-limited. Strong association with HLA-B35 haplotype.
Histology:
- Early: disrupted follicles, neutrophilic microabscesses
- Later: lymphocytes, activated histiocytes/macrophages, multinucleated giant cells engulfing colloid (characteristic)
- Resolution: fibrosis, then restoration of normal architecture
Clinical Course - Three Phases:
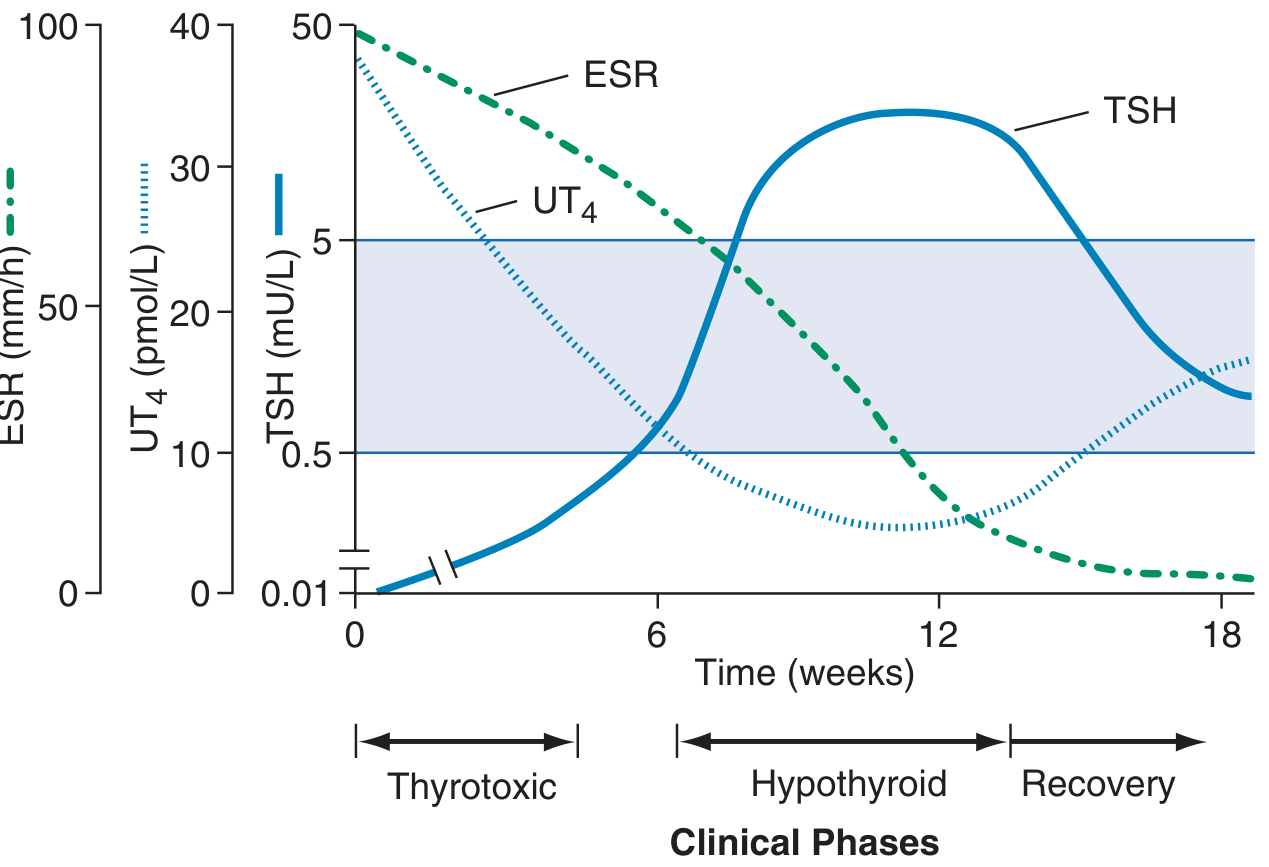
FIGURE 396-3 - Clinical course of subacute thyroiditis. ESR is initially very high; UT4 elevated then falls; TSH suppressed then rises. (Harrison's Principles of Internal Medicine, 22nd Ed.)
| Phase | Duration | T4/T3 | TSH | RAIU | ESR |
|---|---|---|---|---|---|
| Thyrotoxic | ~0-6 wks | ↑ | ↓ | Very low (<5%) | Very high |
| Hypothyroid | ~6-12 wks | ↓ | ↑ | Returns toward normal | Falling |
| Recovery | ~12-18+ wks | Normal | Normal | Normal | Normal |
Key features:
- Exquisitely tender goiter; pain referred to jaw or ear
- Malaise, fever, sore throat; preceded by URTI
- T4:T3 ratio lower than in Graves' disease
- Antithyroid antibodies usually negative
- ESR typically >50 mm/h (often >100)
Treatment:
- NSAIDs/aspirin for pain relief
- Corticosteroids for severe cases
- Beta-blockers for symptomatic thyrotoxicosis
- Thyroid hormone replacement if symptomatic hypothyroidism
- Self-limited in >90%; ~15% develop permanent hypothyroidism
3. Hashimoto Thyroiditis (Chronic Autoimmune / Chronic Lymphocytic Thyroiditis)
Etiology: Autoimmune - breakdown of self-tolerance to thyroid antigens (thyroglobulin, thyroid peroxidase, TSH-R)
Epidemiology: Most common cause of hypothyroidism in iodine-sufficient regions. Prevalence peaks 45-65 years; F:M = 10-20:1. Most common inflammatory thyroid disorder worldwide.
Pathogenesis (summary):
- Genetic predisposition: CTLA4, PTPN22, IL2RA polymorphisms
- Treg dysfunction → autoreactive CD4+ and CD8+ T-cell activation
- CD8+ cytotoxic T cells directly kill thyrocytes
- CD4+ Th1 cells → IFN-γ → macrophage activation and follicular damage
- Autoantibodies (anti-TPO ~95%, anti-Tg ~60%) → ADCC and complement-dependent killing
- Apoptosis (Fas-FasL pathway) contributes additionally
Histology:
- Diffuse lymphoplasmacytic infiltration with germinal center formation
- Hürthle (oxyphil/oncocytic) cell metaplasia of follicular epithelium
- Follicular atrophy
- Variable interstitial fibrosis (does not extend beyond the capsule)
Clinical features:
- Painless diffuse goiter (firm, rubbery)
- Hypothyroidism (slow onset, in ~20-85%)
- "Hashitoxicosis" - transient thyrotoxic phase in some patients
- Goiter may cause compressive symptoms
- Associated with other autoimmune conditions (T1DM, pernicious anemia, Addison's)
- Elevated anti-TPO antibodies (hallmark laboratory finding)
Variants:
- Goitrogenic form (classic - enlarged gland)
- Atrophic form (no goiter, directly hypothyroid)
- Fibrosing variant (extensive fibrosis; can mimic Riedel's thyroiditis)
Complications:
- Permanent hypothyroidism
- Increased risk of thyroid lymphoma (extranodal marginal zone B-cell lymphoma)
- Possible association with papillary thyroid carcinoma (controversial)
4. Silent (Painless) Thyroiditis / Chronic Lymphocytic Thyroiditis
Etiology: Presumed autoimmune - most patients have anti-TPO antibodies or family history of autoimmune disease
Special form - Postpartum thyroiditis: Occurs in ~5% of postpartum females; peaks at ~6 weeks after delivery coinciding with immune rebound after pregnancy-induced immune tolerance
Histology:
- Lymphocytic infiltration with germinal centers
- Patchy follicular disruption and collapse
- No fibrosis, no Hürthle cell metaplasia (distinguishes it from Hashimoto thyroiditis)
- Thyroid grossly normal or mildly enlarged
Clinical features:
- Painless goiter (key distinguishing feature)
- Mild transient hyperthyroidism → hypothyroidism → recovery (similar pattern to de Quervain but without pain)
- RAIU low during thyrotoxic phase (low uptake differentiates from Graves')
- ~30% may evolve into permanent hypothyroidism
5. Riedel's Thyroiditis (Invasive Fibrous Thyroiditis)
Etiology: Now recognized as a manifestation of IgG4-related disease - associated with fibrosis and tissue infiltration by IgG4-positive plasma cells
Characteristics:
- Rare, chronic condition
- Extensive fibrosis involving the thyroid AND contiguous neck structures (muscles, nerves, vessels, trachea, esophagus)
- Fibrosis extends beyond the thyroid capsule (key distinction from Hashimoto's fibrosing variant)
- Hard, fixed thyroid mass clinically simulates thyroid carcinoma
- May be associated with fibrosis at other sites: retroperitoneum (retroperitoneal fibrosis), mediastinum, orbit, bile ducts
Clinical features:
- Progressive compressive symptoms: dyspnea, dysphagia, hoarseness (recurrent laryngeal nerve involvement)
- Hypothyroidism if sufficient thyroid parenchyma is destroyed
- Hypoparathyroidism if parathyroids are encased
Treatment: Corticosteroids (first line for IgG4-RD); tamoxifen; surgical decompression of trachea if needed
6. Drug-Induced Thyroiditis
Several drugs can cause thyroiditis through different mechanisms:
| Drug | Mechanism | Type of Thyroiditis |
|---|---|---|
| Amiodarone | Excess iodine + direct cytotoxic effect | Type 1 (iodine-induced) or Type 2 (destructive/thyroiditis) |
| Interferon-α | Immune activation | Autoimmune (can trigger Hashimoto or Graves') |
| Lithium | Inhibits thyroid hormone release | Hypothyroidism/thyroiditis |
| Tyrosine kinase inhibitors (sunitinib, sorafenib) | Multiple mechanisms | Hypothyroidism |
| Immune checkpoint inhibitors (anti-PD1, anti-CTLA4) | Immune dysregulation | Autoimmune thyroiditis; hyper then hypo pattern |
7. Radiation Thyroiditis
- Occurs days to weeks after radioactive iodine (¹³¹I) treatment or external beam radiation to the neck
- Characterized by acute inflammation and tenderness of the thyroid
- Usually transient; thyroid function eventually declines toward hypothyroidism
- FNA not typically needed (diagnosis is clinical in context of recent radiation)
Comparative Summary: Key Distinguishing Features
| Feature | Acute (Suppurative) | Subacute (de Quervain) | Hashimoto | Silent/Postpartum | Riedel |
|---|---|---|---|---|---|
| Pain | Severe | Severe, referred | None | None | None |
| Fever | Yes | Yes (low-grade) | No | No | No |
| Etiology | Infection | Viral | Autoimmune | Autoimmune | IgG4-RD |
| Anti-TPO | Negative | Negative | Positive (95%) | Often positive | Variable |
| RAIU | Normal | Very low | Low/normal | Low | Variable |
| ESR | High | Very high | Normal/mildly ↑ | Normal | Variable |
| WBC | High | Normal or mild ↑ | Normal | Normal | Normal |
| Histology | PMN infiltrate | Granulomas, giant cells | Lymphocytes, germinal centers, Hürthle cells | Lymphocytes, no Hürthle cells | Dense fibrosis |
| Outcome | Resolution | Self-limited; 15% permanent hypo | Permanent hypothyroidism | 30% permanent hypo | Progressive; compressive |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition - Primary reference for clinical classification
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Histopathology and pathogenesis
- Robbins & Kumar Basic Pathology - Key concepts
- Current Surgical Therapy, 14th Edition - Clinical variants and surgical management
This is a shared conversation. Sign in to Orris to start your own chat.