Ischemic ulcer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
I now have comprehensive content from multiple textbooks. Let me compile the full answer.
Ischemic (Arterial Insufficiency) Ulcer
Definition
An ischemic ulcer is a tissue breakdown resulting from inadequate arterial perfusion to the skin and underlying structures. It represents one of the most serious presentations of peripheral artery disease (PAD) and is a hallmark of chronic limb-threatening ischemia (CLTI) - formerly called critical limb ischemia.
Epidemiology & Risk Factors
About 5% of lower extremity ulcerations are caused by arterial insufficiency. High-risk patients include:
- Long-standing hypertension
- Active smokers
- Diabetics
- Hyperlipidemia
- Those with atherosclerotic coronary artery disease
The presence of an arterial ulceration identifies patients at increased risk for limb loss.
- Andrews' Diseases of the Skin, p. 11
- Rosen's Emergency Medicine, p. 1182
Pathophysiology
Ischemic ulcers result from the reduction in arterial blood flow, most commonly due to atherosclerosis obliterans causing progressive luminal narrowing. Reduced perfusion leads to tissue hypoxia, cell death, and failure of normal wound healing mechanisms. The ulcers typically appear at sites of highest pressure and furthest from the arterial supply - the distal digits and toes.
Clinical Features
Location
- Distal to the ankle - most commonly the toes and terminal digits
- Around nail beds or between toes (friction from one toe on another)
- Less common: metatarsal heads, heel, malleoli, lateral surface of the ankle
Ulcer Characteristics
- Painful - the most severe pain of all lower extremity ulcers
- Small, shallow, dry base
- Base is gray, yellow, or black - minimal to no granulation tissue
- Sharp, indolent rim - no signs of epithelialization or cellular proliferation
- Minimal or no discharge/drainage
- Initial red, painful plaque that breaks down into a superficial ulcer with a surrounding zone of purpuric erythema
- A membranous, inactive eschar may form over the ulcer
Associated Limb Signs
- Skin thinning and atrophy
- Absence of hair on the dorsum of the foot
- Nail deformities
- Absent or decreased pedal pulses
- Pallor on elevation
- Dependent rubor (foot becomes red when lowered)
- Cold extremity
- Collapsed veins
- Pale and cyanotic appearance
Pain Pattern
- Pain worsens at night and at rest
- Relieved by placing the foot in a dependent position (patients hang leg off bed or sleep in a chair)
- Claudication on exercise at reproducible distances
Comparison: Ischemic vs. Neuropathic Ulcer
| Feature | Ischemic Ulcer | Neuropathic Ulcer |
|---|---|---|
| Pain | Painful | Painless |
| Pulses | Absent | Normal |
| Margins | Irregular | Regular, punched-out |
| Location | Toes, glabrous margins | Plantar surface of foot |
| Calluses | Absent/infrequent | Present |
| Sensation | Variable | Loss of sensation |
| Blood flow | Decreased | Increased (AV shunting) |
| Veins | Collapsed | Dilated |
| Foot temperature | Cold | Warm, dry |
| Appearance | Pale, cyanotic | Red, hyperemic |
| Bony deformities | None | Present |
- Schwartz's Principles of Surgery, 11th ed., p. 986
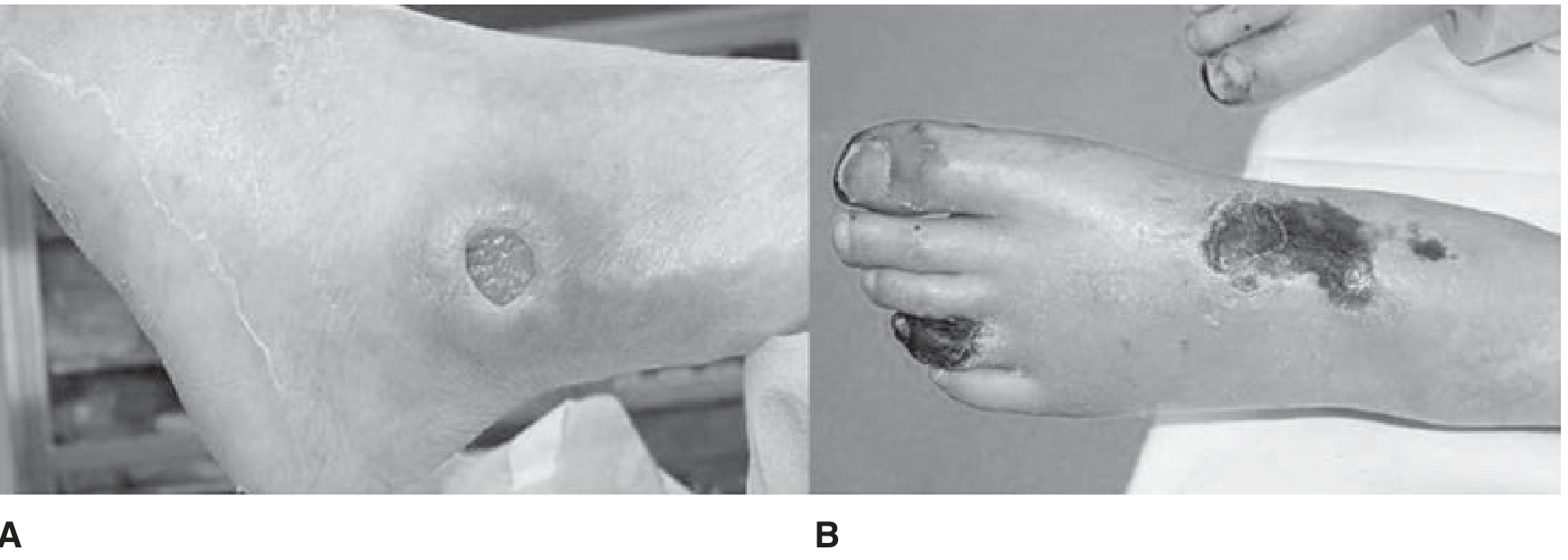
Figure: A - Neuropathic ulcer with punched-out appearance. B - Ischemic ulcer showing gangrenous skin change on the foot and toes.
Differential Diagnosis of Lower Extremity Ulcers
| Type | ~Prevalence | Key Feature |
|---|---|---|
| Venous stasis ulcer | ~90% | Near medial malleolus, moist, improves with elevation |
| Arterial/ischemic ulcer | ~5% | Distal digits, dry, worsens with elevation |
| Neuropathic ulcer | Most of remainder | Painless, plantar surface, rim of callus |
| Hypertensive (Martorell) ulcer | Rare | Lateral malleolus, most painful |
| Vasculitis / cholesterol emboli | Rare | Multiple ulcers, sudden onset |
Additional clues:
- Multiple ulcers above and below the ankle - suggest vasculitis or atheromatous embolization
- Eosinophilia + palpable pulses + sudden onset + renal insufficiency - cholesterol emboli
Diagnosis
Clinical Examination
- Careful palpation of leg pulses (femoral, popliteal, dorsalis pedis, posterior tibial)
- Assess skin changes, temperature, capillary refill
Ankle-Brachial Index (ABI)
- The ratio of ankle systolic pressure to brachial systolic pressure
- Normal: approximately 1.0
- ABI < 0.9 - PAD present
- ABI < 0.75 - arterial insufficiency
- ABI < 0.5 - substantial insufficiency (limb-threatening)
- ABI < 0.4 - typically associated with rest pain and tissue loss
Imaging
- CT Angiography - identifies location and extent of occlusive disease for surgical/endovascular planning
- Duplex ultrasound for non-invasive assessment
Management
1. Risk Factor Modification
- Smoking cessation (essential)
- Blood pressure control
- Lipid management (statins)
- Glycemic control in diabetics
- Antiplatelet therapy (aspirin or clopidogrel)
2. Wound Care
- Protect from injury and cold
- Avoid tight socks and constrictive footwear
- Prevent infection using measures similar to venous ulcer care
- Keep wound clean; avoid compression bandaging (contraindicated in significant arterial disease)
3. Revascularization (Definitive Treatment)
- Limb-threatening ischemia is a surgical emergency
- Options:
- Open surgical bypass (for complex, long-segment, or heavily calcified lesions - TASC type D)
- Endovascular intervention - preferred for shorter, less calcified lesions (TASC type A); includes angioplasty, stenting
- Hybrid approaches combining open and endovascular techniques
- If blood supply cannot be improved, conservative measures are the only option
4. Adjunctive Therapies
- Hyperbaric oxygen - may improve short-term healing; evidence is limited (Cochrane review shows benefit short-term, not long-term); limited by availability and cost
- Prostanoids (e.g., iloprost) - used in non-reconstructable disease
- Amputation - as a last resort when limb is not salvageable
5. Cardiac Evaluation
All patients with peripheral arterial disease require full cardiac evaluation before any vascular procedure, given the high incidence of concomitant coronary artery disease (~25% have correctable CAD).
Special Considerations
- Thromboangiitis obliterans (Buerger disease) - should be considered in progressive arterial insufficiency, especially in young smokers
- Anal fissure is classified as a localized ischemic ulcer of the anal canal (treated by relaxing the internal anal sphincter)
- Martorell hypertensive-ischemic ulcer - a specific subtype in poorly controlled hypertension; characteristically starts as a painful reddish-blue infarcted skin area near the lateral malleolus, forming a hemorrhagic bleb that breaks down into a superficial ulcer (up to 5-10 cm); the most painful of all lower extremity ulcers
- Injury to a foot with borderline ischemia can convert a stable situation into one that is limb-threatening
Sources: Andrews' Diseases of the Skin (Clinical Dermatology) | Rosen's Emergency Medicine | Schwartz's Principles of Surgery, 11th ed. | Fuster and Hurst's The Heart, 15th ed.
This is a shared conversation. Sign in to Orris to start your own chat.