Apex pulse deficit
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Good data retrieved. Here is the full answer:
Apex-Pulse Deficit
Definition
The apex-pulse deficit (or simply "pulse deficit") is the numerical difference between the apical heart rate (counted by auscultating the cardiac apex with a stethoscope) and the peripheral pulse rate (counted simultaneously at the radial artery by palpation).
Formula: Apex-pulse deficit = Apical rate - Radial rate
Mechanism
When the heart contracts prematurely or when ventricular filling time is insufficient, the stroke volume generated by that contraction is too low to propagate a palpable pressure wave to the periphery. The apex beat (or apical auscultatory sound) still occurs, but the corresponding radial pulse is absent - creating a "deficit." As Guyton & Hall explains:
"When the heart contracts ahead of schedule, the ventricles will not have filled with blood normally, and the stroke volume output during that contraction is depressed or is almost absent. Therefore, the pulse wave passing to the peripheral arteries after a premature contraction may be so weak that it cannot be felt in the radial artery. Thus, a deficit in the number of radial pulses occurs when compared with the actual number of contractions of the heart."
- Guyton and Hall Textbook of Medical Physiology
Causes
| Condition | Reason for deficit |
|---|---|
| Atrial fibrillation (AF) | Most common cause - chaotic, irregularly irregular rhythm with variable ventricular filling; many beats have inadequate stroke volume |
| Atrial flutter with variable block | Similar mechanism to AF |
| Premature atrial contractions (PACs) | Early beat = short filling time = weak or absent peripheral wave |
| Premature ventricular contractions (PVCs) | Same as above; compensatory pause follows |
| Pulseless electrical activity (PEA) / electro-mechanical dissociation | Extreme end of the spectrum - all beats lack a peripheral pulse |
Clinical Significance
- An irregular pulse on palpation should prompt auscultation of the apical rate. Roberts & Hedges notes: "An irregular pulse suggests atrial fibrillation or flutter with variable block, and accurate assessment of the pulse should be carried out by auscultation of the apical cardiac sounds."
- The larger the deficit, the more severe the arrhythmia/hemodynamic compromise. A greater pulse deficit in AF generally reflects more severe disease (Roberts & Hedges' Clinical Procedures in Emergency Medicine).
- In AF, the deficit helps guide the urgency of rate control therapy.
How to Measure
- Two examiners ideally work simultaneously - one auscultates the apex, the other palpates the radial pulse.
- Both count for exactly 60 seconds (or 30 seconds x 2).
- Subtract radial rate from apical rate.
- Even a single examiner can estimate it using a watch, but simultaneous counting is more accurate.
Normal Value
Zero - in a healthy person with every cardiac contraction generating an adequate peripheral pulse wave, there is no deficit.
Example Scenario
A patient in atrial fibrillation has an apical rate of 130 bpm and a radial rate of 90 bpm:
- Apex-pulse deficit = 130 - 90 = 40 beats/min
- This indicates 40 ventricular contractions per minute are mechanically ineffective at the periphery.
Relation to Monitoring
In anesthesia and critical care, pulse deficit can arise when the ECG-derived heart rate (electrical) diverges from the plethysmograph/arterial-line pulse rate (mechanical) - Miller's Anesthesia describes this as the monitoring equivalent of pulse deficit, with PEA being the most extreme form.
Sources:
- Guyton and Hall Textbook of Medical Physiology
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Miller's Anesthesia, 10th ed.
Atrial flutter ecg features
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Comprehensive data gathered. Here is the full answer:
Atrial Flutter - ECG Features
12-Lead ECG of Typical Atrial Flutter (Fuster & Hurst's The Heart, 15th ed.)
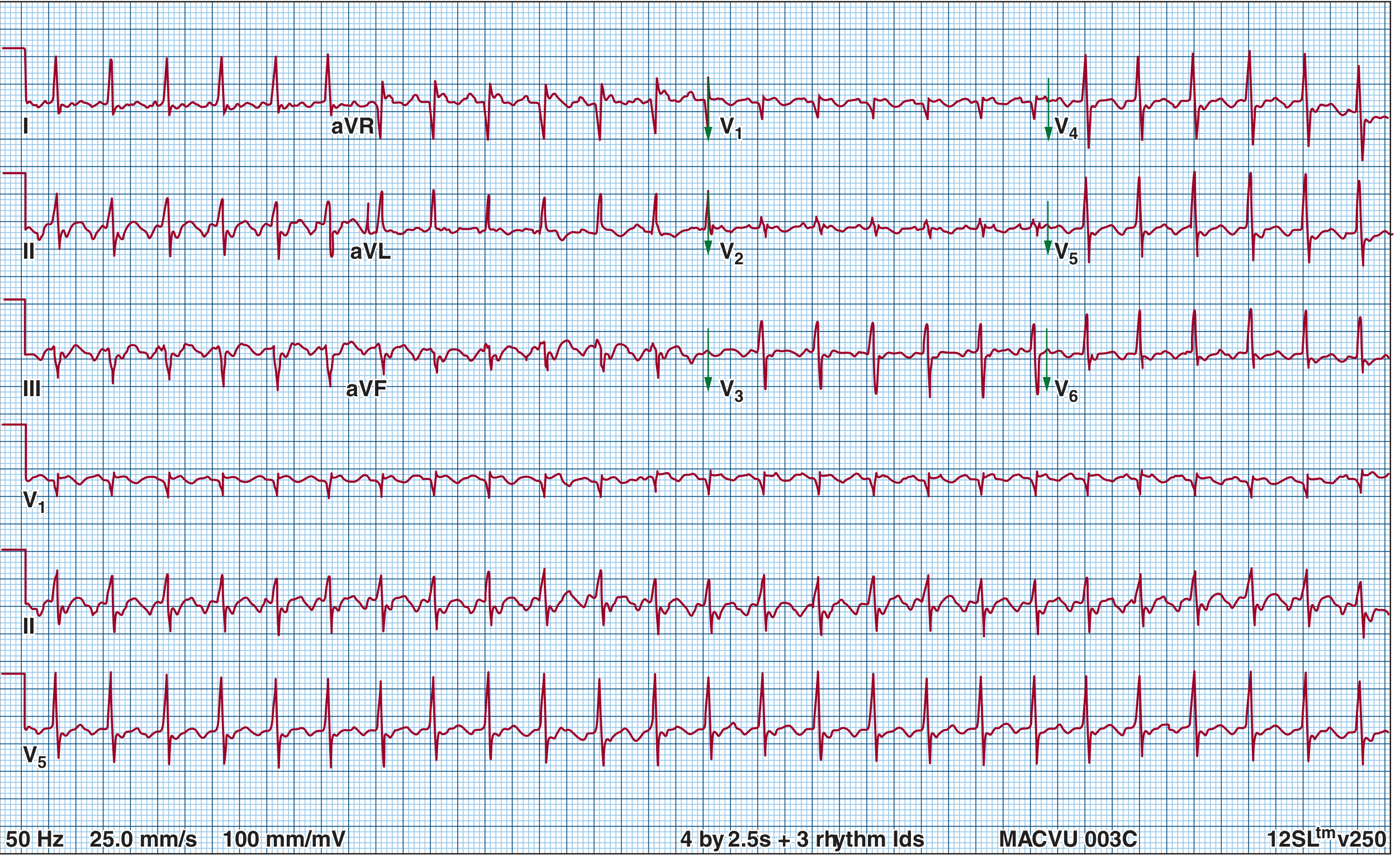
Typical atrial flutter with 2:1 AV block. Note the classic negative sawtooth flutter waves in leads II, III, and aVF, and upright discrete P-like waves in V1.
Core ECG Features
| Feature | Detail |
|---|---|
| Atrial rate | 250-350 bpm; classically ~300 bpm |
| Flutter (F) waves | Continuous sawtooth-like pattern - no isoelectric baseline between waves |
| AV conduction ratio | Typically 2:1 (ventricular rate ~150 bpm); can be 3:1, 4:1, or variable |
| Ventricular rate | Depends on block - most commonly 150 bpm with 2:1 |
| QRS morphology | Usually narrow and normal (unless aberrant conduction or BBB) |
| Rhythm | Ventricular rhythm is regular (with fixed block) or regularly irregular (with variable block) |
Lead-by-Lead Flutter Wave Morphology
Typical (Counterclockwise / Type I) Flutter:
- Leads II, III, aVF: Negative ("inverted") sawtooth flutter waves - the hallmark. The waves show a slow downslope followed by a sharp upstroke.
- Lead V1: Discrete, upright, positive P-like waves (no sawtooth) - because V1 is perpendicular to the frontal plane circuit. This can be mistaken for a different rhythm on telemetry monitoring.
- Lead aVR: Positive flutter waves
- Lead I / aVL: Flutter waves may be small or biphasic
"The negative sawtooth pattern in ECG leads II, III, and aVF represents activation superiorly up the interatrial septum, followed by inferiorly directed activation down the right atrial free wall anterior to the crista terminalis, and then across the tricuspid annulus."
- Fuster and Hurst's The Heart, 15th ed.
Reverse Typical (Clockwise / Type II) Flutter:
- Leads II, III, aVF: Positive flutter waves
- Lead V1: Negative flutter waves
- Same macro-reentrant circuit around the tricuspid annulus, but in the opposite (clockwise) direction
Lead II Rhythm Strip - Classic Sawtooth (Guyton & Hall)
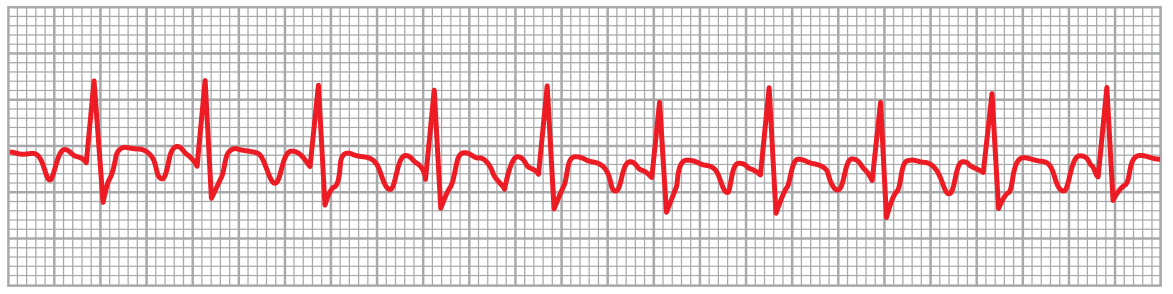
Atrial flutter at 250 bpm with 2:1 AV block. Every second flutter wave is "buried" within or just after the QRS/T complex.
Mechanism Behind the ECG Pattern
The circuit is a large single macro-reentrant loop around the tricuspid valve annulus in the right atrium, dependent on the cavotricuspid isthmus (CTI) as the critical slow-conduction zone:
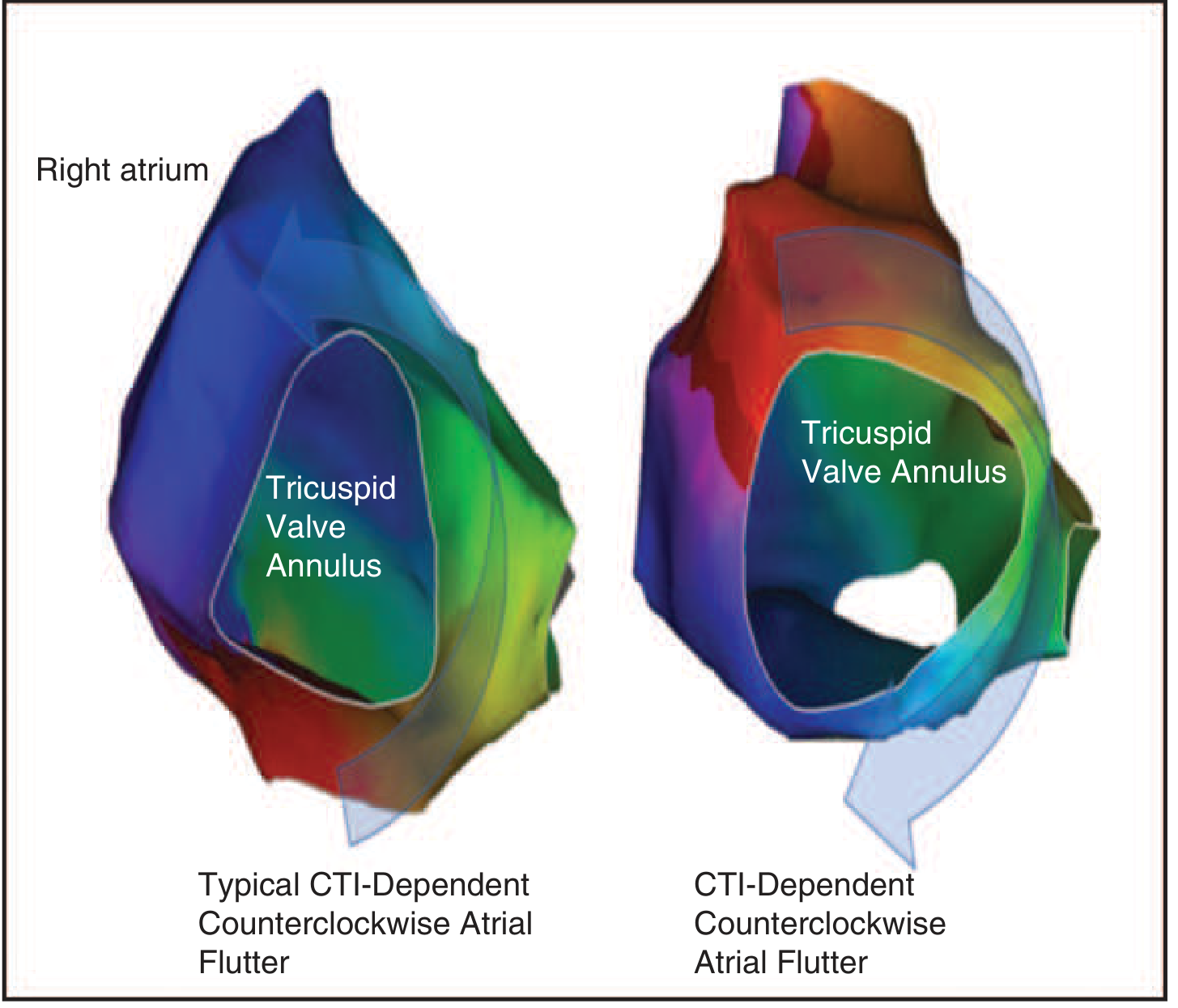
Electroanatomical maps showing the counterclockwise reentrant circuit around the tricuspid valve annulus - the substrate of typical flutter.
Because only one synchronized wavefront travels around the atrium (unlike AF where multiple chaotic wavelets exist), flutter waves are regular and uniform rather than irregular and chaotic.
Key Distinguishing Points vs. Atrial Fibrillation
| Atrial Flutter | Atrial Fibrillation | |
|---|---|---|
| Atrial waves | Regular sawtooth F waves | Chaotic, irregular f waves |
| Atrial rate | 250-350 bpm | >350 bpm (often 400-600) |
| Ventricular rhythm | Regular (fixed block) or regularly irregular | Irregularly irregular |
| Isoelectric baseline | Absent (waves flow continuously) | May be present between fine f waves |
| AV block | Fixed ratio (2:1, 3:1, 4:1) | No fixed ratio |
Clinical Tip: Unmasking Flutter Waves
When 2:1 flutter produces a ventricular rate of exactly ~150 bpm, the alternate flutter waves are hidden within the QRS or T waves. To unmask them:
- Carotid sinus massage or IV adenosine transiently increases AV block, slowing the ventricular rate and revealing the flutter waves clearly.
"Flutter waves on the ECG may be difficult to see. Atrial flutter waves can be unmasked by vagal maneuvers such as carotid sinus massage or the use of adenosine to block the AV node transiently."
- Fuster and Hurst's The Heart, 15th ed.
Sources:
- Fuster and Hurst's The Heart, 15th ed.
- Guyton and Hall Textbook of Medical Physiology
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- Rosen's Emergency Medicine, 9th ed.
HAS BLED score
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
All data in hand. Here is the complete answer:
HAS-BLED Score
Purpose
HAS-BLED estimates the 1-year risk of major bleeding in patients with atrial fibrillation who are being considered for or are on anticoagulation therapy. It is used alongside CHA₂DS₂-VASc to weigh bleeding risk against stroke risk - the goal being not to withhold anticoagulation, but to identify and correct modifiable bleeding risk factors.
Scoring Table
| Letter | Clinical Characteristic | Points |
|---|---|---|
| H | Hypertension (uncontrolled systolic BP >160 mmHg) | 1 |
| A | Abnormal renal function (dialysis, transplant, creatinine >200 µmol/L) | 1 |
| Abnormal liver function (cirrhosis, bilirubin >2× normal, or AST/ALT/ALP >3× normal) | 1 | |
| S | Stroke (prior history) | 1 |
| B | Bleeding (prior major bleeding or predisposition - anaemia, coagulopathy) | 1 |
| L | Labile INR (unstable/high INR; time in therapeutic range <60%) | 1 |
| E | Elderly (age >65 years) | 1 |
| D | Drugs predisposing to bleeding (antiplatelets, NSAIDs) | 1 |
| Alcohol (≥8 drinks/week) | 1 | |
| Maximum score | 9 |
Note: "A" (renal OR liver) and "D" (drugs OR alcohol) can each score 1 or 2 if both sub-criteria are present, giving the maximum of 9.
Score Interpretation
| HAS-BLED Score | Risk Category | Approximate Major Bleeds/100 patient-years |
|---|---|---|
| 0 | Low | ~1.0 |
| 1 | Low | ~1.0 |
| 2 | Moderate | ~1.9 |
| ≥3 | High | ≥3.7 - rising steeply |
Score ≥3 = "High risk" - warrants caution and efforts to correct modifiable risk factors.
- Rosen's Emergency Medicine; Bradley and Daroff's Neurology in Clinical Practice
Annual Bleeding Rate vs. Stroke Risk at Equivalent Scores
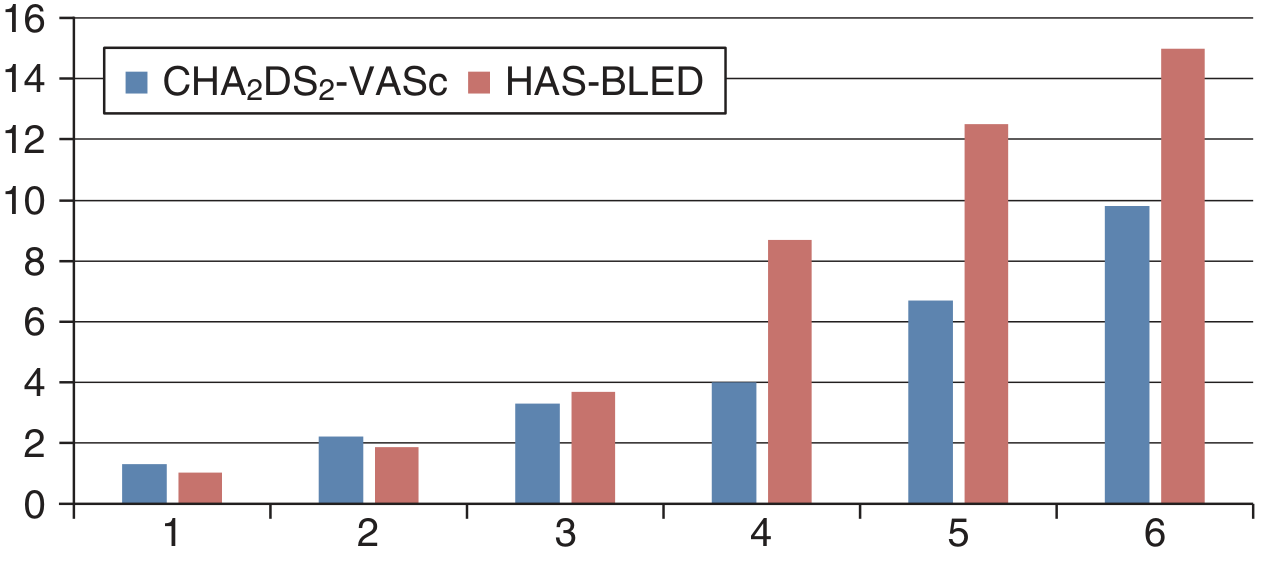
Annual event rates (%) for stroke (CHA₂DS₂-VASc) and major bleeding (HAS-BLED) as a function of score. Note that at scores 4-6 the bleeding risk rises faster and higher than stroke risk at the same numeral score - Harrison's, 22nd ed.
Mnemonic: H-A-S-B-L-E-D
Hypertension uncontrolled Abnormal renal/liver function (1 pt each) Stroke history Bleeding history or predisposition Labile INR Elderly (>65) Drugs (antiplatelets/NSAIDs) or alcohol (1 pt each)
Clinical Use - Key Points
-
High HAS-BLED does NOT mean withhold anticoagulation. In most patients with AF, stroke risk (CHA₂DS₂-VASc ≥2) outweighs bleeding risk. The score flags which modifiable factors to address.
-
Modifiable factors to correct: uncontrolled hypertension, labile INR (switch to DOAC), drugs causing bleeding (stop NSAIDs/antiplatelets if possible), excess alcohol.
-
Non-modifiable factors (age, prior stroke, prior bleed) still warrant anticoagulation in most cases but heighten monitoring.
-
DOACs vs. warfarin: Labile INR (L criterion) is eliminated when using DOACs (dabigatran, rivaroxaban, apixaban, edoxaban), which reduces the HAS-BLED score by 1 point and is one reason DOACs are preferred.
-
The score was originally validated in the Euro Heart Survey population and has been externally validated in multiple cohorts. It performs similarly to other bleeding scores (ORBIT, ATRIA) with modest predictive accuracy (c-statistic ~0.60-0.72).
Sources:
- Rosen's Emergency Medicine, 9th ed. (Box 65.11)
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- Bradley and Daroff's Neurology in Clinical Practice (Table 65.3)
- Sabiston Textbook of Surgery, 21st ed.
Supraventricular tachycardia as emergency physician theory from Harrison, balthzar, tintinaali , rosen emergency book and latest updates
Finding Sources
Finding Sources
Searching PubMed
"supraventricular tachycardia"[MeSH Terms] AND "emergency"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"supraventricular tachycardia" AND "guideline"
Reading File
Reading File
Searching the Web
2019 ESC SVT guidelines supraventricular tachycardia management summary 2024 2025 update
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading Web Page
https://www.acc.org/latest-in-cardiology/ten-points-to-remem…
This covers the full emergency physician's theory of SVT drawn from all four requested sources plus the latest guideline updates. Key takeaways worth memorizing:
- AVNRT is ~60-80% of all PSVT - the most common SVT you'll see in the ED
- Vagal maneuvers first - the modified Valsalva (supine + leg raise after straining) converts ~43%
- Adenosine 6→12→12 mg IV rapid push works in 85-90% of cases
- WPW + AF = do NOT block the AV node - procainamide or immediate cardioversion only
- Treat all wide-complex tachycardia as VT until proven otherwise
- The 2019 ESC guidelines removed amiodarone, digoxin, sotalol, and lidocaine from SVT management - these are no longer appropriate acute agents for SVT
VT vs SVT brugada criteria
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
All data collected. Comprehensive answer below:
VT vs SVT with Aberrancy - Brugada Criteria & Beyond
The Core Rule
Any wide-complex tachycardia must be treated as VT until proven otherwise.
This is because:
- VT is the most common cause of wide-complex tachycardia (~80%)
- Misdiagnosing VT as SVT and giving AV-nodal blockers (verapamil, diltiazem) can cause hemodynamic collapse
- Treating SVT as VT (with amiodarone or cardioversion) is almost never fatal
Brugada Algorithm (1991) - The Classic 4-Step Stepwise Approach
Algorithm Flowchart (Rosen's Emergency Medicine):
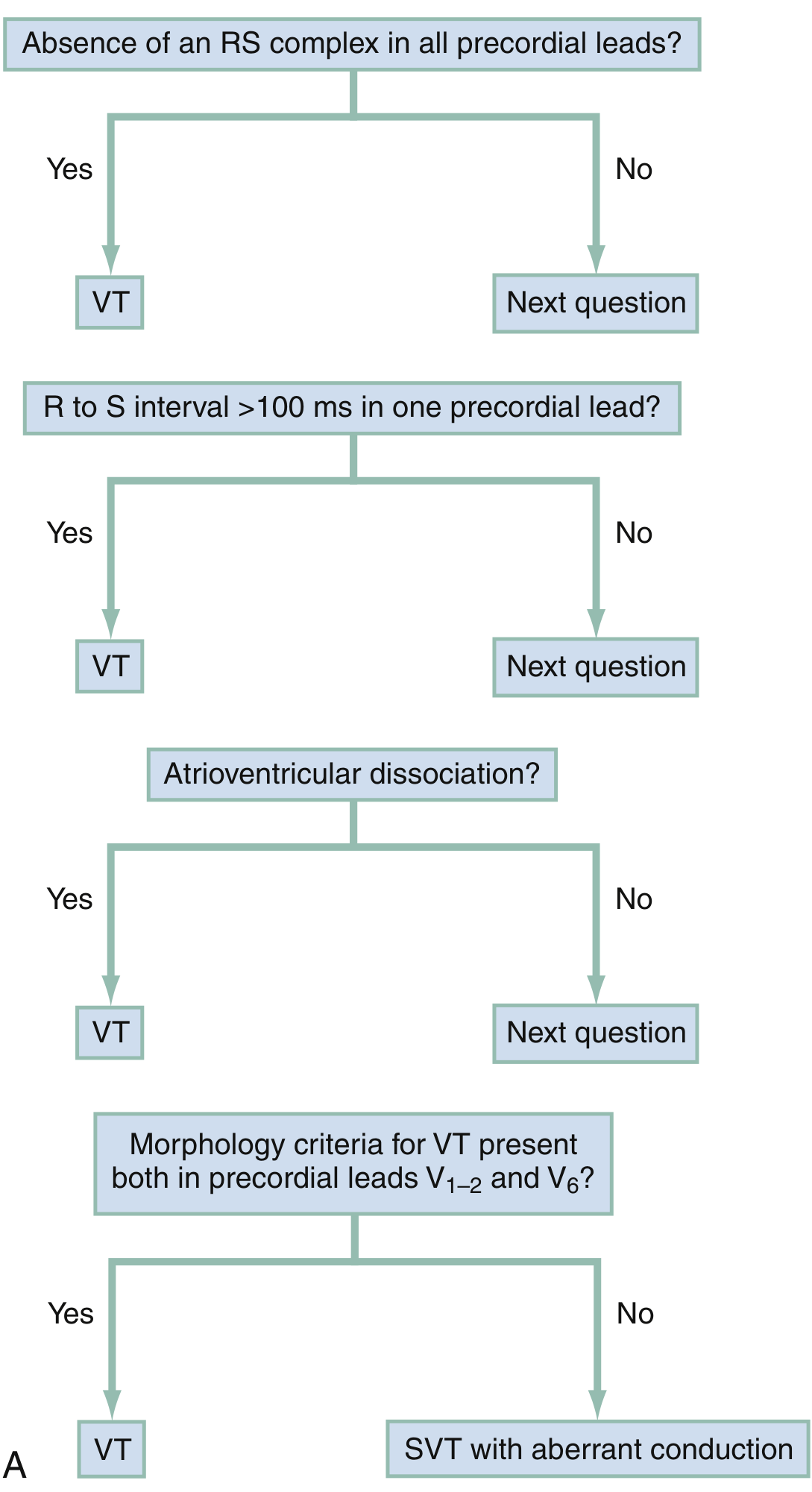
Brugada four-step algorithm - Rosen's Emergency Medicine. Any single YES answer = VT. Only if ALL FOUR are NO = SVT with aberrancy.
The Four Criteria in Detail
| Step | Question | Finding | Diagnosis |
|---|---|---|---|
| 1 | Absence of RS complex in all precordial leads (V1-V6)? | Only R, only QS, only QR, only monophasic patterns - no RS anywhere | VT |
| 2 | R-to-S nadir interval >100 ms in any one precordial lead? | Slow, slurred descent from R peak to S nadir >100 ms | VT |
| 3 | AV dissociation present? | P waves marching independently of QRS; capture beats; fusion beats | VT |
| 4 | Morphology criteria for VT in V1-2 AND V6? | See lead-specific patterns below | VT |
| All 4 = NO | - | None of the above found | SVT with aberrancy |
"Only when the response to all four questions is negative is a supraventricular rhythm with abnormal conduction diagnosed. As soon as a single 'yes' answer is noted, VT is diagnosed."
- Rosen's Emergency Medicine, 9th ed.
Sensitivity: ~99% | Specificity: ~97% (original Brugada paper, 1991)
Step 4 - Lead Morphology Criteria Explained
The most complex step. Patterns depend on whether the wide complex has RBBB-like or LBBB-like morphology:
RBBB-like (positive in V1 - tall right precordial leads):
| Lead | Favors VT | Favors SVT (classic RBBB) |
|---|---|---|
| V1 | Monophasic R wave, QR pattern, or RS (where R>S) | Typical rSR' (rabbit ear pattern, R'>r) |
| V6 | S wave, rS, or QR pattern | Typical qRS (small q, tall R, small s) |
Remember: In RBBB + VT, V1 looks "wrong" - you get a fat rabbit ear (R>R') or monophasic R, not the clean rSR' of true RBBB.
LBBB-like (negative in V1 - left precordial leads dominant):
| Lead | Favors VT | Favors SVT (classic LBBB) |
|---|---|---|
| V1 or V2 | R wave >30 ms wide; notching on S wave downstroke; R to S nadir >70 ms | Clean rS or QS, rapid S nadir <70 ms |
| V6 | QR or QS pattern (Q wave present) | Monophasic R with NO Q wave |
Quick rule for LBBB-like WCT: Any Q wave in V6 = VT. Any initial R>30 ms in V1/V2 = VT.
Griffith Algorithm (1994) - The Alternative Approach
The Griffith approach is "reversed" - it assumes VT first and looks for classic BBB patterns to diagnose SVT:
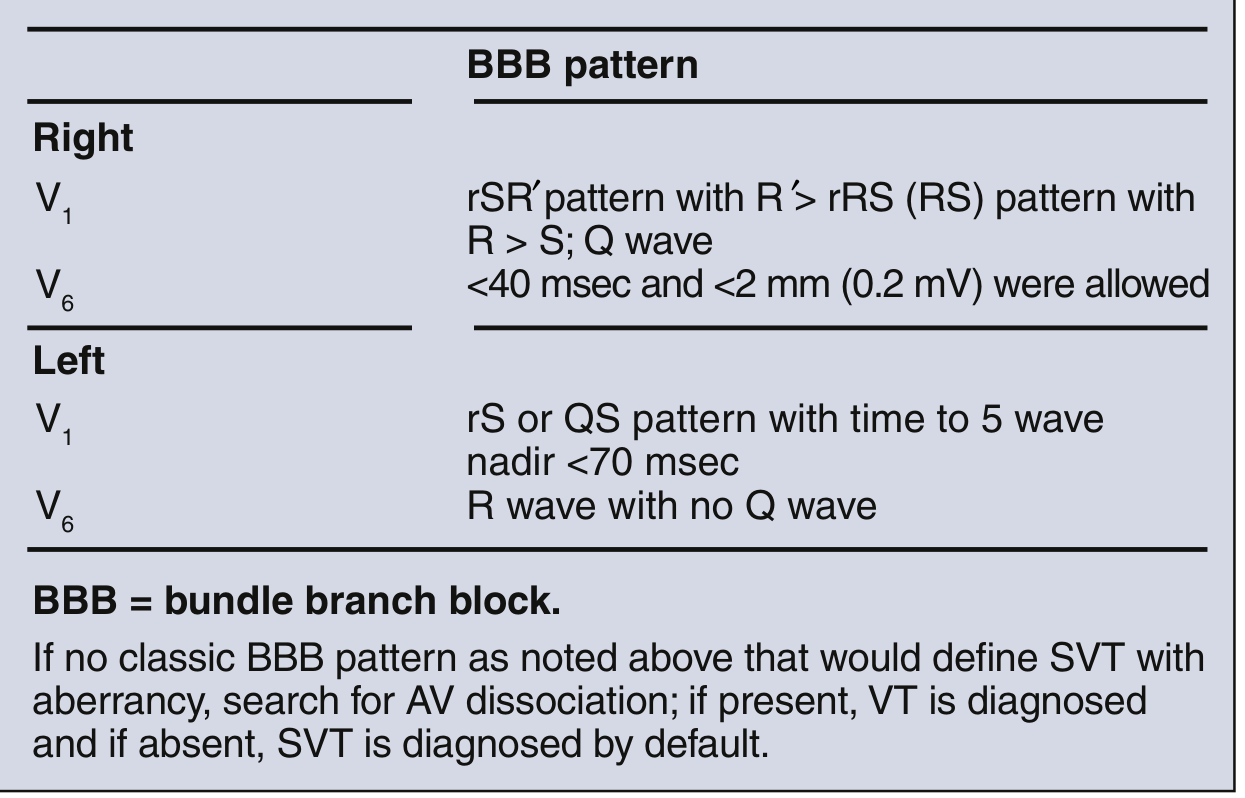
Griffith criteria: SVT is diagnosed only if the QRS looks exactly like classic RBBB or LBBB. Anything else = VT.
Harrison's Algorithm - AV Dissociation + aVR Focus
Harrison's 22nd ed. highlights two high-yield bedside markers:
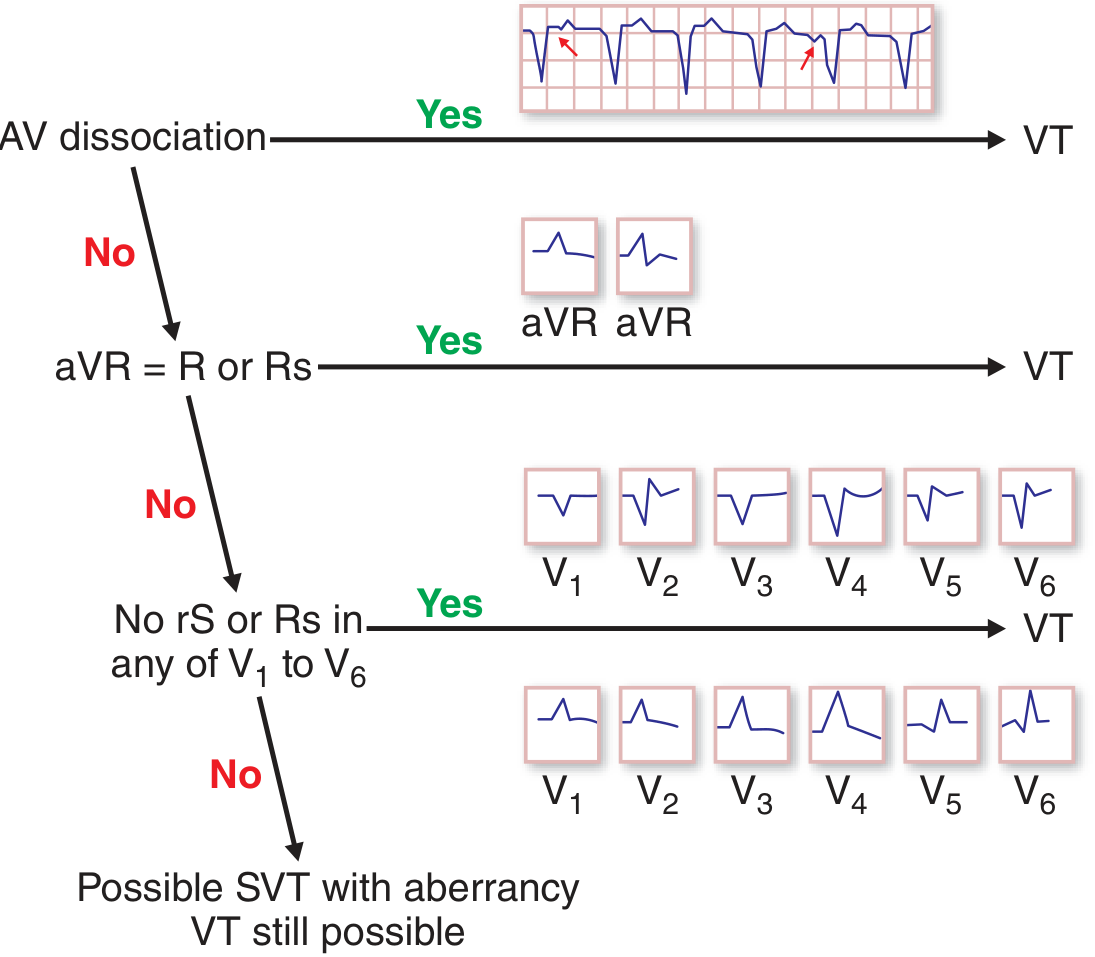
Harrison's simplified algorithm using AV dissociation, aVR morphology, and concordance.
"A monophasic R wave or Rs complex in aVR, or concordance from V1 to V6 of monophasic R or S waves, is also relatively specific for VT."
- Harrison's, 22nd ed.
Vereckei Algorithm (2008) - Lead aVR Only
A simpler, single-lead approach using only aVR. VT if ANY one of:
| Step | Criterion | Rationale |
|---|---|---|
| 1 | Initial R wave in aVR | Depolarization moving away from normal vector |
| 2 | Initial r or q wave >40 ms in aVR | Slow initial conduction = ventricular origin |
| 3 | Notch on initial descending limb of predominantly negative QRS | Slurred slow conduction |
| 4 | vi/vt ratio <1 (voltage traveled in first 40 ms / last 40 ms) | Slow onset, fast terminal = VT pattern |
If none = SVT with aberrancy.
Pava Criterion (2010) - Simplest Single Rule
R-wave peak time in lead II >50 ms = VT
Measure from the onset of QRS to the first peak of R wave in lead II. Fast to remember and apply.
All 5 Algorithms Compared (Tintinalli Table 18-22)
| Algorithm | Leads Used | Approach | Notes |
|---|---|---|---|
| Brugada 1991 | All precordial leads | Stepwise; any 1 of 4 = VT | Classic; highest sensitivity |
| Griffith 1994 | V1, V2, V6 | Reversed; look for SVT pattern | Assumes VT, seeks to disprove |
| Lau 2000 | Multiple | Bayesian likelihood ratios | Complex; rarely used bedside |
| Vereckei 2008 | aVR only | Stepwise 4 criteria | Simple; good in fast ED setting |
| Pava 2010 | Lead II only | Single criterion: R peak >50 ms | Simplest of all |
"Neither has proven consistently superior. Simplicity favors the Vereckei or Pava approaches."
- Tintinalli's Emergency Medicine, 9th ed.
Classic Clinical Features Favoring VT vs SVT (Rosen's Table 65.5)
| Parameter | Favors VT | Favors SVT with aberrancy |
|---|---|---|
| Age | ≥50 years | ≤35 years |
| History | Prior MI, CHF, CABG, ASHD | Prior SVT episodes |
| Cannon A waves | Present (AV dissociation) | Absent |
| Pulse variability | Variable (AV dissociation) | Constant |
| First heart sound | Variable intensity | Constant |
| QRS duration | >140 ms (RBBB) or >160 ms (LBBB) | <140 ms |
| Frontal axis | Extreme left axis ("northwest": -90° to ±180°) | Normal or right axis |
| Concordance V1-V6 | All positive or all negative | Absent |
| Fusion beats | Present (pathognomonic for VT) | Absent |
| Capture beats | Present (narrow QRS amid wide) | Absent |
| AV dissociation | Present | Absent |
| Response to vagal maneuvers | No effect | May slow or terminate |
Pitfalls and Limitations
- AV dissociation is pathognomonic for VT but present in only ~20-30% of VT cases - its absence does NOT exclude VT
- 1:1 retrograde VA conduction can occur in VT - a P wave after every QRS does not mean SVT
- Sodium channel toxicity (tricyclic poisoning, flecainide overdose) and hyperkalemia can produce wide bizarre QRS mimicking VT - look for clinical context
- Antidromic WPW produces very wide QRS that satisfies Brugada VT criteria yet is not VT - adenosine/cardioversion are appropriate; avoid AV-nodal blockers
- Bundle branch reentry VT can look identical to native LBBB in sinus rhythm
- Brugada pattern (sodium channelopathy) is NOT the same as Brugada VT/SVT algorithm
- All algorithms have lower accuracy in patients with severe structural heart disease
ED Management of Undifferentiated WCT
Wide-complex tachycardia (QRS >120 ms, rate >100 bpm)
|
↓
Hemodynamically UNSTABLE?
→ Immediate synchronized DC cardioversion (200 J biphasic)
|
↓ (stable)
Apply Brugada algorithm (or Vereckei/Pava if faster)
|
→ VT diagnosed or uncertain: treat as VT
→ Adenosine trial reasonable if regular, stable, possibly SVT
|
VT treatment:
- Amiodarone 150 mg IV over 10 min (preferred if structural heart disease)
- Procainamide 15-17 mg/kg IV over 30-60 min (if no structural disease)
- Lidocaine 1-1.5 mg/kg IV (third line)
- Synchronized cardioversion if refractory
Amiodarone is the preferred drug for stable VT with structural heart disease (Harrison's, 22nd ed.).
Sources:
- Rosen's Emergency Medicine, 9th ed. (Table 65.5, Fig. 65.32)
- Tintinalli's Emergency Medicine, 9th ed. (Table 18-22)
- Harrison's Principles of Internal Medicine, 22nd ed. (Fig. 261-1)
- Braunwald's Heart Disease, 12th ed.
- Original: Brugada P et al. Circulation 1991;83:1649-1659
- Vereckei A et al. Heart Rhythm 2008;5:89-98
- Pava LF et al. J Am Coll Cardiol 2010;55:2017-2023
VT vs SVT brugada criteria with ECG explanation
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
All images and data collected. Full ECG-illustrated guide below:
VT vs SVT - Brugada Criteria with ECG Explanation
The Overriding Rule
All wide-complex tachycardias (QRS >120 ms, rate >100 bpm) are VT until proven otherwise.
Hemodynamic stability does NOT rule out VT - patients can be in VT with preserved BP for hours.
What Is a Wide-Complex Tachycardia (WCT)?
A WCT arises when a tachycardia produces a QRS >120 ms. Three main causes:
- VT - impulse originates in ventricle, spreads slowly cell-to-cell without the fast conduction system
- SVT with aberrancy - supraventricular impulse with pre-existing or rate-related bundle branch block
- Pre-excited tachycardia (WPW antidromic / pre-excited AF) - accessory pathway bypass
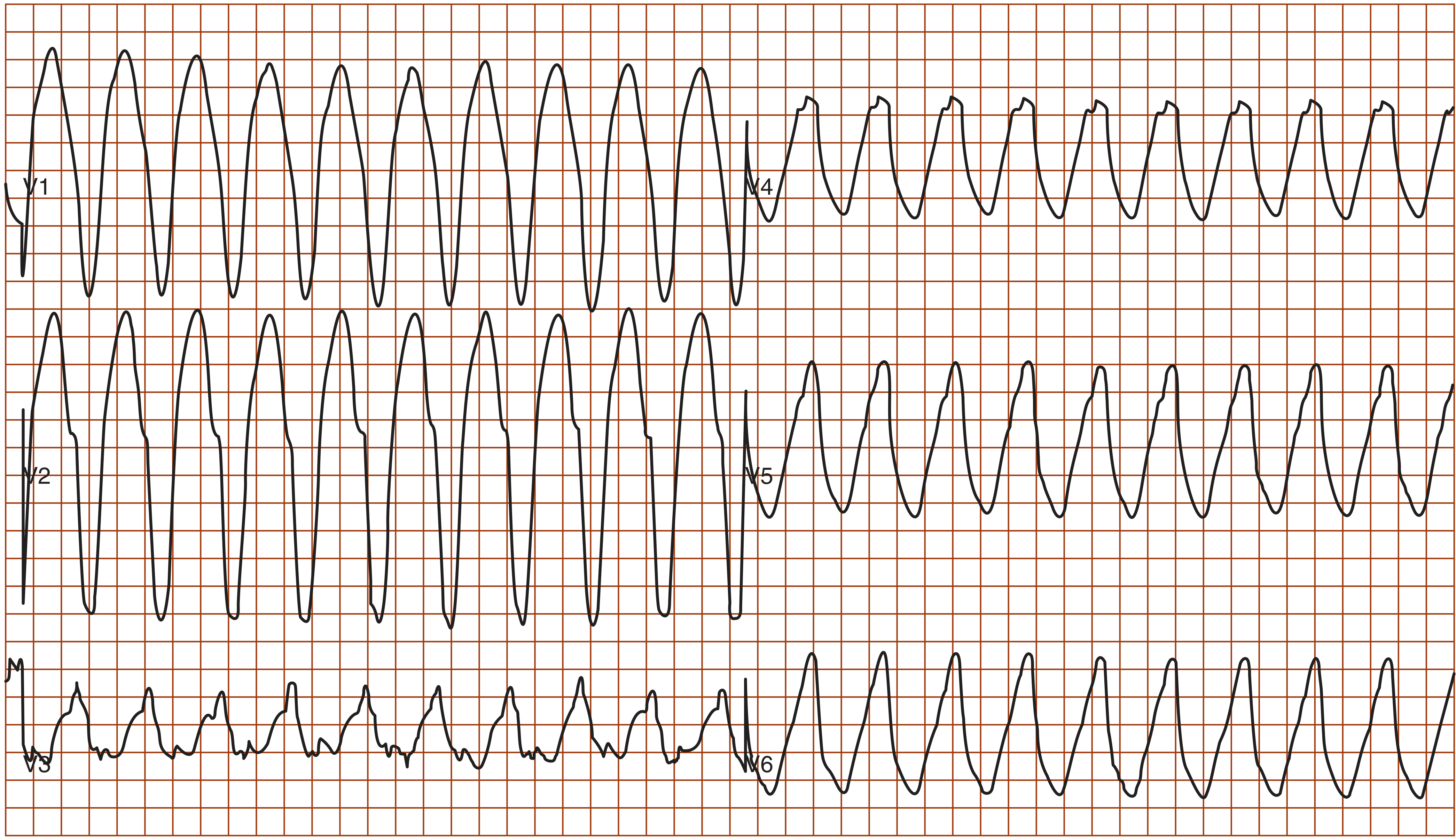
ECG of Ventricular Tachycardia (Monomorphic):
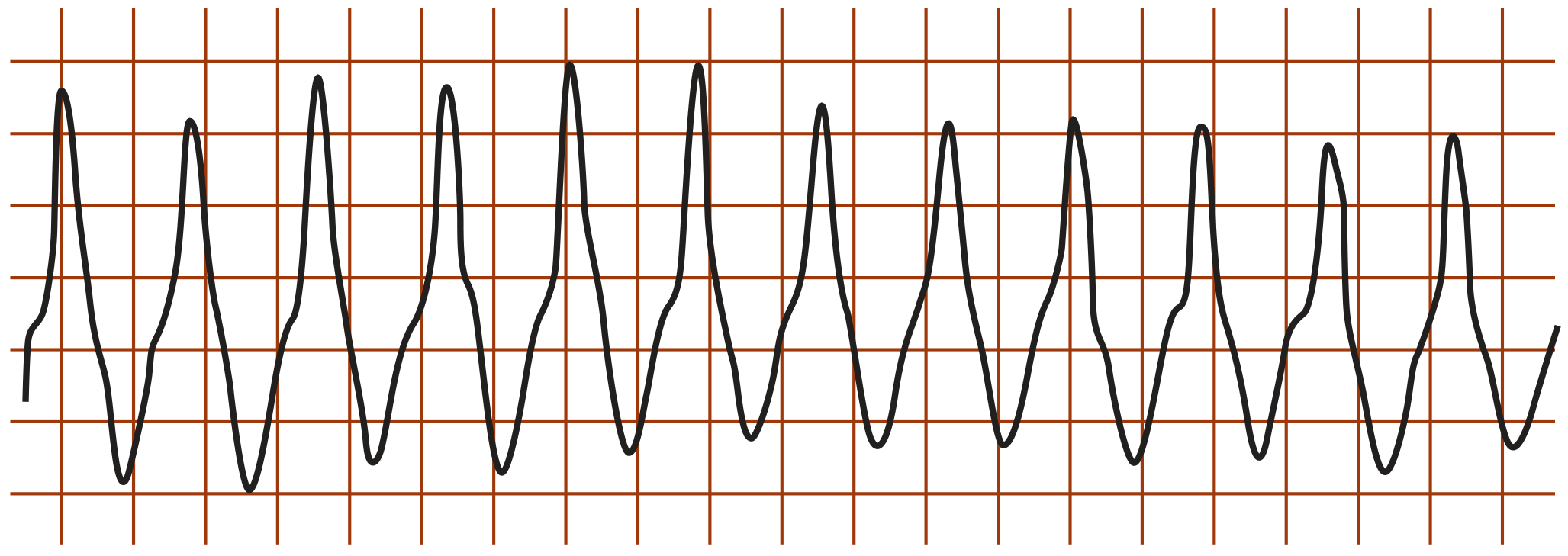
Monomorphic VT: wide, regular, bizarre-looking QRS complexes at ~150-200 bpm. No discernible P waves. - Symptom to Diagnosis, 4th ed.
Brugada 4-Step Algorithm (1991) - The Stepwise Flowchart
Apply questions in sequence. Stop as soon as one answer is YES - that is VT. Only if ALL FOUR are NO = SVT with aberrancy.
Flowchart (Washington Manual / Rosen's):
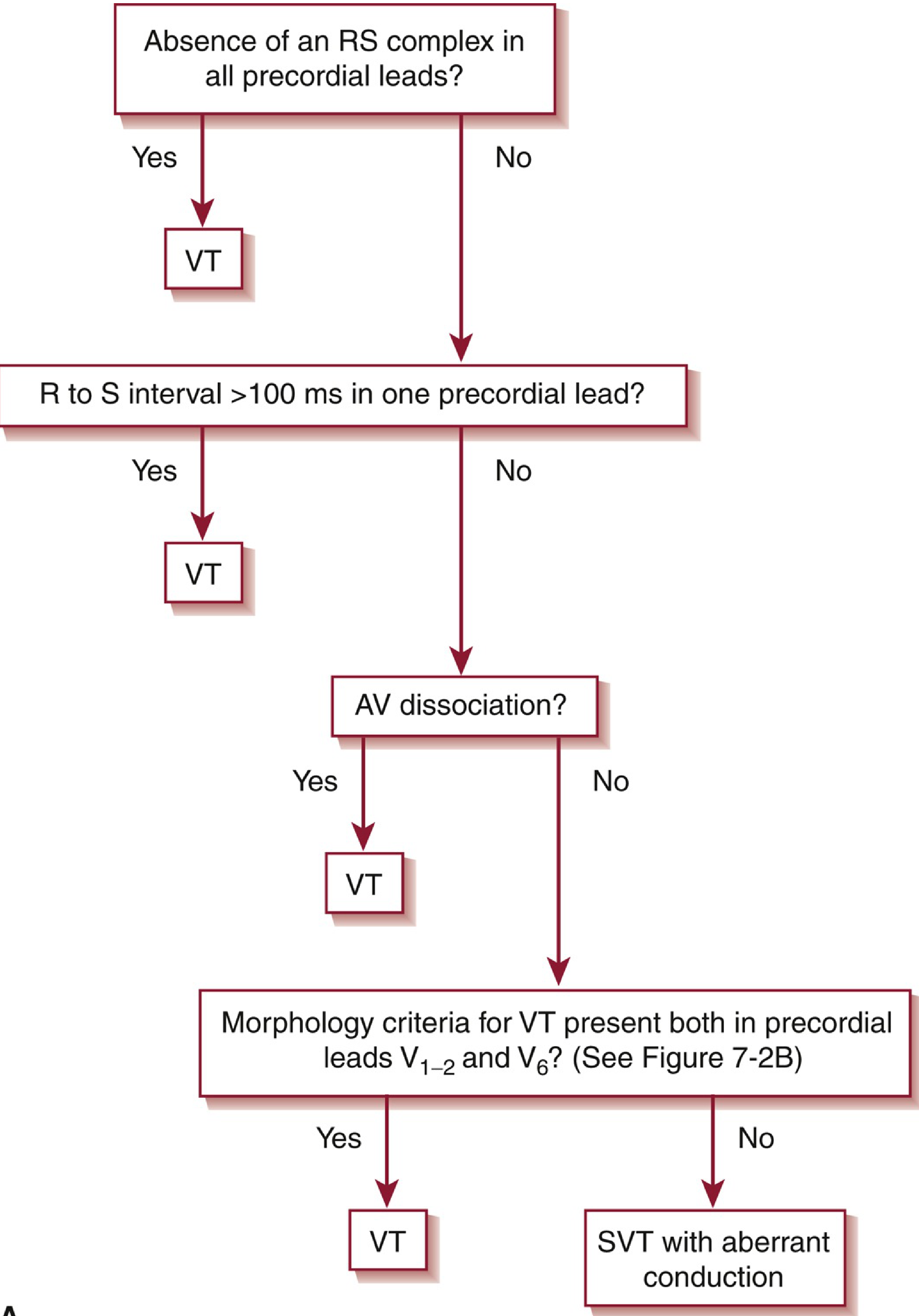
The Brugada algorithm. Any single YES = VT diagnosed immediately. Proceed to next step ONLY on NO. - Washington Manual / Rosen's
Criterion 1 - Absence of RS Complex in ALL Precordial Leads
What to look for: Scan all 6 chest leads (V1 through V6). If not a single lead has an RS pattern - meaning every lead has only a monophasic R, only a QS, only a QR, or only a monophasic QS - this is VT.
Why this occurs: In VT, the wavefront originates from an ectopic ventricular focus and spreads in an abnormal direction. The depolarization is so discordant with normal ventricular activation that it cannot produce the typical RS transition seen in normal conduction.
ECG clue: Look across ALL precordial leads - if you see any RS anywhere, move to question 2.
| Finding | Interpretation |
|---|---|
| All leads show R only, or QS only, or QR only (no biphasic RS anywhere) | YES = VT |
| At least one lead shows an RS pattern | NO - proceed to Q2 |
Criterion 2 - R-to-S Nadir Interval >100 ms in Any Precordial Lead
What to measure: In any lead that has an RS pattern, measure from the peak of R to the lowest point (nadir) of S. If this interval exceeds 100 ms (2.5 small squares) in even ONE lead = VT.
Normal comparison: In true BBB (SVT with aberrancy), the S nadir is reached quickly because the conduction system is partially intact. The rapid descent from R peak to S nadir is a marker of fast conduction tissue involvement.
Why in VT: The ventricular ectopic impulse spreads slowly through working myocardium rather than fast conduction fibers, so the whole QRS - including the descent from R to S - is sluggish and prolonged.
Normal RS (SVT): R peak → S nadir occurs in ≤100 ms (fast, conducted)
VT RS pattern: R peak → S nadir takes >100 ms (slow, cell-to-cell)
| Finding | Interpretation |
|---|---|
| Any precordial RS: time from R peak to S nadir >100 ms | YES = VT |
| All RS durations ≤100 ms | NO - proceed to Q3 |
Criterion 3 - AV Dissociation
What it means: P waves and QRS complexes march completely independently of each other. The atria are still being driven by the SA node at a normal rate (~60-100 bpm), while the ventricles are firing rapidly from an ectopic focus. They are completely uncoupled.
ECG signs of AV dissociation:
- Independent P waves "marching through" QRS complexes at a slower rate
- Capture beats - a rare narrow QRS amid the wide-complex beats when a sinus impulse successfully conducts through to the ventricles (pathognomonic for VT)
- Fusion beats - intermediate-width QRS when a sinus beat partially conducts and fuses with the ventricular beat (also pathognomonic for VT)
Caveat: AV dissociation is pathognomonic for VT but is only visible in ~20-30% of VT cases. Its absence does NOT exclude VT. Also, 1:1 retrograde VA conduction can occur in VT (each QRS followed by a retrograde P) - this does NOT mean SVT.
Three VT ECGs Showing Brugada Criteria Applied (Rosen's Emergency Medicine):
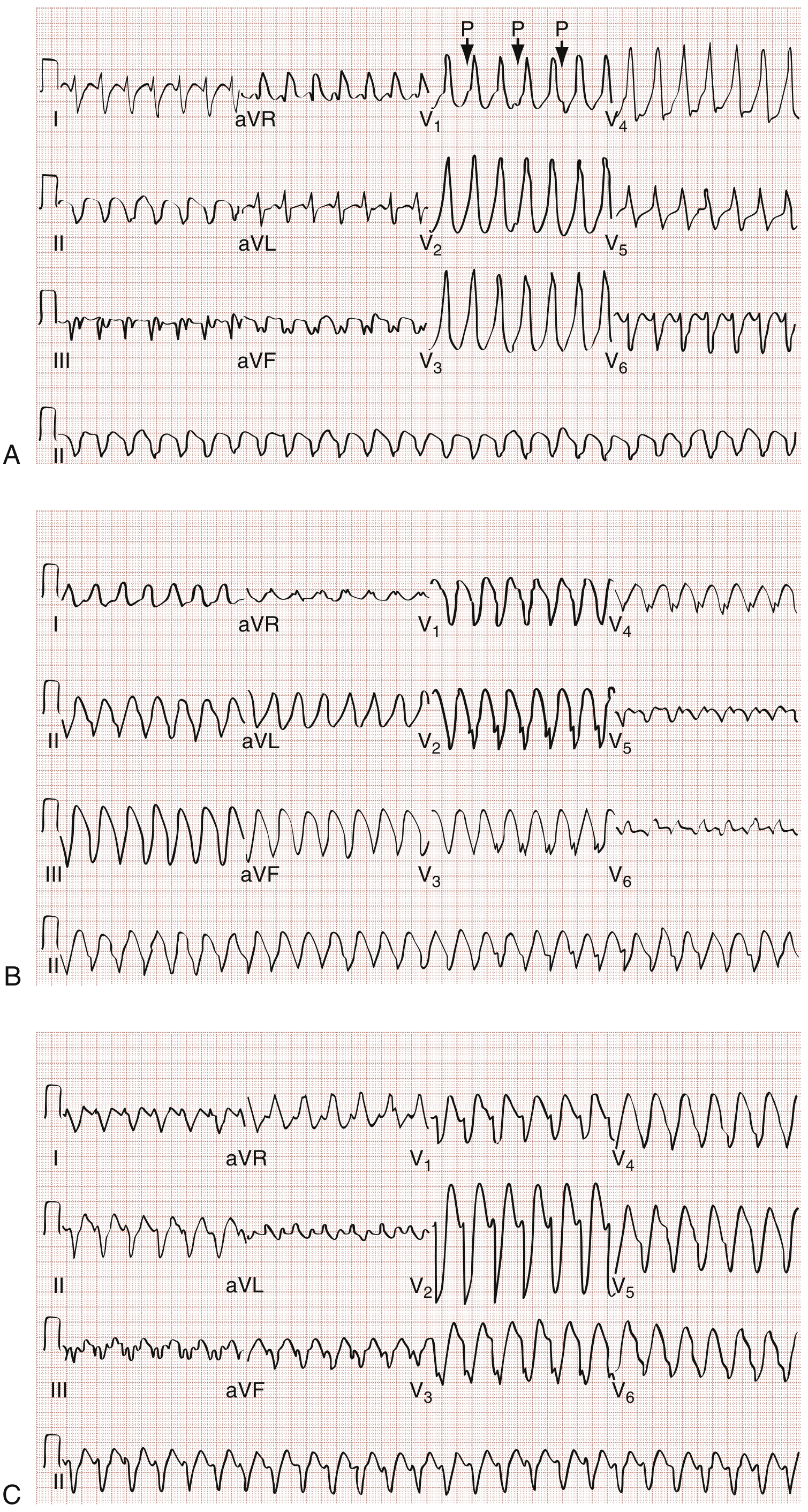
(A) RS complexes present, RS duration >100 ms → VT by criterion 2. AV dissociation also visible (P waves marked with arrows in V1). V6 QRS confirms VT morphology.
(B) RS present, duration ≤100 ms, no AV dissociation visible → proceed to criterion 4. Notched S in V1 + QR in V6 = morphology criteria positive = VT.
(C) Diagnosed by morphologic criteria alone: notched S in V1/V2 and QS in V6 = VT.
Criterion 4 - QRS Morphology Criteria for VT in V1-2 AND V6
This is the most detailed criterion. First determine whether the QRS looks RBBB-like (positive/tall in V1) or LBBB-like (negative/deep in V1), then apply the specific pattern rules for both V1/V2 and V6 simultaneously. Both must show VT patterns.
Morphology Images (Rosen's - Criterion 4A = RBBB-like; 4B = LBBB-like):
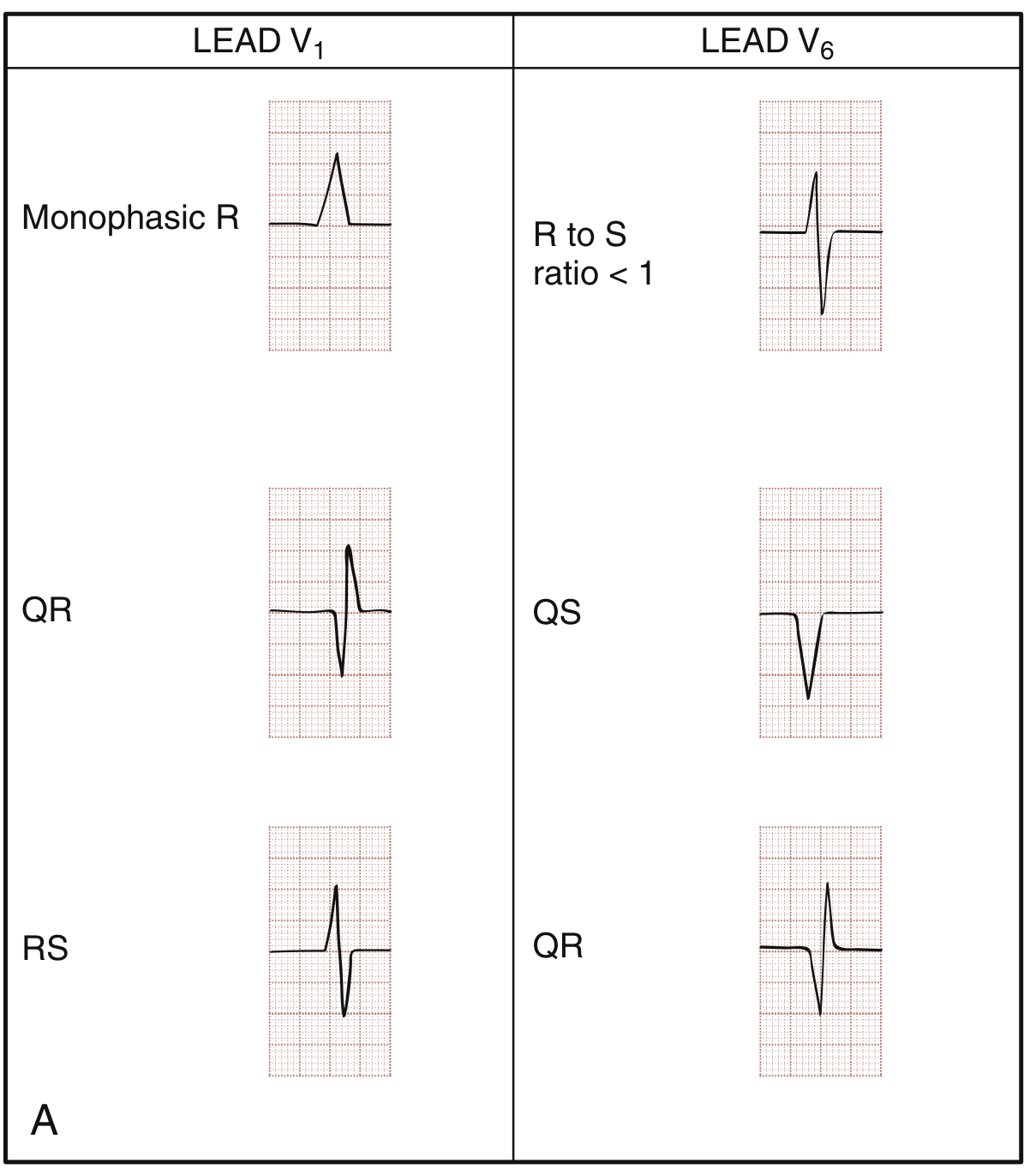
RBBB-like WCT (V1 mainly positive)
| Lead | VT pattern | SVT/True RBBB pattern |
|---|---|---|
| V1 | Monophasic R wave | rSR' (classic triphasic - second R taller: R' > r) |
| V1 | QR pattern | rSR' with R' > r |
| V1 | RS where R > S (fat first rabbit ear) | rSR' with R' dominant |
| V6 | R to S ratio < 1 (S is dominant) | Typical qRs (small q, big R, small s) |
| V6 | QS pattern | qRs |
| V6 | QR pattern | qRs |
Memory hook for RBBB-like VT:
- V1: "Wrong rabbit ear" - the FIRST hump (R) is taller than the second (R'), or no second hump at all (monophasic R)
- V6: Deep S or Q wave - ventricle depolarizing away from V6 (opposite to normal)
LBBB-like WCT (V1 mainly negative)
| Lead | VT pattern | SVT/True LBBB pattern |
|---|---|---|
| V1 or V2 | Initial r wave ≥ 30 ms wide (broad r) | Clean, narrow r or absent r |
| V1 or V2 | Notching or slurring on the downstroke of S wave | Smooth, clean descent to S nadir |
| V1 or V2 | R to S nadir time >70 ms | R to S nadir <70 ms |
| V6 | Any Q wave present (QR or QS) | Pure R wave with no Q |
Memory hook for LBBB-like VT:
- V1/V2: The descent to S nadir is slow and dirty (notched, wide initial r, delayed nadir) - slow cell-to-cell spread
- V6: Any Q wave = VT. True LBBB never has a Q in V6.
Washington Manual Summary Table (LBBB vs RBBB criteria):
| LBBB-like | RBBB-like | |
|---|---|---|
| VT - V1/V2 | r ≥0.04s; notched S downstroke; delayed S nadir >0.06s | Taller left peak (R>R'); biphasic RS or QR |
| SVT - V1/V2 | Absence of above (clean rS or QS, rapid S nadir) | Triphasic rSR' or rR' |
| VT - V6 | Monophasic QS or any Q wave (QR) | R to S ratio <1; QR; QS |
| SVT - V6 | R wave with no Q wave | Typical qRs |
Additional High-Yield ECG Signs (Non-Brugada)
Concordance
Positive concordance - ALL precordial leads V1-V6 show upright (positive, all R waves) QRS = VT (strongly)
Negative concordance - ALL precordial leads show downward (negative, all QS or rS) QRS = VT (strongly, often apical origin)
Positive Concordance ECG (Symptom to Diagnosis, 4th ed.):
Positive concordance: all V1-V6 are upright with large positive deflections, no RS transition. Highly specific for VT.
Extreme ("Northwest") Axis
- QRS axis between -90° and ±180° (negative in both lead I and aVF)
- "No man's land" axis - never produced by normal or BBB conduction
- Strongly favors VT
QRS Duration
-
160 ms in RBBB-like = strongly VT (LR+ 22.9 for QRS >160 ms per Symptom to Diagnosis)
-
140 ms in LBBB-like = favors VT
aVR Criterion (Vereckei 2008)
- Initial R wave in aVR alone = VT
- Initial r or q >40 ms in aVR = VT
- Used as a quick bedside single-lead check
Complete Visual Summary
WIDE COMPLEX TACHYCARDIA (QRS >120 ms, rate >100 bpm)
↓
STEP 1: Any RS complex in V1-V6?
NO (all monophasic) → VT ✓
YES → STEP 2
↓
STEP 2: R-to-S nadir > 100 ms in any lead?
YES → VT ✓
NO → STEP 3
↓
STEP 3: AV dissociation? (independent P waves / fusion / capture beats)
YES → VT ✓
NO → STEP 4
↓
STEP 4: VT morphology in BOTH V1-2 AND V6?
RBBB-like: V1 = mono-R, QR, or RS(R>S) AND V6 = S dominant / QS / QR
LBBB-like: V1/V2 = wide r ≥30ms / notched S / nadir >70ms AND V6 = any Q wave
YES → VT ✓
NO → SVT with aberrancy
Real-World Tips
| Pitfall | Correct Approach |
|---|---|
| "Patient is stable, so it can't be VT" | Stability does NOT rule out VT - treat as VT |
| "There's a P wave after each QRS so it's SVT" | 1:1 retrograde VA conduction can occur in VT |
| "Adenosine converted it so it was SVT" | Rare VT forms (fascicular VT) respond to adenosine |
| Sodium channel toxicity (TCA OD, flecainide) | Causes wide QRS mimicking VT - treat underlying toxicity |
| Hyperkalemia | Produces wide sine-wave QRS - not VT per se |
| Prior BBB on baseline ECG matching tachycardia | Strongly favors SVT with aberrancy |
Sources:
- Rosen's Emergency Medicine, 9th ed. (Table 65.5, Fig. 65.32, 65.33, 65.36)
- Washington Manual of Medical Therapeutics (Fig. 7-2)
- Tintinalli's Emergency Medicine, 9th ed. (Table 18-22)
- Symptom to Diagnosis, 4th ed. (Fig. 31-6, 31-7)
- Original: Brugada P et al. Circulation 1991;83:1649-1659
This is a shared conversation. Sign in to Orris to start your own chat.