Explain anatomy of thyroid gland , cbme curriculum , india mbbs phase 1
Reading File
Finding Sources
Searching the Web
CBME curriculum India MBBS Phase 1 anatomy thyroid gland competencies
Finding Sources
Reading Web Page
https://www.nmc.org.in/wp-content/uploads/2020/01/UG-Curricu…
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, CBME-aligned answer.
Anatomy of the Thyroid Gland
CBME Curriculum — India MBBS Phase 1 (Anatomy)
CBME competency alignment (NMC): The student should be able to describe the gross anatomy, relations, blood supply, nerve supply, lymphatic drainage, and applied anatomy of the thyroid gland (Competency AN 47 / Surgery SU22.1).
1. Development (Embryology)
The thyroid originates from two components:
- Median anlage — endodermal thickening at the base of the tongue (foramen cecum), descends in the midline along the thyroglossal duct
- Lateral anlage — from the 4th–5th pharyngeal pouches; contributes C cells (parafollicular cells)
The two anlagen fuse at the final position anterior to the trachea by the 7th week. Remnants of the thyroglossal duct may persist as a pyramidal lobe (present in 50–75% of individuals) or a thyroglossal duct cyst (midline neck swelling that moves up on tongue protrusion; treated by Sistrunk procedure).
2. Gross Anatomy
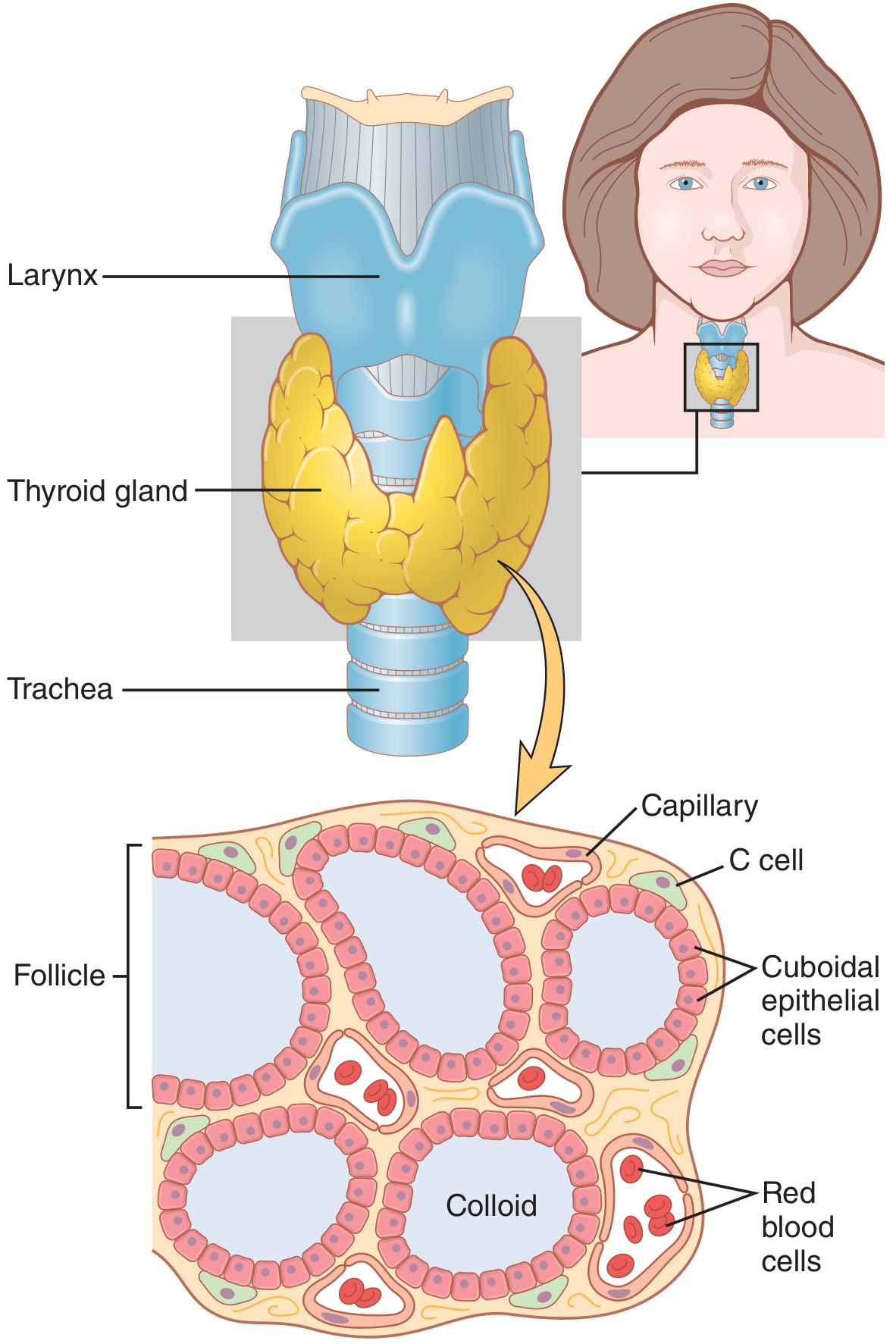
Anatomy and microscopic appearance of the thyroid gland (Guyton & Hall Textbook of Medical Physiology)
Shape, Size, and Weight
| Parameter | Value |
|---|---|
| Shape | Butterfly / H-shaped |
| Weight (adult) | 20–30 g (females slightly heavier) |
| Each lobe height | 4–6 cm |
| Lobe transverse/AP dimensions | 1.3–1.8 cm |
| Isthmus thickness | 2–3 mm |
| Color | Reddish-brown |
| Consistency | Rubbery/firm |
Position
- Lies in the anterior triangle of neck, posterior to the sternohyoid and sternothyroid (strap) muscles
- Isthmus overlies tracheal rings 2–4, just caudal to the cricoid cartilage
- Each lobe extends from the mid-thyroid cartilage level down to the 5th–6th tracheal rings
Parts
- Right lobe and Left lobe — the major components
- Isthmus — connects the lower poles; lies over tracheal rings 2–4
- Pyramidal lobe — a cranial extension from the isthmus (remnant of thyroglossal duct), present in ~50–75% of individuals
- Tubercle of Zückerkandl — a small posterolateral projection of each lobe; important surgical landmark for the RLN
3. Relations
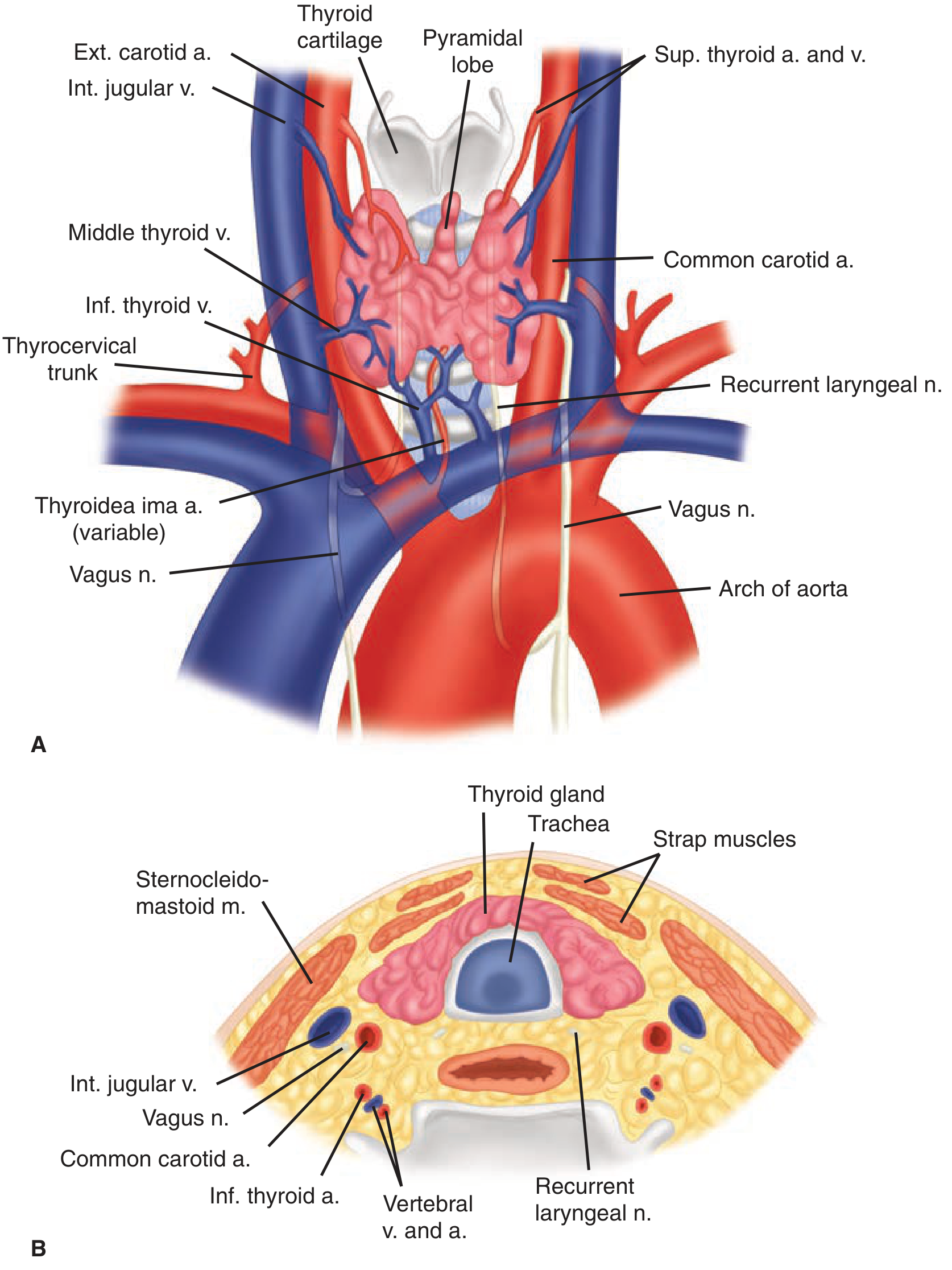
Figure 38-2. Anterior (A) and cross-sectional (B) views of thyroid gland and surrounding structures — Schwartz's Principles of Surgery, 11e
| Surface/Direction | Structures |
|---|---|
| Anterior | Sternohyoid and sternothyroid strap muscles, pretracheal fascia |
| Posterior | Trachea and esophagus (especially left side), parathyroid glands, RLN |
| Lateral | Carotid sheath (common carotid artery, internal jugular vein, vagus nerve), sternocleidomastoid |
| Superior | Cricoid cartilage, inferior pharyngeal constrictor |
| Medial | Trachea, cricoid/thyroid cartilages, cricothyroid muscles |
Capsule & Fascial Coverings
- The gland is invested by pretracheal fascia (forms the true capsule)
- This condenses as the suspensory ligament of Berry (posterior medial), which anchors the gland to the trachea — the RLN passes close to this ligament and may even traverse it in 25% of individuals
- Also forms the anterior suspensory ligament above the isthmus
4. Blood Supply
Arterial Supply
| Artery | Origin | Area Supplied |
|---|---|---|
| Superior thyroid artery (paired) | External carotid artery | Upper poles; divides into anterior and posterior branches at apex of each lobe |
| Inferior thyroid artery (paired) | Thyrocervical trunk (subclavian) | Lower and posterior part of each lobe; passes posterior to carotid sheath, enters midpole |
| Thyroidea ima artery (variable, 1–4%) | Aorta or innominate artery | Enters isthmus or replaces a missing inferior thyroid artery |
The inferior thyroid artery crosses the recurrent laryngeal nerve — this relationship is the most critical surgical landmark during thyroidectomy.
Venous Drainage
Three sets of veins drain the thyroid:
- Superior thyroid veins — run with superior thyroid arteries → drain into internal jugular vein (IJV)
- Middle thyroid veins — most variable; drain laterally → IJV
- Inferior thyroid veins — form a plexus from the inferior poles → drain into brachiocephalic (innominate) veins
5. Lymphatic Drainage
The lymphatic network is rich and extensive. Drainage follows a consistent pattern relevant to thyroid cancer staging and surgery:
- Primary drainage: Perithyroidal nodes in the central neck (Level VI) — bounded superiorly by the hyoid bone, inferiorly by the innominate artery, laterally by the carotid sheaths
- Secondary drainage: Level VI drains into lateral cervical nodes (Levels II, III, IV) along the jugular veins bilaterally
- Upper thyroid/pyramidal lobe → pretracheal and prelaryngeal (Delphian) nodes → Level VI
- Mediastinal nodes may also receive drainage inferiorly
6. Nerve Supply
| Nerve | Origin | Function |
|---|---|---|
| Recurrent laryngeal nerve (RLN) | Vagus (CN X) | Motor to all intrinsic laryngeal muscles except cricothyroid; sensation below vocal cords |
| External branch of superior laryngeal nerve (EBSLN) | Superior laryngeal nerve (branch of vagus) | Motor to cricothyroid muscle (tenses vocal cords; controls pitch) |
| Sympathetic fibers | Middle cervical ganglion | Vasomotor |
RLN course (critical applied anatomy):
- Left RLN: arises from vagus at aortic arch, loops around ligamentum arteriosum, ascends in the tracheoesophageal groove
- Right RLN: arises at right subclavian artery, more oblique course, less predictable
- Non-recurrent RLN: right side in 0.5–1% (associated with aberrant right subclavian artery); left only with situs inversus — a catastrophic surgical surprise
- Both RLNs are most vulnerable near the ligament of Berry and at their crossing with the inferior thyroid artery
7. Histology (Microanatomy)
The thyroid is composed of:
| Structure | Description |
|---|---|
| Follicles | Spherical units, 100–300 µm diameter; the functional unit |
| Follicular cells (principal cells) | Cuboidal/low columnar epithelium; secrete T3 and T4; height varies with activity (tall = active, flat = inactive) |
| Colloid | Proteinaceous material filling follicle lumen; mainly thyroglobulin |
| Parafollicular cells (C cells) | Derived from neural crest; secrete calcitonin; located between follicles or at periphery of follicular epithelium |
| Rich capillary network | Blood flow ~5× gland weight/minute — one of the highest perfusion rates in the body |
8. Applied Anatomy (Clinically Important)
| Condition | Anatomical Basis |
|---|---|
| Thyroglossal duct cyst | Persistence of thyroglossal duct; midline, moves up with tongue protrusion or swallowing |
| Lingual thyroid | Failure of median anlage to descend; mass at base of tongue; often the only thyroid tissue |
| RLN palsy after thyroidectomy | Injury during ligation of inferior thyroid artery or at Berry's ligament → hoarseness |
| EBSLN injury | Damage during superior pole ligation → loss of high pitch (cricothyroid denervation) |
| Tracheotomy precaution | Thyroidea ima artery can bleed catastrophically during emergency tracheotomy |
| Retrosternal goiter | Enlargement of substernal thyroid → compresses trachea and esophagus |
| Superior parathyroid | Dorsal to RLN plane (more constant); inferior parathyroid is ventral (more variable) |
| Berry's ligament | RLN passes posterior to it; branches may traverse the ligament in 25% of individuals |
9. CBME Phase 1 Competency Summary (NMC India)
According to the NMC CBME curriculum (Vol. I), the relevant Phase 1 anatomy competency requires the student to:
- Describe the gross anatomy and position of the thyroid gland
- Describe its relations to surrounding structures
- Describe its blood supply, venous drainage, and lymphatic drainage
- Describe the nerve supply with emphasis on the RLN and external laryngeal nerve
- Explain the applied aspects and clinical implications (thyroiditis, goiter, thyroidectomy complications)
- Integrated teaching with Surgery (SU22.1 — applied anatomy and physiology of thyroid)
The topic spans Anatomy (Phase 1) integrated with Physiology (thyroid hormones) and forms the anatomical basis for surgical competencies in Phase 2/3.
Sources:
- Schwartz's Principles of Surgery, 11e — Ch. 38, Thyroid Anatomy
- Sabiston Textbook of Surgery — Ch. 73, Thyroid Embryology and Anatomy
- Mulholland & Greenfield's Surgery, 7e — Anatomy of the Thyroid
- Guyton & Hall Textbook of Medical Physiology — Ch. 77, Physiological Anatomy of the Thyroid Gland
- NMC CBME Curriculum Vol. I (Anatomy competencies; Surgery SU22.1)
This is a shared conversation. Sign in to Orris to start your own chat.