Classify orthosis based on anatomical location and function with example and proper diagrams
orthosis classification anatomical location function types examples
orthosis classification anatomical location types diagram
AFO ankle foot orthosis KAFO knee ankle foot orthosis HKAFO types
spinal orthosis cervical thoracolumbosacral TLSO CTLSO scoliosis brace
upper limb orthosis wrist hand finger elbow shoulder WHO EWHO
foot orthosis insole rigid soft semirigid plantar support
wrist hand orthosis cock-up resting splint functional position static dynamic
Classification of Orthoses
Classification Framework
| Axis | Categories |
|---|---|
| Anatomical Location | Upper Limb, Lower Limb, Spinal, Head/Cranial |
| Function | Static/Immobilising, Corrective, Functional/Assistive, Protective, Unloading |
A. CLASSIFICATION BY ANATOMICAL LOCATION
I. UPPER LIMB ORTHOSES
1. Shoulder Orthosis (SO)
- Immobilises or supports the glenohumeral joint
- Examples: Shoulder abduction brace (for rotator cuff repairs); gunslinger splint (shoulder abduction immobiliser)
- Function: Abduction positioning, protection post-surgery
2. Elbow Orthosis (EO)
- Hinged designs provide ligamentous stability; dynamic spring-loaded designs treat flexion/extension contractures
- Examples:
- Hinged EO — lateral epicondylitis, UCL instability
- Dynamic EO — flexion/extension contractures (spring-loaded hinge)
- Cubital tunnel splint — long arm with elbow at 45° flexion for ulnar nerve decompression

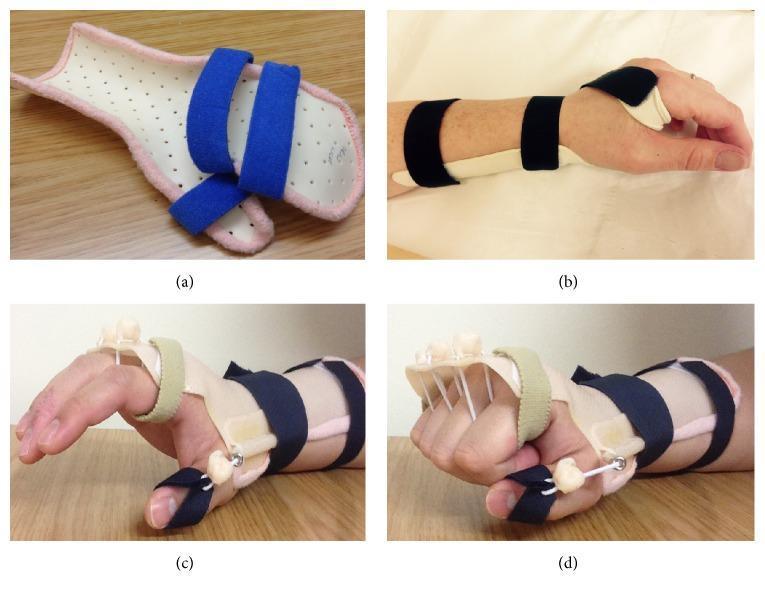
3. Wrist-Hand Orthosis (WHO)
- Most commonly used for post-operative and post-injury care; can be static, static-progressive, or dynamic
- Examples:
- Static resting splint — wrist in neutral extension, MCPs partially flexed, thumb abducted; prevents contractures in stroke/spasticity
- Wrist cock-up splint — wrist extension support; carpal tunnel syndrome, radial neuropathy
- Opponens splint — prepositions thumb for functional prehension
- Wrist-driven tenodesis orthosis — for C6/C7 quadriplegia; tenodesis action converts wrist extension into finger flexion (prehension)
- Dynamic MCP extension orthosis — radial nerve palsy (wrist/finger drop)
II. LOWER LIMB ORTHOSES
1. Foot Orthosis (FO)
- Used to align and support the foot, prevent/correct/accommodate deformities, and improve foot function
- Three types:
- Rigid FO — limits joint motion, stabilises flexible deformities
- Semirigid FO — partial support + shock absorption
- Soft FO — best shock absorption; accommodates fixed deformities (neuropathic, dysvascular, ulcerative foot)
- Examples: Custom arch insoles for pes planus; diabetic pressure-relief insoles; heel cups for plantar fasciitis
2. Ankle-Foot Orthosis (AFO)
- Most commonly prescribed lower limb orthosis; can be metal/shoe design or thermoplastic elastomer (TPE)
- Indications: Foot drop, plantar spasticity, spinal cord injury, post hindfoot fusion
- Types:
- Rigid AFO — prevents all ankle motion; maximum control
- Articulating (hinged) AFO — allows dorsiflexion while blocking plantar flexion
- Posterior leaf spring AFO — flexible; assists dorsiflexion in swing phase (foot drop)
- Ground reaction AFO — blocks ankle dorsiflexion to stabilise knee in quadriceps weakness
- Dynamic AFO — carbon fibre spring; energy storage and return during gait

3. Knee Orthosis (KO)
- A subset of the KAFO system; provides mediolateral stability, patellar control, or post-operative protection
- Examples:
- Knee immobiliser — post-operative stabilisation
- Hinged KO — ACL/MCL ligament injuries; controlled ROM brace
- Unloading KO (toothed segment joint) — knee OA; offloads medial or lateral compartment
- Patellar stabilising brace — patellofemoral syndrome
4. Knee-Ankle-Foot Orthosis (KAFO)
- Extends from upper thigh to foot; controls unstable knee + ankle/foot
- Indications: Polio, paraplegia (L3–L4 lesion), quadriceps paralysis
- Knee locks: Drop lock, Swiss lock, stance control (free swing + locked stance)
- Examples: Metal double upright KAFO; thermoplastic KAFO with drop lock; carbon fibre KAFO with swing-phase release
5. Hip-Knee-Ankle-Foot Orthosis (HKAFO)
- Extends from pelvis to foot; provides hip and pelvic stability
- Used in children with upper lumbar myelomeningocele (L1–L2); rarely used in adult paraplegics (too cumbersome)
- Reciprocating Gait Orthosis (RGO) — modified HKAFO; hip cable linkage creates alternating hip flexion for simulated walking
- Pavlik harness — paediatric HKAFO variant for developmental dysplasia of the hip (DDH)
6. Hip Orthosis (HO)
- Examples: Hip abduction brace (Legg-Calvé-Perthes disease containment); post-THR abduction orthosis (dislocation prevention)
III. SPINAL ORTHOSES
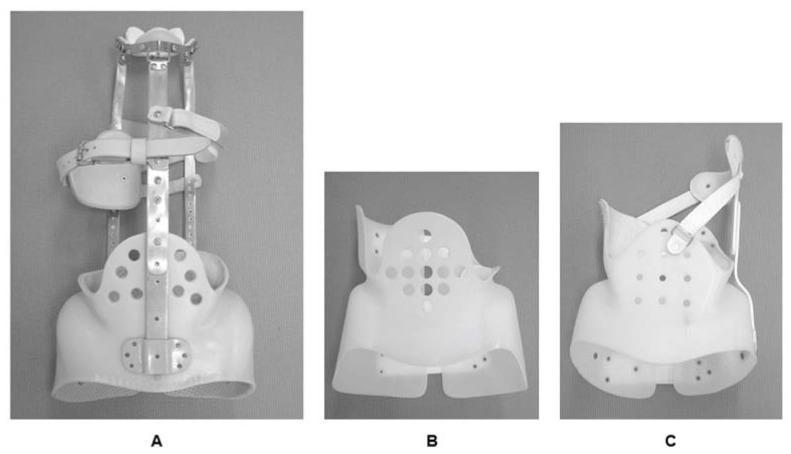
1. Cervical Orthoses (CO / CTO / CTLSO)
| Type | Design | Immobilisation Level | Example |
|---|---|---|---|
| Soft collar | Foam, no rigid support | Minimal (proprioceptive) | Cervical muscle strain |
| Philadelphia collar | Rigid anterior + posterior shells | Moderate | C-spine minor instability |
| SOMI brace | Sternal-occipital-mandibular immobiliser | Moderate-high | Post-cervical fusion |
| Halo vest | Skull pins + vest | Maximum | Unstable C-spine fractures, odontoid fractures |
| CTO (Cervicothoracic) | Extends to thorax | High | C7–T1 injuries |
- Cervical orthoses use three-point pressure: mandible and occiput proximally; clavicle and sternal notch anteroinferiorly
- The halo vest achieves the most stability by direct skull fixation
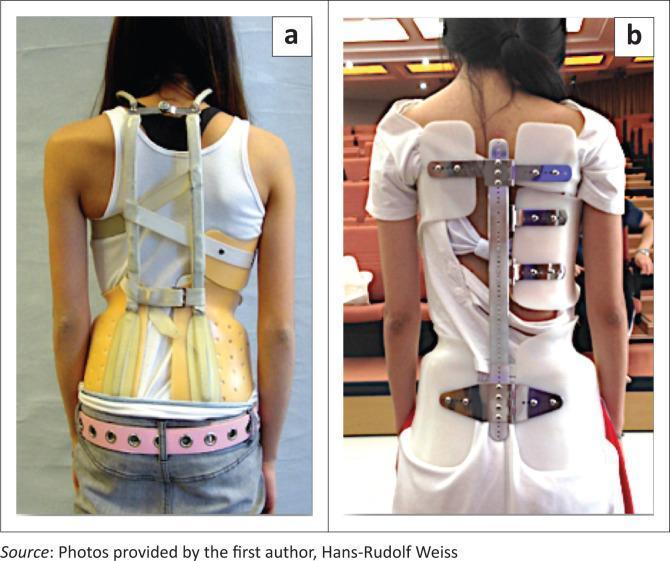
2. Thoracolumbosacral Orthosis (TLSO)
- Stabilises the thoracolumbar spine via three-point pressure + increased body cavity pressure
- Indications: Scoliosis, vertebral fractures, post-spinal surgery, osteoporotic compression fractures
- Milwaukee brace (CTLSO) — cervical ring + two posterior + one anterior upright + pelvic mold; for curves with apex above T7; original standard brace
- Boston brace (TLSO) — symmetric rigid plastic shell; underarm; for curves apex T7 and below
- Chêneau brace / Rigo-Chêneau — asymmetric 3D corrective TLSO with expansion zones and pressure pads; best evidence for idiopathic scoliosis
- Jewett brace — three-point hyperextension TLSO; limits flexion; thoracolumbar compression fractures
- Knight-Taylor TLSO — restricts flexion, extension, and lateral flexion
- TLSO body jacket — rigid total contact shell; post-surgical stabilisation
3. Lumbosacral Orthosis (LSO)
- Indications: Low back pain, lumbar spondylosis, post-lumbar fusion
- Examples: Lumbosacral corset; rigid LSO (Williams flexion brace — limits extension); LSO chair-back brace
IV. HEAD / CRANIAL ORTHOSES
- Cranial remoulding orthoses (helmets) — used for positional plagiocephaly, brachycephaly, scaphocephaly in infants (0–18 months)
- Function: Gently redirect skull growth by providing contact in prominent areas + freedom in flattened areas
B. CLASSIFICATION BY FUNCTION
| Functional Category | Definition | Examples |
|---|---|---|
| Static / Immobilising | No joint motion allowed; maintains fixed position | Rigid AFO, resting hand splint, hard cervical collar |
| Static-Progressive | Incrementally adjusted to gain range of motion over time | Serial casting equivalent; adjustable elbow EO for contracture |
| Dynamic | Allows or assists joint movement through springs, elastic, or cables | Dynamic WHO, posterior leaf spring AFO, RGO, Saebo Flex |
| Corrective | Applies a force to reduce or correct a deformity | Milwaukee/Boston brace (scoliosis), Denis Browne bar (clubfoot) |
| Functional/Assistive | Substitutes for or augments lost motor function | Wrist-driven tenodesis WHO (quadriplegia), stance-control KAFO |
| Protective / Unloading | Reduces stress on injured or diseased structures | Unloading KO (OA), diabetic pressure-relief FO, fracture brace |
| Proprioceptive/Sensorimotor | Provides afferent input to augment neuromuscular control | Soft ankle brace, sensorimotor foot orthosis |
Summary Diagram (ISO Naming Hierarchy)
ORTHOSES
├── Upper Limb
│ ├── SO — Shoulder Orthosis
│ ├── EO — Elbow Orthosis
│ ├── WHO — Wrist-Hand Orthosis
│ └── FO (finger) — Finger Orthosis
│
├── Lower Limb
│ ├── FO — Foot Orthosis
│ ├── AFO — Ankle-Foot Orthosis
│ ├── KO — Knee Orthosis
│ ├── KAFO — Knee-Ankle-Foot Orthosis
│ └── HKAFO — Hip-Knee-Ankle-Foot Orthosis
│
├── Spinal
│ ├── CO — Cervical Orthosis
│ ├── CTO — Cervicothoracic Orthosis
│ ├── CTLSO — Cervicothoracolumbosacral Orthosis (e.g., Milwaukee)
│ ├── TLSO — Thoracolumbosacral Orthosis (e.g., Boston, Chêneau)
│ └── LSO — Lumbosacral Orthosis
│
└── Head
└── Cranial Remoulding Orthosis (helmet)
Key Clinical Principles
- Orthoses are NOT indicated for fixed deformities or spastic deformities that cannot be manually corrected (Miller's Review of Orthopaedics, 9th ed.)
- Three-point pressure principle — all rigid orthoses use three points of contact to control joint position or alignment
- Material choice — thermoplastic (lightweight, mouldable, used for AFOs/WHO); metal with leather (durability, adjustability for KAFOs); carbon fibre (energy return, dynamic gait orthoses)
- Static vs. dynamic distinction is critical — dynamic orthoses permit functional movement; static devices fully immobilise for healing or prevention
Drawabkw diagram
A detailed medical educational diagram titled "Classification of Orthoses" showing a clean, well-organized flowchart/tree diagram. The diagram has a central box labeled "ORTHOSES" at the top, branching into four main categories: "UPPER LIMB ORTHOSES", "LOWER LIMB ORTHOSES", "SPINAL ORTHOSES", and "HEAD/CRANIAL ORTHOSES". Each category has colored boxes. Under UPPER LIMB ORTHOSES (blue): SO - Shoulder Orthosis (gunslinger brace, abduction brace), EO - Elbow Orthosis (hinged, dynamic spring), WHO - Wrist-Hand Orthosis (resting splint, cock-up splint, tenodesis WHO), FO - Finger Orthosis (mallet finger splint) Under LOWER LIMB ORTHOSES (green): FO - Foot Orthosis (rigid, semirigid, soft), AFO - Ankle-Foot Orthosis (rigid, hinged, posterior leaf spring, ground reaction, dynamic carbon fiber), KO - Knee Orthosis (immobiliser, unloading, hinged), KAFO - Knee-Ankle-Foot Orthosis (drop lock, stance control), HKAFO - Hip-Knee-Ankle-Foot Orthosis (reciprocating gait orthosis, Pavlik harness) Under SPINAL ORTHOSES (orange): CO - Cervical (soft collar, Philadelphia, SOMI, halo vest), CTO - Cervicothoracic, CTLSO - Milwaukee brace, TLSO - Boston brace / Cheneau brace / Jewett brace, LSO - Lumbosacral corset Under HEAD/CRANIAL (purple): Cranial Remoulding Helmet (plagiocephaly, brachycephaly) On the right side, a FUNCTIONAL CLASSIFICATION column with colored labels: Static/Immobilising (red), Static-Progressive (orange), Dynamic/Assistive (green), Corrective (blue), Protective/Unloading (yellow), Proprioceptive (purple) The diagram should be on a white background, with clear connecting lines, colored boxes, and small illustrative icons next to each orthosis type. Clean medical textbook style, professional and educational.
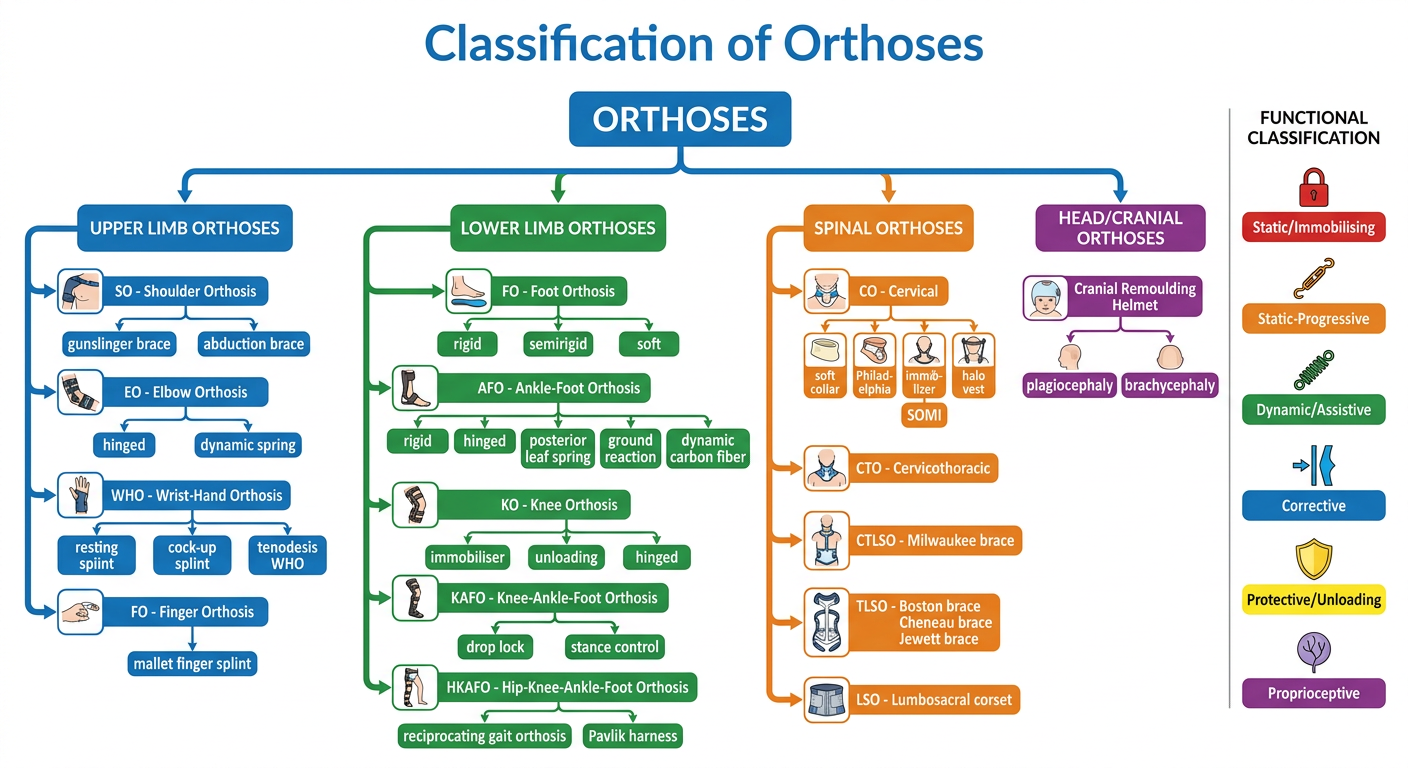
- 🔵 Upper Limb — SO → EO → WHO → Finger FO
- 🟢 Lower Limb — FO → AFO → KO → KAFO → HKAFO
- 🟠 Spinal — CO → CTO → CTLSO → TLSO → LSO
- 🟣 Head/Cranial — Remoulding helmet
- Static/Immobilising, Static-Progressive, Dynamic/Assistive, Corrective, Protective/Unloading, Proprioceptive