Bpt notes
Asking for Preferences
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Lippincott's Pharmacology. Let me compile the full BPT notes.
📘 BPT 2nd Year - General Pharmacology Notes
Source: Lippincott Illustrated Reviews: Pharmacology
UNIT 1: PHARMACOKINETICS
"Pharmacokinetics refers to what the body does to a drug."
The four pharmacokinetic processes are remembered as ADME:
| Process | What It Means |
|---|---|
| Absorption | Drug enters the blood from site of administration |
| Distribution | Drug moves from blood into tissues |
| Metabolism | Drug is chemically transformed (mainly in liver) |
| Elimination | Drug/metabolites are excreted from the body |
CHAPTER 1: PHARMACOKINETICS
I. Routes of Drug Administration
Routes are chosen based on the drug's properties (lipid/water solubility, ionization) and the clinical goal (rapid onset vs. sustained effect).
A. Enteral Routes
| Route | Description | Key Features |
|---|---|---|
| Oral (PO) | Swallowed; absorbed from GI tract | Most common, convenient, economical; subject to first-pass effect |
| Sublingual | Under the tongue | Bypasses first-pass; rapid absorption; e.g., nitroglycerin |
| Buccal | Between cheek and gum | Similar to sublingual; e.g., some hormones |
B. Parenteral Routes
| Route | Description | Key Features |
|---|---|---|
| Intravenous (IV) | Directly into vein | 100% bioavailability; fastest onset; used in emergencies |
| Intramuscular (IM) | Into muscle | Medium rate; suitable for depot preparations |
| Subcutaneous (SC) | Under skin | Slower than IM; e.g., insulin, vaccines |
| Intrathecal | Into cerebrospinal fluid | Bypasses blood-brain barrier; used for CNS infections, spasticity |
C. Topical/Other Routes
- Topical: Local effect on skin/mucosa
- Transdermal patch: Systemic effect via skin absorption; rate depends on skin characteristics and drug lipid solubility; e.g., nicotine patch, fentanyl patch
- Inhalation: Rapid absorption; used for respiratory diseases (asthma, COPD); minimizes systemic effects
- Rectal: 50% bypasses portal circulation; useful when oral route not feasible (vomiting, unconscious patient); absorption is often erratic
Clinical relevance for physiotherapy: Transdermal patches (e.g., diclofenac, fentanyl) and topical NSAIDs are commonly used in patients you will encounter in musculoskeletal and palliative care settings.
II. Drug Absorption
Absorption = movement of drug from site of administration into the systemic circulation.
Bioavailability (F)
- The fraction of administered drug that reaches systemic circulation unchanged
- IV administration = 100% bioavailability (F = 1.0)
- Oral bioavailability is often less than 100% due to:
- Incomplete absorption
- First-pass effect - drug is metabolized in the gut wall and liver before reaching systemic circulation
First-Pass Effect (Presystemic Metabolism)
- Oral drugs absorbed from GI tract pass through the portal vein --> liver --> general circulation
- The liver may extensively metabolize a drug before it reaches systemic circulation
- Drugs with high first-pass effect (e.g., morphine, propranolol, nitroglycerin) may need higher oral doses or alternative routes
- Sublingual/rectal routes bypass the liver and avoid first-pass effect
Factors Affecting Absorption
-
Blood flow - Greater blood flow at absorption site = faster absorption
-
Surface area - Small intestine has a large surface area (villi, microvilli) = main absorption site
-
Drug ionization (pH-partition theory)
- Most drugs are weak acids or weak bases
- Only the non-ionized (uncharged) form crosses lipid membranes easily
- Weak acids (e.g., aspirin, pKa 3.5) are better absorbed in the acidic stomach (non-ionized form predominates in acid)
- Weak bases (e.g., morphine, pKa 8) are better absorbed in the alkaline intestine
- Henderson-Hasselbalch equation applies: pH = pKa + log [ionized/non-ionized] for acids
-
Solubility - Drugs must dissolve before absorption; highly lipid-soluble drugs cross membranes easily
-
Drug formulation - Particle size, salt form, enteric coatings all affect dissolution and absorption rate
-
Chemical instability - Penicillin G is unstable in gastric acid; insulin is destroyed by GI enzymes
Bioequivalence
- Two formulations are bioequivalent if they show comparable bioavailability and similar times to reach peak blood concentrations
- Therapeutic equivalence requires bioequivalence + pharmaceutical equivalence (same dosage form, same active ingredient, same route)
III. Drug Distribution
Distribution = drug reversibly leaves bloodstream and enters extracellular fluid and tissues.
Factors Affecting Distribution
-
Blood flow - High blood flow to "vessel-rich organs" (brain, liver, kidney) leads to rapid drug uptake. Skeletal muscle, adipose tissue get less blood flow.
-
Capillary permeability
- Liver and spleen: large, discontinuous capillaries - large molecules can pass
- Brain: tight junctions form the blood-brain barrier (BBB) - only lipid-soluble drugs or actively transported drugs penetrate
- Example: Levodopa uses a specific transporter to enter the brain
-
Plasma protein binding
- Many drugs bind to plasma proteins (mainly albumin)
- Only the free (unbound) drug is pharmacologically active and can distribute into tissues
- Drug binding is reversible; bound drug acts as a reservoir
- Drugs that are highly protein-bound (e.g., warfarin, valproic acid) can be displaced by other drugs --> dangerous interactions
- In hypoalbuminemia, free drug concentration increases --> risk of toxicity
-
Tissue binding
- Some drugs accumulate in tissues (bone, fat, muscle) acting as reservoirs
- Fat-soluble drugs (e.g., diazepam) accumulate in adipose tissue
Volume of Distribution (Vd)
Vd = Dose / Plasma concentration
- Vd is an apparent (not real) volume
- Low Vd (close to plasma volume ~3-5L): Drug stays in vascular compartment (e.g., heparin, large molecules or highly protein-bound drugs)
- High Vd (hundreds of liters): Drug distributes extensively into tissues (e.g., chloroquine, digoxin)
- Vd formula: Vd = Loading Dose / (Cp × F) or rearranged: Loading Dose = Vd × Cp / F
IV. Drug Metabolism (Biotransformation)
- Primary site: Liver (also GI tract, kidneys, lungs)
- Goals: Convert lipophilic drugs to hydrophilic (water-soluble) metabolites for renal excretion
- Metabolism may: increase, decrease, or have NO effect on pharmacologic activity
- Prodrugs are inactive drugs that become active after metabolism (e.g., codeine --> morphine via CYP2D6; clopidogrel --> active metabolite via CYP2C19)
Phase I Reactions (Functionalization)
- Add or unmask a polar functional group (-OH, -NH2, -SH)
- Types: Oxidation, Reduction, Hydrolysis
- Most common: Cytochrome P450 (CYP) enzyme system (located mainly in liver and GI tract)
CYP System:
| Feature | Detail |
|---|---|
| Major isoforms | CYP3A4/5, CYP2D6, CYP2C8/9, CYP1A2 |
| Most important | CYP3A4 - metabolizes ~50% of all drugs; also present in intestinal mucosa |
| Naming | CYP = gene family; 3 = family number; A = subfamily; 4 = specific isozyme |
Genetic polymorphism:
- CYP2D6: Poor metabolizers can't activate codeine (no analgesia); Ultra-rapid metabolizers convert codeine to morphine rapidly (toxic levels in breastfed infants)
- CYP2C19: Poor metabolizers get reduced antiplatelet effect from clopidogrel
- This forms the basis of pharmacogenomics - personalizing drug therapy based on genetic makeup
CYP Inducers vs. Inhibitors:
| Type | Effect | Examples |
|---|---|---|
| Inducers | Speed up CYP enzymes; reduce drug levels | Rifampicin, phenytoin, carbamazepine, St. John's Wort |
| Inhibitors | Slow down CYP enzymes; increase drug levels (risk of toxicity) | Erythromycin, ketoconazole, grapefruit juice, cimetidine |
Phase II Reactions (Conjugation)
- Phase I metabolite conjugated with an endogenous substrate
- Types: Glucuronidation (most common), sulfation, acetylation, methylation, amino acid conjugation
- Generally inactivates drugs and increases water solubility for excretion
V. Drug Elimination (Excretion)
Primary route: Kidneys (urine)
Renal excretion involves:
- Glomerular filtration (free drug is filtered; protein-bound drug is NOT)
- Active tubular secretion
- Passive tubular reabsorption
Other routes: Bile/feces, lungs (volatile anesthetics), saliva, sweat, breast milk
Clinical note: Patients with renal dysfunction cannot excrete drugs efficiently -> drug accumulation -> toxicity. Dose reduction is required.
VI. Pharmacokinetic Parameters
Half-Life (t½)
- Time for plasma drug concentration to fall by 50%
- t½ = 0.693 × Vd / Clearance
- Used to determine dosing intervals
- ~4-5 half-lives to reach steady state and ~4-5 half-lives to eliminate a drug from the body
Clearance (CL)
- Volume of plasma cleared of drug per unit time (L/hr or mL/min)
- CL = Rate of elimination / Plasma concentration
- Hepatic + Renal clearance are the main components
Steady State (Css)
- Plasma concentration at which rate of drug input = rate of elimination
- Achieved after ~4-5 half-lives of repeated dosing
- If dose is doubled, Css doubles (linear kinetics)
Loading Dose vs. Maintenance Dose
| Parameter | Purpose | Formula |
|---|---|---|
| Loading dose | Achieve therapeutic levels quickly | LD = Vd × Css / F |
| Maintenance dose | Keep drug at steady state | MD = CL × Css / F (per dosing interval) |
Loading doses are used when rapid onset is needed (e.g., digoxin, loading antibiotics in sepsis).
Zero-Order vs. First-Order Kinetics
| Kinetics | Feature | Example |
|---|---|---|
| First-order | A constant fraction of drug is eliminated per unit time; half-life is constant | Most drugs |
| Zero-order | A constant amount of drug is eliminated per unit time; half-life is NOT constant; drug saturates elimination | Alcohol (ethanol), phenytoin at toxic doses, aspirin at high doses |
CHAPTER 2: PHARMACODYNAMICS
"Pharmacodynamics describes what the drug does to the body."
I. Receptors and Signal Transduction
- Most drugs exert effects by interacting with specialized target macromolecules called receptors
- The drug-receptor complex initiates signal transduction - a cascade of biochemical events producing cellular response
- The magnitude of response is proportional to the number of drug-receptor complexes formed
Types of Drug Receptors
| Receptor Type | Mechanism | Onset | Examples |
|---|---|---|---|
| Ligand-gated ion channels (Type 1) | Drug opens/closes ion channel directly | Milliseconds | Nicotinic ACh receptor, GABA-A receptor |
| G protein-coupled receptors (Type 2) | Drug activates G protein -> 2nd messengers (cAMP, IP3, DAG) | Seconds to minutes | β-adrenergic, muscarinic, opioid receptors |
| Enzyme-linked receptors (Type 3) | Drug activates transmembrane enzyme (e.g., tyrosine kinase) | Minutes to hours | Insulin receptor, growth factor receptors |
| Intracellular/nuclear receptors (Type 4) | Drug crosses membrane -> binds intracellular receptor -> alters gene transcription | Hours to days | Steroid hormone receptors, thyroid hormone receptors |
II. Agonists and Antagonists
Agonists
- Drugs that bind to a receptor AND activate it to produce a response
- Full agonist: Produces maximum possible response (100% efficacy)
- Partial agonist: Produces less than maximum response even at full receptor occupancy; can act as antagonist when competing with a full agonist
- Example: Buprenorphine (partial opioid agonist)
Antagonists
- Drugs that bind to a receptor but do NOT activate it; they block agonists from binding
- Have high affinity but zero/low efficacy
Competitive Antagonism:
- Antagonist competes with agonist for the same receptor binding site
- Effect is reversible by increasing agonist concentration
- Shifts the dose-response curve to the right (parallel shift; same maximum, higher EC50)
- Example: Atropine blocks acetylcholine at muscarinic receptors
Non-competitive (Irreversible) Antagonism:
- Antagonist binds irreversibly or at an allosteric site; cannot be overcome by increasing agonist
- Reduces the maximum response (Emax decreases); shifts curve downward
- Example: Phenoxybenzamine (irreversible alpha-blocker)
III. Dose-Response Relationships
Graded Dose-Response Curve
- As dose increases, response increases up to a maximum
- Plotted as log dose vs. effect (produces a sigmoid/S-shaped curve)
Key parameters:
- EC50 (ED50): Dose producing 50% of maximum effect - measures potency
- Emax: Maximum effect achievable - measures efficacy
Potency vs. Efficacy:
- Potency = how much drug is needed to produce an effect (lower EC50 = more potent)
- Efficacy = maximum effect a drug can produce
- A drug can be highly potent but have low efficacy (e.g., partial agonist) or vice versa
- Clinically, efficacy matters more than potency
Therapeutic Index (TI) / Safety Window
TI = TD50 / ED50 (or LD50 / ED50 in animals)
- TD50: Dose producing toxicity in 50% of population
- ED50: Dose producing therapeutic effect in 50% of population
- High TI = safer drug (e.g., penicillin); Low TI = narrow safety margin (e.g., digoxin, warfarin, lithium, theophylline)
- Drugs with narrow therapeutic index require therapeutic drug monitoring (TDM)
IV. Drug Tolerance and Tachyphylaxis
| Term | Meaning | Mechanism |
|---|---|---|
| Tolerance | Decreasing response to a drug with repeated administration; higher dose needed | Receptor downregulation, receptor desensitization, increased metabolism (enzyme induction) |
| Tachyphylaxis | Rapid tolerance developing within minutes/hours of repeated dosing | Receptor desensitization or depletion of neurotransmitters |
| Cross-tolerance | Tolerance to one drug confers tolerance to pharmacologically related drugs | Example: Tolerance to heroin confers partial tolerance to morphine |
| Physical dependence | Body adapts to drug; withdrawal syndrome occurs on stopping | Seen with opioids, alcohol, benzodiazepines |
V. Drug Interactions
Pharmacokinetic Interactions
- One drug affects the ADME of another
- Examples:
- CYP inducers (rifampicin) reduce levels of co-administered drugs
- CYP inhibitors (erythromycin) increase levels of co-administered drugs
- Antacids reduce absorption of certain antibiotics (tetracycline chelation)
Pharmacodynamic Interactions
- Drugs interact at the receptor or physiological level
| Type | Definition | Example |
|---|---|---|
| Synergism | Combined effect greater than additive | Alcohol + benzodiazepines (CNS depression) |
| Additive | Combined effect equals sum of individual effects | Aspirin + paracetamol |
| Antagonism | One drug reduces effect of another | Naloxone reverses opioid effects |
VI. Special Pharmacokinetic Considerations
Factors That Alter Drug Response
| Factor | Effect |
|---|---|
| Age (elderly) | Reduced renal/hepatic function; lower Vd for water-soluble drugs; higher sensitivity |
| Age (neonates/children) | Immature liver enzymes; different receptor sensitivity; doses calculated by weight (mg/kg) |
| Pregnancy | Increased plasma volume, altered protein binding, CYP changes; teratogenicity concern |
| Renal failure | Reduced excretion of renally cleared drugs; dose reduction required |
| Hepatic failure | Reduced metabolism; increased bioavailability of high first-pass drugs |
| Obesity | Increased Vd for lipophilic drugs |
| Genetic factors | CYP polymorphisms affect metabolism (see pharmacogenomics above) |
QUICK REVIEW: KEY TERMS TABLE
| Term | Definition |
|---|---|
| Pharmacokinetics | What the body does to the drug (ADME) |
| Pharmacodynamics | What the drug does to the body |
| Bioavailability (F) | Fraction of drug reaching systemic circulation unchanged |
| First-pass effect | Hepatic/GI metabolism before systemic circulation; reduces oral bioavailability |
| Vd | Apparent volume of distribution; reflects extent of drug distribution |
| Half-life (t½) | Time for plasma concentration to fall by 50% |
| Clearance (CL) | Volume of plasma cleared of drug per unit time |
| Steady state (Css) | Plasma concentration achieved when rate in = rate out (after ~5 half-lives) |
| Agonist | Drug that binds and activates receptor |
| Antagonist | Drug that binds receptor but blocks activation |
| Potency (EC50) | Dose needed to produce 50% maximal effect |
| Efficacy (Emax) | Maximum effect a drug can produce |
| Therapeutic index | TD50 / ED50; measure of drug safety margin |
| Tolerance | Decreased response with repeated use |
| CYP3A4 | Most important drug-metabolizing enzyme; metabolizes ~50% of drugs |
DIAGRAMS TO KNOW
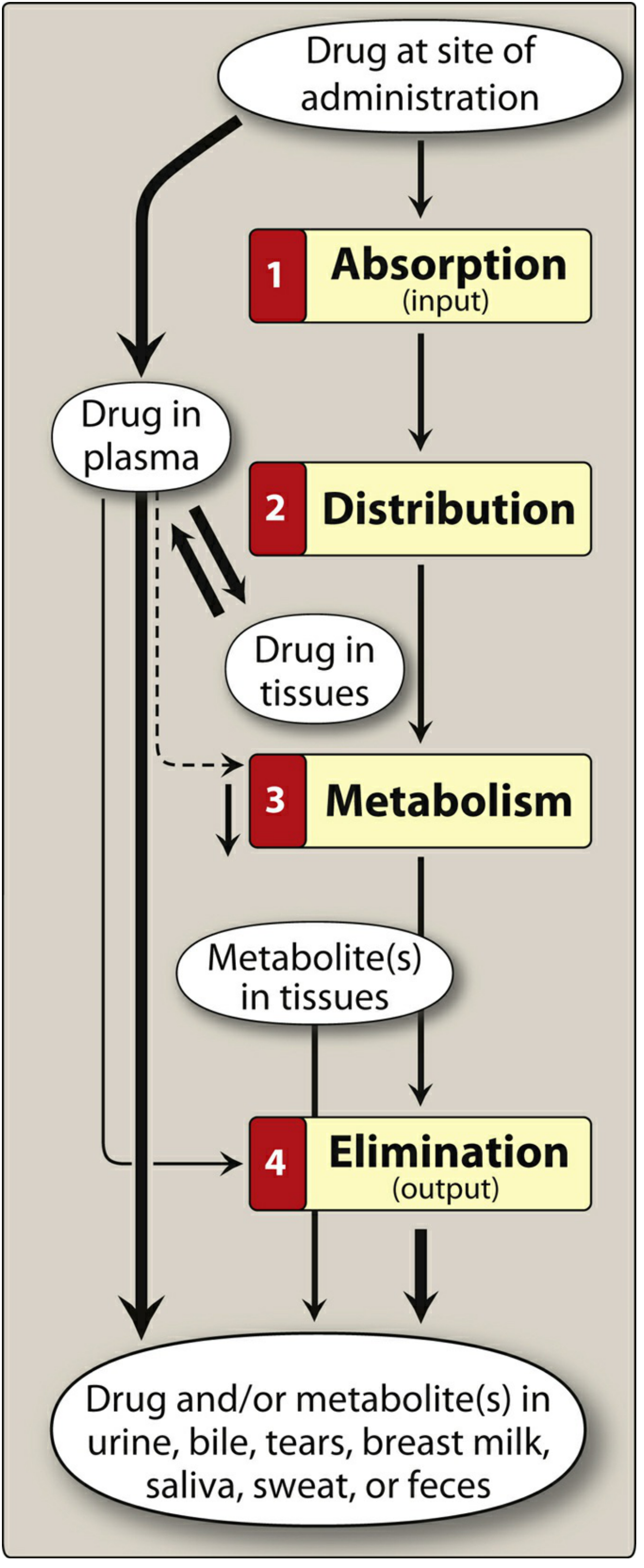
Fig. 1 - Schematic of drug absorption, distribution, metabolism, and elimination (Lippincott's Pharmacology)
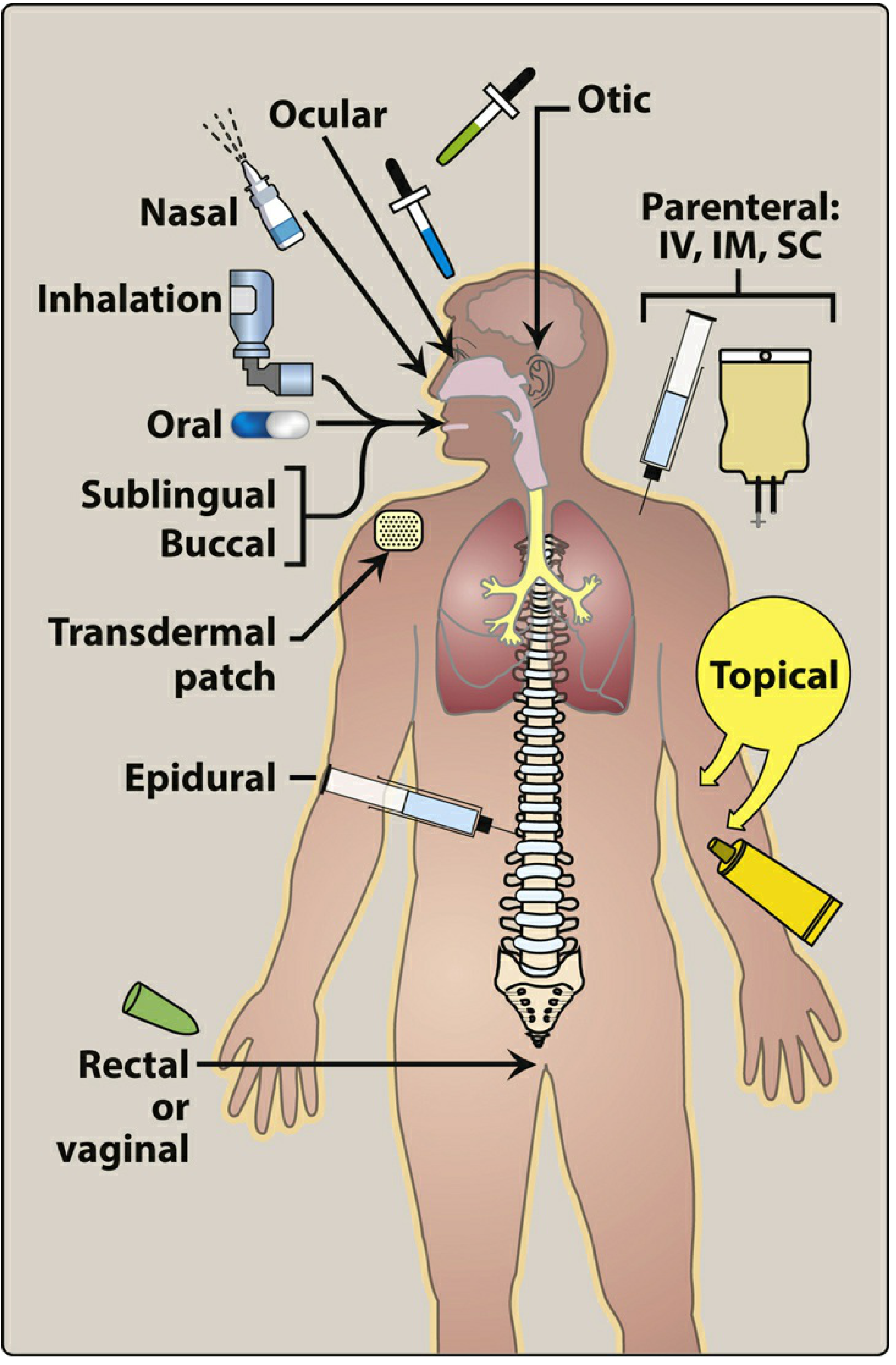
Fig. 2 - Routes of drug administration
IMPORTANT EXAM POINTS FOR BPT
- ADME - the four pharmacokinetic processes; know them in order
- First-pass effect - why nitroglycerin is given sublingually (not orally)
- Ion-trapping - weak acids are absorbed better in the stomach; weak bases in the intestine
- Protein binding - only FREE drug is active; low albumin -> higher free drug -> toxicity risk
- CYP3A4 is the most important drug-metabolizing enzyme; know key inducers and inhibitors
- Half-life determines dosing frequency; 4-5 half-lives to reach steady state
- Narrow therapeutic index drugs (digoxin, warfarin, lithium, theophylline) require monitoring
- Agonist vs. Antagonist - know the types and examples
- Therapeutic index formula: TI = TD50/ED50
- Competitive antagonism shifts dose-response curve to the right without changing Emax; non-competitive reduces Emax
Source: Lippincott Illustrated Reviews: Pharmacology (Chapters 1 & 2 - Pharmacokinetics and Pharmacodynamics)
This is a shared conversation. Sign in to Orris to start your own chat.