Pain pathway
Reading File
Finding Sources
Searching the Web
pain pathway nociception ascending descending anatomy physiology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have rich textbook content and diagrams. Here is a comprehensive answer:
The Pain Pathway
Pain is transmitted from peripheral tissues to conscious perception through a hierarchical, three-neuron system with multiple sites of modulation. It is not a simple "alarm wire" but a dynamically regulated network.
1. Overview: Three-Neuron Chain
Pain is conducted along three neuronal orders from the periphery to the cerebral cortex:
1st-order neuron - peripheral tissue → dorsal root ganglion → dorsal horn
2nd-order neuron - dorsal horn → crosses midline → thalamus (via spinothalamic tract)
3rd-order neuron - thalamus → somatosensory cortex (postcentral gyrus)
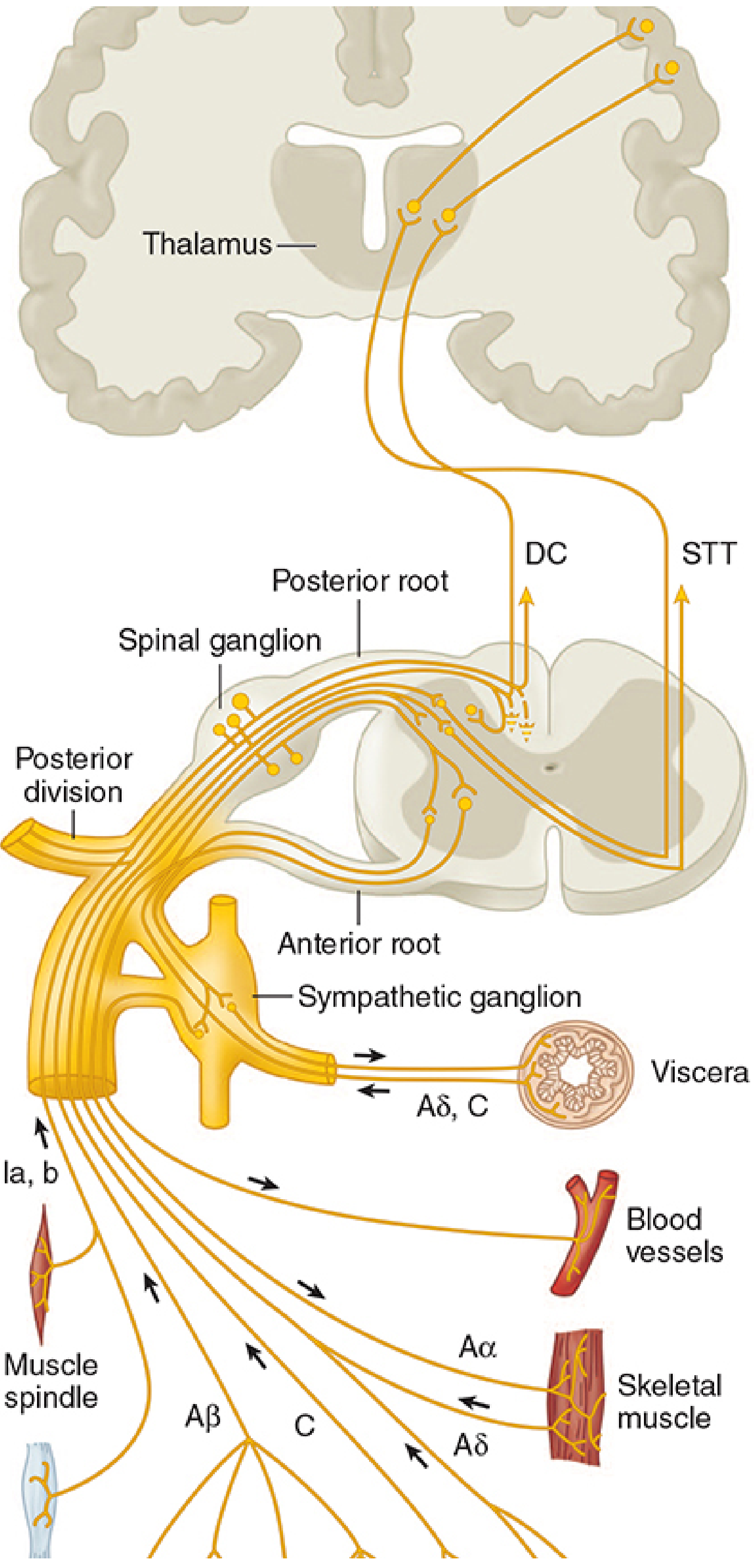
2. Peripheral Nociceptors and Transduction
Noxious stimuli are detected by free nerve endings (nociceptors) found throughout skin, muscle, joints, and viscera. These are the terminals of primary afferent neurons whose cell bodies sit in the dorsal root ganglion (DRG).
Fiber Types
| Fiber | Diameter | Myelination | Conduction | Pain quality |
|---|---|---|---|---|
| Aδ | 2-5 µm | Thin myelin | Fast (5-30 m/s) | Sharp, well-localized ("first pain") |
| C | 0.2-1.5 µm | Unmyelinated | Slow (0.5-2 m/s) | Dull, burning, aching ("second pain") |
Transduction mechanisms - Tissue injury releases a "inflammatory soup" including:
- Bradykinin (from kallidin cleavage in damaged tissue)
- Prostaglandins (PGE2) - sensitize nociceptors
- Serotonin (from platelets)
- Histamine (from mast cells)
- Substance P, CGRP, NGF
- ATP (activates P2X2/P2X3 receptors on muscle nociceptors - mechanism of ischemic muscle pain)
- H+ ions (activate ASIC channels - mechanism of anginal pain via ASIC3)
Key ion channels: TRPV1 (heat, capsaicin, acid), TRPA1 (mechanical, cold, chemicals), piezo2 (mechanosensation), ASICs (acid).
Nociceptor Types
- Cutaneous: high-threshold mechanoreceptors, thermal nociceptors, polymodal (respond to mechanical + thermal + chemical)
- Deep somatic: in muscles and joint capsules; less sensitive than cutaneous but easily sensitized by inflammation; produce dull, poorly localized pain
- Visceral: mostly silent nociceptors activated by smooth muscle spasm, ischemia, and inflammation; few in number but widely distributed; pain referred to somatic regions (e.g., cardiac ischemia → left arm)
3. First-Order Neurons: DRG to Dorsal Horn
The proximal axon enters the spinal cord via the dorsal root. Note: some unmyelinated C fibers anomalously enter via the ventral root, explaining why some patients still feel pain after dorsal rhizotomy.
- Pain fibers travel 1-3 segments in Lissauer's tract before entering the dorsal horn gray matter
- Large Aβ fibers sort medially; small Aδ and C fibers sort laterally upon entering
4. Dorsal Horn Processing (Rexed Laminae)
The dorsal horn gray matter is divided into Rexed laminae I-VI. This is where peripheral input is filtered, modulated, and transmitted upward.
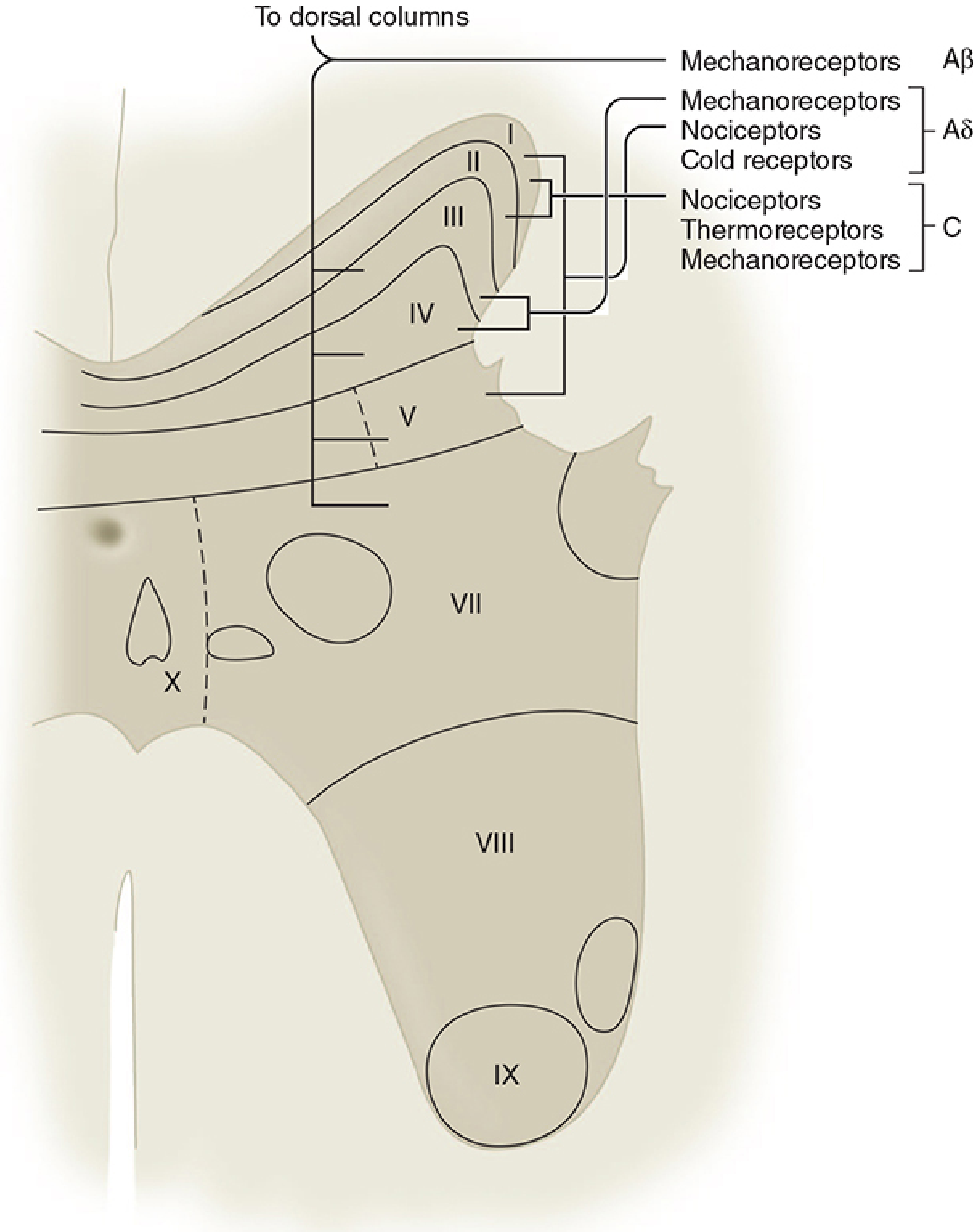
| Lamina | Name | Input | Function |
|---|---|---|---|
| I | Marginal layer | Aδ, C | Nociception, thermoreception |
| II | Substantia gelatinosa | C, Aδ | Nociceptive modulation; major opioid action site |
| III-IV | Nucleus proprius | Aβ, Aδ | Mechanoreception (non-nociceptive) |
| V | Nucleus proprius | Aβ, Aδ, (C) | Visceral + somatic nociception; WDR neurons; referred pain |
| VII | Intermediolateral column | - | Sympathetic preganglionic neurons |
Second-Order Neuron Types
- Nociceptive-specific (NS) neurons - respond only to high-threshold noxious input; somatotopically arranged in lamina I; normally silent
- Wide dynamic range (WDR) neurons - respond to noxious AND innocuous stimuli from Aβ, Aδ, and C fibers; most common in lamina V; show wind-up (exponentially increasing firing rate with repeated stimulation)
Visceral afferents terminate mainly in laminae I and V, convergent with somatic input - this is the basis of referred pain (e.g., cardiac ischemia perceived as arm/jaw pain, appendicitis perceived at the umbilicus before localizing).
5. Ascending Tracts (Second-Order Neurons Upward)
Second-order axons cross the midline via the anterior commissure (taking 2-3 spinal segments to fully decussate - clinically important: a lateral cord lesion affects pain/temperature contralaterally, beginning a few segments below the lesion).
Three Anterolateral Tracts
| Tract | Also called | Terminates | Mediates |
|---|---|---|---|
| Spinothalamic (lateral) | Neospinothalamic | VPL nucleus of thalamus | Discriminative pain: location, intensity |
| Spinothalamic (medial) | Paleospinothalamic | Intralaminar thalamic nuclei | Emotional/affective dimension of pain |
| Spinoreticular | Archispinothalamic | Medullary-pontine reticular formation → centromedian thalamus | Arousal, emotional, autonomic responses |
| Spinomesencephalic | - | Periaqueductal gray (PAG), midbrain | Activates descending inhibition |
The spinothalamic tract occupies the anterolateral white matter with a somatotopic organization: legs most lateral, arms more medial (fibers from the anterior commissure add medially as the tract ascends).
From the VPL, the signal projects via thalamic somatosensory radiations to the primary somatosensory cortex (areas 3, 1, 2) in the postcentral gyrus. Projections to intralaminar/medial thalamic nuclei connect to the limbic system for the emotional "suffering" component.
Facial pain follows an analogous trigeminothalamic pathway - first-order neurons in the trigeminal ganglion (Gasserian) synapse in the spinal nucleus of V, then cross and ascend to the VPM nucleus of the thalamus.
6. Supraspinal Processing
The thalamus is not merely a relay - it has nociceptive-specific neurons with contralateral receptive fields. From here:
- Somatosensory cortex (S1/S2) - pain localization, intensity encoding
- Anterior cingulate cortex (ACC) - emotional/motivational "unpleasantness"
- Insular cortex - autonomic and interoceptive aspects
- Prefrontal cortex - cognitive appraisal, attention
This distributed "pain matrix" explains why pain is simultaneously a sensory event AND an emotional experience.
7. Descending Modulation (Gate Control)
The gate control theory (Melzack & Wall, 1965) - activity in large Aβ fibers can inhibit pain transmission via interneurons in the substantia gelatinosa, "closing the gate."
The descending inhibitory system is an endorphin/enkephalin-based network originating from the cortex and limbic system, with major links in:
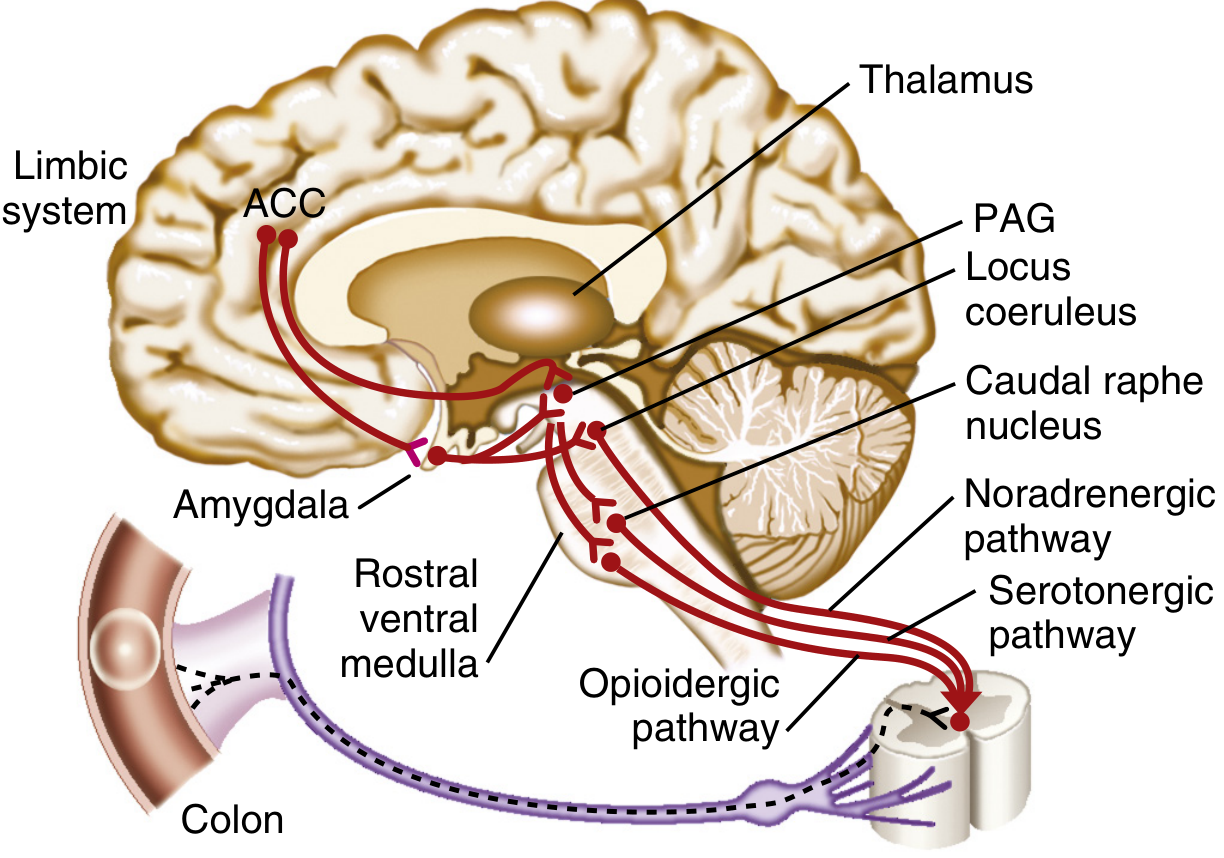
Key stations and neurotransmitters:
- Periaqueductal gray (PAG) - primary relay; responds to endogenous and exogenous opioids
- Locus coeruleus - noradrenergic projections inhibit dorsal horn
- Nucleus raphe magnus / caudal raphe nucleus - serotonergic projections inhibit dorsal horn
- These pathways together produce diffuse noxious inhibitory control (DNIC) - activating pain in one body area inhibits pain throughout the body
Impairment of DNIC is seen in fibromyalgia and other central sensitization syndromes.
8. Central Sensitization
Sustained nociceptive input can cause plastic changes in the dorsal horn:
- Peripheral sensitization - decreased activation threshold of nociceptors, spontaneous discharge, increased response magnitude (primary hyperalgesia)
- Central sensitization - NMDA receptor activation in the dorsal horn produces wind-up, expansion of receptive fields, allodynia (pain from innocuous stimuli), and secondary hyperalgesia
- Neurogenic inflammation - antidromic release of substance P and CGRP from peripheral nociceptor terminals causes vasodilation and plasma extravasation
New gene expression in the dorsal horn can occur within 1 hour of noxious input. The intensity of acute postoperative pain is a predictor of chronic postoperative pain, which is the rationale for preventive multimodal analgesia.
9. Key Neurotransmitters Summary
| Neurotransmitter | Receptor | Effect |
|---|---|---|
| Substance P | Neurokinin-1 | Excitatory |
| CGRP | - | Excitatory |
| Glutamate | NMDA, AMPA, kainate | Excitatory |
| Serotonin (5-HT) | Multiple | Context-dependent (spinal: inhibitory) |
| Norepinephrine | α2-adrenergic | Inhibitory (descending) |
| Enkephalin / Endorphins | µ, δ, κ opioid | Inhibitory |
| GABA | GABA-A/B | Inhibitory |
| Somatostatin | - | Inhibitory |
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Neuroanatomy through Clinical Cases, 3e | Miller's Anesthesia, 10e | Bradley & Daroff's Neurology in Clinical Practice | Sleisenger & Fordtran's GI & Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.