What is petreguem
Searching the Web
petreguem meaning
"Petreguem" doesn't appear to be a recognized word in English or any major language I'm aware of, and the web search didn't find a match either - only results for "petroleum" came up as the closest match.
A few possibilities:
- Typo for "petroleum" - the dark, thick fossil fuel crude oil extracted from underground deposits
- A regional/dialect word - it might be a term from a specific local language or dialect I don't have data on
- A proper noun - a place name, brand, or personal name from a specific region
- A misspelling - could you be thinking of a different word?
Could you share more context about where you came across "petreguem"? For example, is it from a specific language, a book, a game, or a location? That would help me give you a more accurate answer.
What is diabetic retinopathy
Reading File
Finding Sources
Searching PubMed
"diabetic retinopathy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough, textbook-based overview of diabetic retinopathy (DR).
Diabetic Retinopathy
What Is It?
Diabetic retinopathy is a microvascular complication of diabetes mellitus that damages the blood vessels of the retina - the light-sensitive tissue lining the back of the eye. It is the most common cause of new blindness in working-age adults in industrialized countries. Around 40% of all people with diabetes have some degree of DR, and the prevalence in type 2 diabetes reaches 67% after 10 years. With effective screening and treatment, the risk of severe visual loss can be reduced to less than 5%.
- Kanski's Clinical Ophthalmology, 10th ed., p. 521
Normal Retinal Anatomy (Baseline)
The retina relies on a network of fine capillaries supplied by endothelial cells and pericytes (supporting cells that regulate blood flow and vessel integrity).
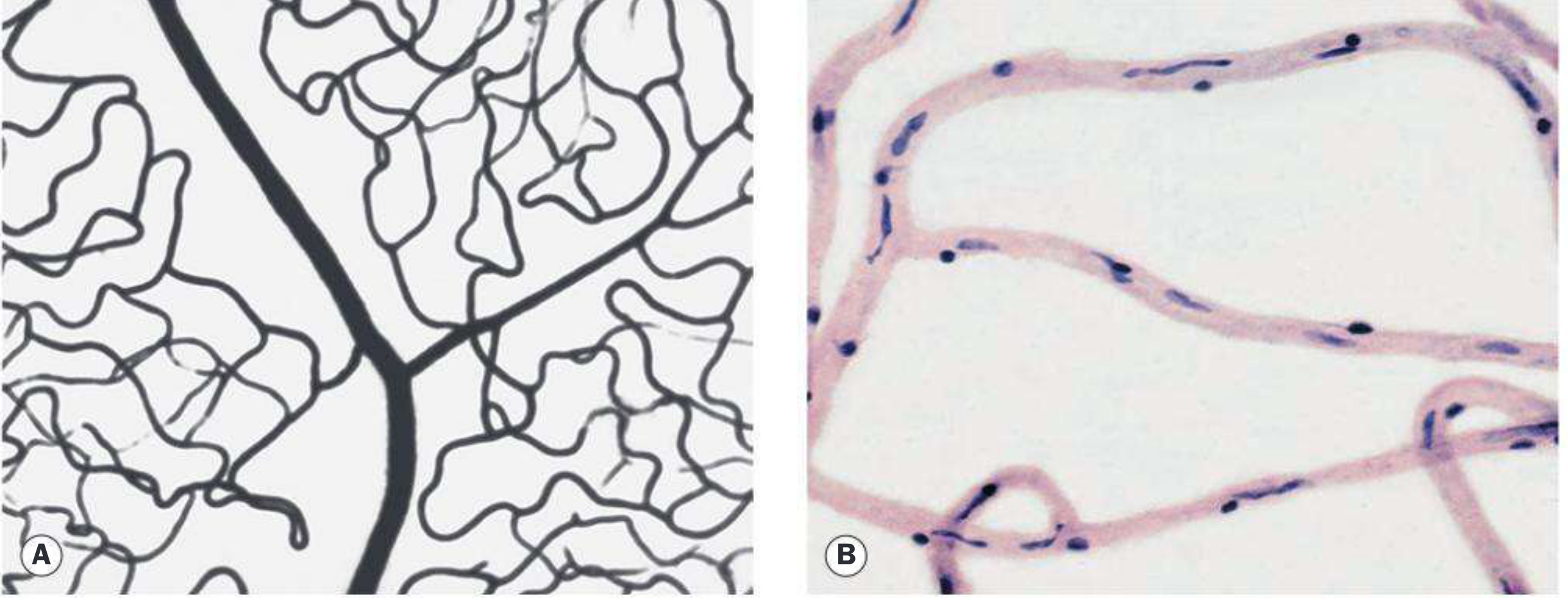
Normal retinal capillary bed - Kanski's Clinical Ophthalmology, p. 521
Pathogenesis (How It Develops)
The primary target tissue is the retinal capillary. Chronic hyperglycemia causes:
- Loss of pericytes - these are directly involved in DR pathogenesis; their loss destabilizes vessel walls
- Basement membrane thickening - weakens capillary structure
- Endothelial dysfunction - increases vascular permeability and promotes leakage
- Localized ischemia - triggers release of VEGF (vascular endothelial growth factor), which drives abnormal new vessel growth (neovascularization)
The result is a cascade of vascular events: microaneurysms, hemorrhages, exudates, macular edema, and eventually proliferative disease.
- Robbins & Kumar Basic Pathology; Textbook of Family Medicine 9e
Classification (Disease Severity Scale)
| Stage | Key Features |
|---|---|
| No apparent retinopathy | Normal fundus |
| Mild NPDR | Microaneurysms only |
| Moderate NPDR | More than mild; may have cotton-wool spots (CWSs) and venous beading |
| Severe NPDR | >20 intraretinal hemorrhages in all 4 quadrants, 2+ quadrants of venous beading, OR 1 quadrant of prominent intraretinal microvascular abnormalities (IRMA) - no PDR |
| PDR (Proliferative DR) | Neovascularization of iris, disc, or retina; vitreous/preretinal hemorrhage |
| Diabetic Macular Edema (DME) | Can occur at any stage; fovea-threatening DME requires treatment |
- The Wills Eye Manual, p. 811-812
Ophthalmic Complications of Diabetes
Common:
- Diabetic macular edema (DME) and macular ischemia
- Retinal ischemia leading to neovascularization and vitreous hemorrhage
- Unstable refraction
Uncommon/Rare:
- Neovascular glaucoma (NVG)
- Tractional retinal detachment
- Accelerated cataract
- Ocular motor nerve palsies
- Papillopathy
Risk Factors
-
Duration of diabetes - the single most important predictor; DR is rare in the first 5 years
-
Poor glycemic control - higher HbA1c = greater risk (DCCT and UKPDS trials confirmed tight glucose control reduces risk)
-
Hypertension - must be controlled to <140/80 mmHg; especially important in type 2 with maculopathy
-
Nephropathy - severe renal disease worsens DR
-
Pregnancy - can accelerate DR, especially if control was poor before pregnancy (up to 1/3 of those with moderate DR progress to PDR during pregnancy)
-
Hyperlipidemia, anemia, cataract surgery - additional risk factors
-
Drugs - pioglitazone is linked to worsening of diabetic macular edema
-
Kanski's Clinical Ophthalmology, p. 521-522
Workup / Investigations
- Slit-lamp examination with gonioscopy (check for neovascularization of iris/angle)
- Dilated fundus examination (90D or 60D lens; indirect ophthalmoscopy for periphery)
- HbA1c, fasting blood sugar, lipid panel
- Blood pressure check
- OCT - evaluates presence and extent of diabetic macular edema (DME)
- IVFA (intravenous fluorescein angiography) - assesses perfusion, foveal ischemia, microaneurysms
- OCT Angiography (OCTA) - non-invasive, detects central macular ischemia
Treatment
Diabetic Macular Edema (DME)
- Anti-VEGF agents - first-line for center-involving DME. FDA-approved agents: ranibizumab, aflibercept; off-label: bevacizumab
- Intravitreal corticosteroids - for suboptimal anti-VEGF response; FDA-approved: dexamethasone implant, fluocinolone acetonide. Side effects: cataract, raised intraocular pressure
- Focal macular laser - for extrafoveal microaneurysms causing edema; also used when injections are contraindicated
Proliferative Diabetic Retinopathy (PDR)
- Panretinal photocoagulation (PRP) - indicated for high-risk characteristics:
- NVD (neovascularization of disc) >1/4-1/3 disc area
- Any NVD with preretinal or vitreous hemorrhage
- NVE >1/2 disc area with hemorrhage
- Any neovascularization of iris (NVI) or angle (NVA)
- Anti-VEGF therapy - alternative to PRP; preferred if DME coexists or vitreous hemorrhage limits the view to the peripheral retina. Note: patients lost to follow-up on anti-VEGF alone have worse outcomes than those receiving PRP.
- The Wills Eye Manual, pp. 813-814
Differential Diagnosis
- Central/Branch Retinal Vein Occlusion (CRVO/BRVO) - typically unilateral, sudden onset; hemorrhages follow venous distribution
- Hypertensive retinopathy - flame-shaped hemorrhages, microaneurysms rare, AV nicking
- Ocular Ischemic Syndrome (OIS) - hemorrhages in midperiphery, no exudates, usually painful
- Radiation retinopathy - develops years after radiation; microaneurysms rare
- Sickle cell retinopathy - peripheral "sea fan" neovascularization
Recent Evidence
A 2025 meta-analysis (PMID 39128789) comparing anti-VEGF vs. panretinal photocoagulation (PRP) for PDR found anti-VEGF injections to be an effective alternative to PRP laser therapy. AI-based screening tools are also rapidly advancing as a systematic approach to earlier DR detection (PMID 38885761).
Key takeaway: Diabetic retinopathy is preventable and treatable. Regular screening, tight glycemic and blood pressure control, and timely use of anti-VEGF therapy or laser treatment are the cornerstones of management.
This is a shared conversation. Sign in to Orris to start your own chat.