Give a short note on dentinal hypersensitivity for 3 marks. Don't give too much long answer, don't give too much short answer. Give answer pointwise and make the answer in such a way that I should get 3 on 3 full marks.
Dentinal Hypersensitivity
- Exposure of dentinal tubules due to gingival recession, enamel erosion, abrasion, or tooth preparation
- Removal of the smear layer (e.g., after scaling and root planing, acid etching)
- Dentine becomes exposed at the cervical region most commonly
- The most widely accepted explanation
- Exposed dentinal tubules are filled with dentinal fluid
- External stimuli (cold, air, osmotic agents) cause rapid inward or outward movement of fluid within the tubules
- This fluid movement activates A-delta nerve fibers at the pulp-dentine junction, producing sharp, transient pain
- C-fibers in the pulp are responsible for the duller, burning component
- Desensitizing toothpastes - contain potassium nitrate (depolarizes nerve fibers) or strontium chloride
- Tubule occlusion agents - fluoride varnishes, oxalate compounds, glass ionomer cement, resin-based bonding agents - physically block exposed tubules
- In-office treatments - laser therapy (Nd:YAG), dentin bonding agents, iontophoresis with fluoride
- Addressing the cause (diet modification, correction of brushing technique, gingival grafting if needed)
Key point to mention for full marks: The hydrodynamic theory by Brannstrom is the accepted mechanism, and treatment is aimed either at blocking the tubules or desensitizing the nerve endings.
I don't like, I don't like that the answer, can you give me, give me more, more proper answer?
Dentinal Hypersensitivity
- Gingival recession - exposes root dentine at the cervical region
- Enamel loss due to erosion (acid diet/GERD), abrasion (aggressive brushing), or attrition
- Tooth preparation, scaling and root planing (removal of cementum and smear layer)
- Cracked tooth syndrome
- Dentinal tubules are filled with dentinal fluid
- External stimuli (cold air, sweet foods, touch) cause rapid inward or outward movement of this fluid
- The fluid movement mechanically activates A-delta nerve fibers located at the pulpo-dentinal junction
- This produces the characteristic short, sharp, transient pain
- The tubules must be open at both ends (at dentinal surface and at the pulp) for this mechanism to operate
| Approach | Examples |
|---|---|
| Nerve desensitization | Potassium nitrate toothpaste (depolarizes nerve endings) |
| Tubule occlusion | Fluoride varnish, strontium chloride, oxalate compounds, glass ionomer cement |
| In-office procedures | Bonding agents, Nd:YAG laser, iontophoresis |
| Surgical | Gingival grafting for severe recession |
Can you please give treatment in point wise answer
Dentinal Hypersensitivity
- Gingival recession - exposes root dentine at the cervical region
- Enamel loss due to erosion (acid diet/GERD), abrasion (aggressive brushing), or attrition
- Tooth preparation, scaling and root planing (removal of cementum and smear layer)
- Cracked tooth syndrome
- Dentinal tubules are filled with dentinal fluid
- External stimuli (cold air, sweet foods, touch) cause rapid inward or outward movement of this fluid
- The fluid movement mechanically activates A-delta nerve fibers at the pulpo-dentinal junction
- This produces a short, sharp, transient pain
- Tubules must be open at both ends for this to occur
- Desensitizing toothpaste containing potassium nitrate - depolarizes nerve endings and blocks pain transmission
- Toothpaste with strontium chloride - occludes dentinal tubules
- Soft-bristled toothbrush with correct brushing technique to prevent further abrasion
- Dietary modification - reduce acidic food and drinks
- Fluoride varnish - precipitates calcium fluoride crystals inside tubules, occluding them
- Oxalate compounds (potassium oxalate) - react with calcium in dentinal fluid to form insoluble crystals blocking tubules
- Glass ionomer cement / resin bonding agents - physically seal and cover exposed dentinal surfaces
- Iontophoresis with fluoride - uses electric current to drive fluoride ions deeper into tubules
- Nd:YAG laser / diode laser - melts and fuses the peritubular dentine, closing tubule openings
- Gingival grafting (connective tissue graft) - indicated when recession is the cause; covers exposed root surface
- Cervical restorations - placement of composite or GIC at the cervical region to cover exposed dentine
Short
Dentinal Hypersensitivity
- Exposed dentinal tubules contain fluid
- Stimuli cause rapid fluid movement inside tubules
- This activates A-delta nerve fibers at the pulpo-dentinal junction
- Results in short, sharp, transient pain
- Potassium nitrate toothpaste - desensitizes nerve endings
- Strontium chloride toothpaste - occludes tubules
- Soft toothbrush + correct technique
- Fluoride varnish - occludes tubules
- Potassium oxalate - blocks tubules with insoluble crystals
- Bonding agents / GIC - seals exposed dentine
- Laser therapy (Nd:YAG) - fuses tubule openings
- Gingival grafting - for recession cases

Give a short note on dentinal hypersensitivity for 3 marks. Don't give too much long answer, don't give too much short answer. Give answer pointwise and make the answer in such a way that I should get 3 on 3 full marks.take refrence from this and alos point by your side
Dentinal Hypersensitivity
-
Hydrodynamic Theory (Brannstrom) - Most Accepted
- Dentinal tubules are filled with fluid
- External stimuli cause rapid inward or outward movement of dentinal fluid
- This fluid movement excites A-delta nerve endings at the pulpo-dentinal junction
- Produces characteristic short, sharp, transient pain
-
Direct Neural Stimulation Theory
- Nerves that enter dentine do not extend beyond the inner two-thirds of dentine
- Direct stimulation of these nerve endings causes pain
-
Transduction Theory
- Stimulation of odontoblastic processes transmits the pain signal to the pulp nerves
- Gingival recession - exposes cervical dentine
- Enamel loss due to erosion, abrasion, or attrition
- Scaling, root planing - removes cementum and smear layer
- Cavity preparation or tooth fracture
- Desensitizing toothpaste with potassium nitrate - blocks nerve depolarization
- Strontium chloride toothpaste - occludes dentinal tubules
- Soft-bristled brush + proper brushing technique
- Fluoride varnish - precipitates calcium fluoride to occlude tubules
- Potassium oxalate - forms insoluble crystals blocking tubule openings
- Bonding agents / GIC - seals exposed dentinal surface
- Laser (Nd:YAG) - fuses and closes tubule openings
- Gingival grafting - for cases with significant recession


Give a short note on age change in dentine for 3 marks. Don't give too much long answer, don't give too much short answer. Give answer pointwise and make the answer in such a way that I should get 3 on 3 full marks.
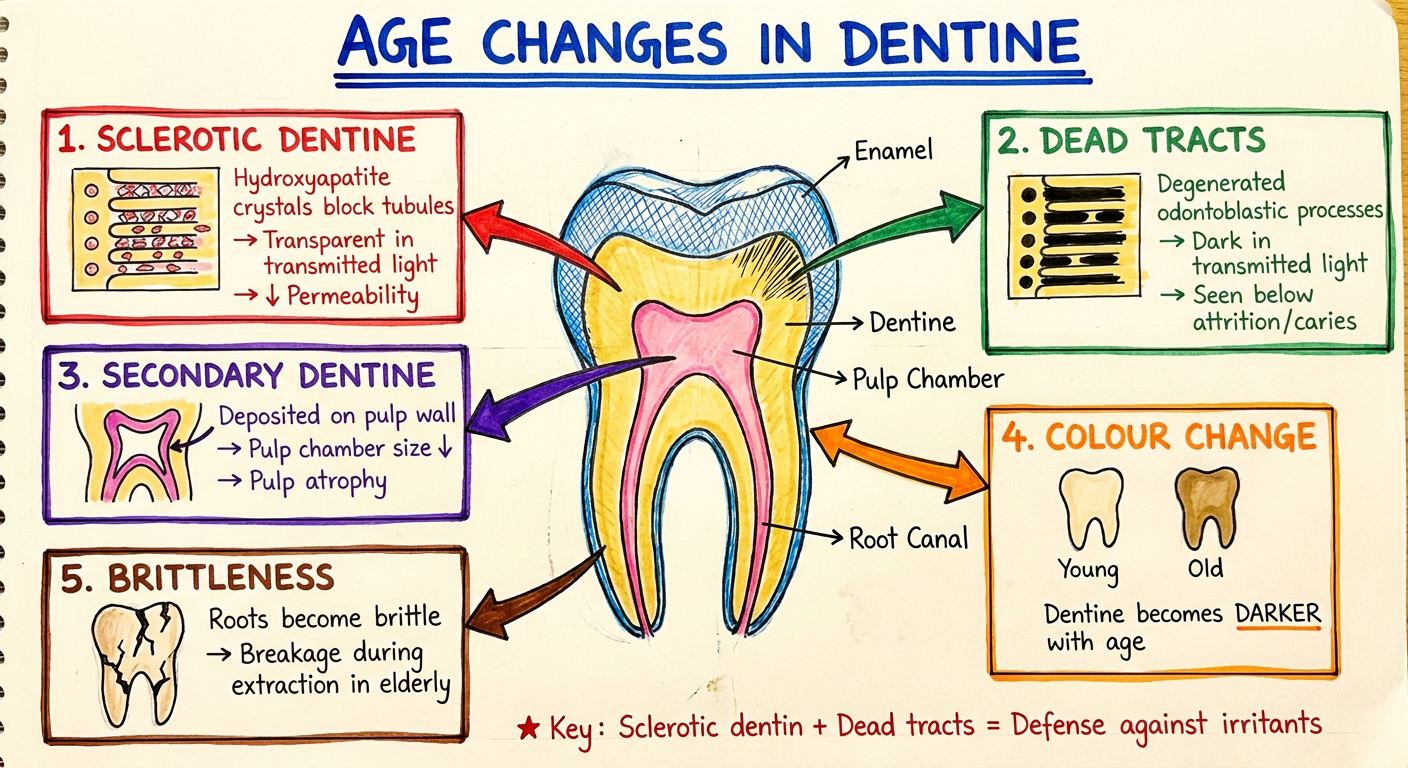
Age Changes in Dentine
- Hydroxyapatite crystals are laid down in the intertubular dentine and within dentinal tubules to block tubule openings
- This prevents entry of bacteria, etc.
- The dentine becomes transparent in transmitted light - hence called transparent or sclerotic dentine
- Permeability of dentine is reduced in these regions
- Areas containing degenerated dentinal tubules that appear dark in transmitted light
- Commonly seen in dentine below attrited, abraded, or carious lesions
- Represent areas where odontoblastic processes have degenerated
- Secondary dentine is deposited over the pulp chamber with age
- This causes pulp atrophy - the size of the pulp chamber decreases progressively with age
- Deposition of peritubular dentin constricts the lumen of dentinal tubules
- Sclerotic dentin deposition decreases tubular fluid volume
- Overall permeability of dentine decreases in elderly teeth
- Dentine becomes darker in colour with age
- Odontoblasts atrophy and may disappear completely under areas of sclerotic dentine
- Roots become brittle during extraction in elderly due to sclerotic changes in apical third
I don't like answer
Age Changes in Dentine
- Hydroxyapatite crystals are deposited inside dentinal tubules and intertubular dentine
- Tubules get blocked, preventing bacterial entry
- Dentine appears transparent in transmitted light
- Permeability of dentine is reduced
- Dentinal tubules containing degenerated odontoblastic processes
- Appear dark in transmitted light
- Seen below areas of attrition, abrasion, or carious lesions
- Laid down on the pulpal wall throughout life
- Causes progressive reduction in pulp chamber size (pulp atrophy)
- Peritubular dentine deposition narrows tubule lumen
- Tubular fluid volume decreases
- Makes dentine less permeable with age
- Dentine becomes darker with age
- Roots become brittle in elderly - breakage during extraction common, especially in apical third
Give sketch colors diagram hand made note style in age change in dentine
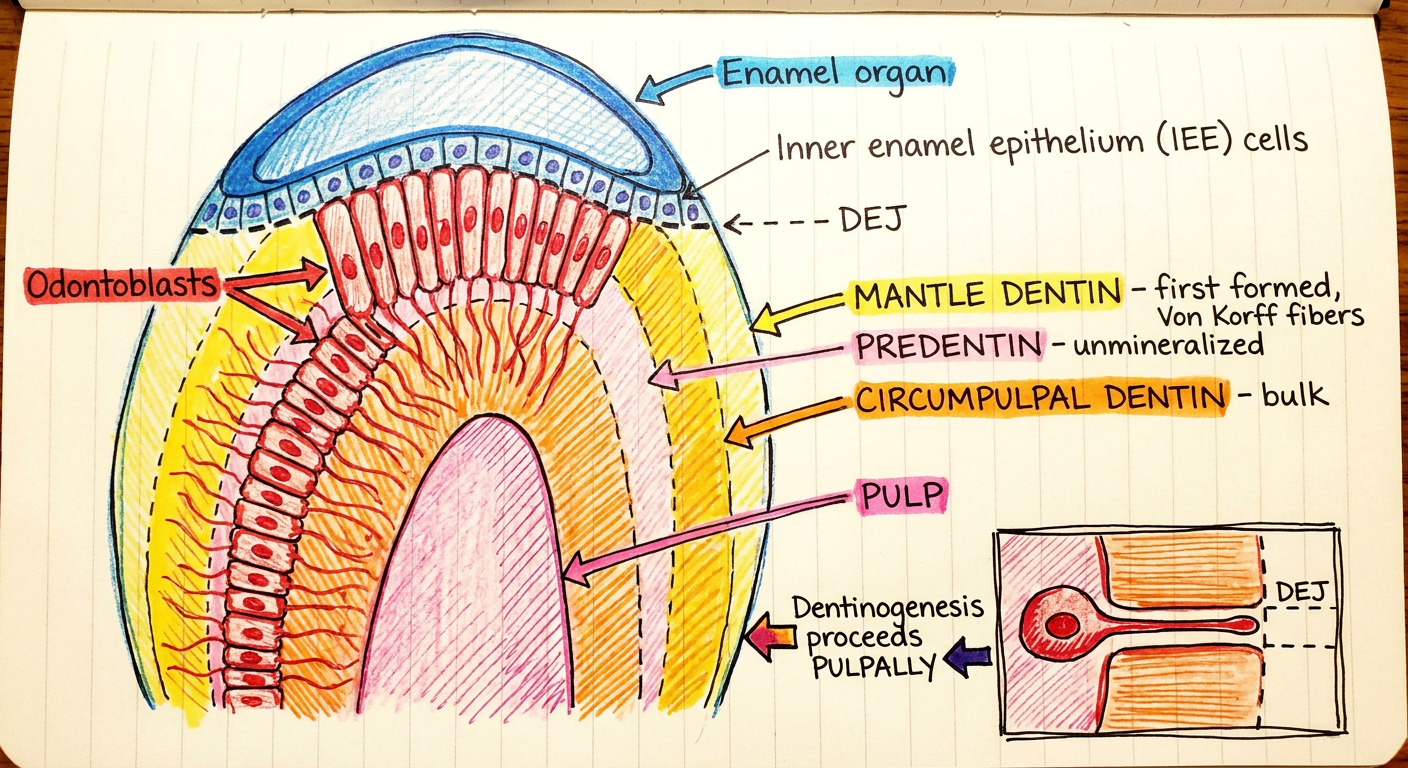
Give sketch colors diagram hand made note style in dentinogenesis
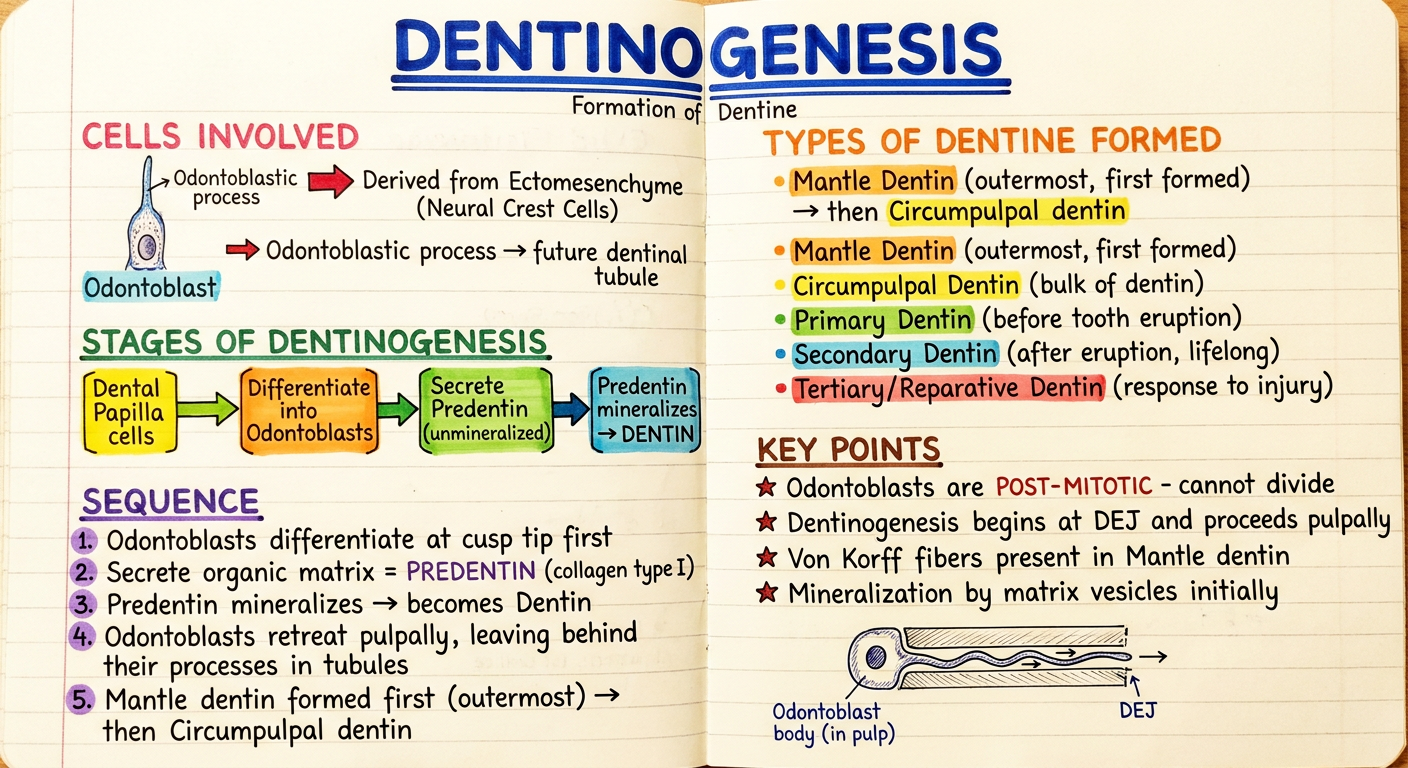
- Cells involved - Odontoblasts from ectomesenchyme
- Stages - Differentiation → Predentin → Mineralized Dentin
- Sequence - Mantle dentin first, then circumpulpal
- Types of dentin - Primary, Secondary, Tertiary
- Key exam points - Von Korff fibers, post-mitotic odontoblasts, DEJ to pulp direction
Only diagram