Explain me 10 common heart diseases with ecg change and ecg images is those diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
10 common heart diseases ECG changes findings images
Reading File
Reading File
Searching the Web
ECG atrial fibrillation ventricular fibrillation heart block LBBB images site:litfl.com OR site:ecgwaves.com
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading Web Page
https://litfl.com/atrial-fibrillation-ecg-library
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG STEMI inferior anterior pericarditis hypertrophy Brugada syndrome images site:litfl.com
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I have gathered all the information I need. Let me now compose the comprehensive answer with ECG images and textbook-based content.
10 Common Heart Diseases: ECG Changes & Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia. Three concurrent electrical changes occur: rapid repolarization in infarcted cells, decreased resting membrane potential, and delayed depolarization - all producing current flow that elevates the ST segment in overlying leads.
ECG Changes:
- Hyperacute T waves - tall, broad, peaked T waves (earliest sign, minutes)
- ST elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in precordial leads - the hallmark finding
- Reciprocal ST depression in leads on the opposite side of the heart
- Q waves develop hours to days after infarction (necrosis marker)
- T-wave inversion follows as the infarct evolves
Localization:
- Anterior (LAD): V1-V4 ST elevation, reciprocal changes in II, III, aVF
- Inferior (RCA/LCx): ST elevation in II, III, aVF
- Lateral (LCx): I, aVL, V5-V6
- Posterior: tall R in V1-V2 + ST depression V1-V3 (mirror image)
"Profound ST elevation or depression in multiple leads usually indicates very severe ischemia." - Harrison's Principles of Internal Medicine 22E, p. 1916
Diagram - Current of Injury:

Figure: A = Subendocardial ischemia causes ST depression in overlying leads. B = Transmural/epicardial ischemia: ST vector points outward, overlying leads show ST elevation.
Inferior STEMI ECG:
Inferior STEMI: Note ST elevation in II, III, aVF (inferior wall) and reciprocal ST depression in I and aVL.
2. Non-STEMI / Unstable Angina (NSTEMI/ACS)
Pathophysiology: Partial coronary occlusion or subtotal stenosis causes subendocardial ischemia. The ST vector shifts toward the subendocardium and ventricular cavity.
ECG Changes:
- ST depression (horizontal or downsloping) - especially in anterior or lateral leads
- T-wave inversions - deep symmetric T-wave inversions in V1-V4 (Wellens sign) indicate critical LAD stenosis
- No Q waves (no full-thickness necrosis in pure NSTEMI)
- ECG may be normal in up to 6% of confirmed NSTEMI
Wellens T-wave sign (critical LAD stenosis):

Wellens T-wave pattern: deep T-wave inversions across precordial leads V1-V6, associated with high-grade LAD stenosis. This is a "STEMI equivalent" requiring urgent catheterization.
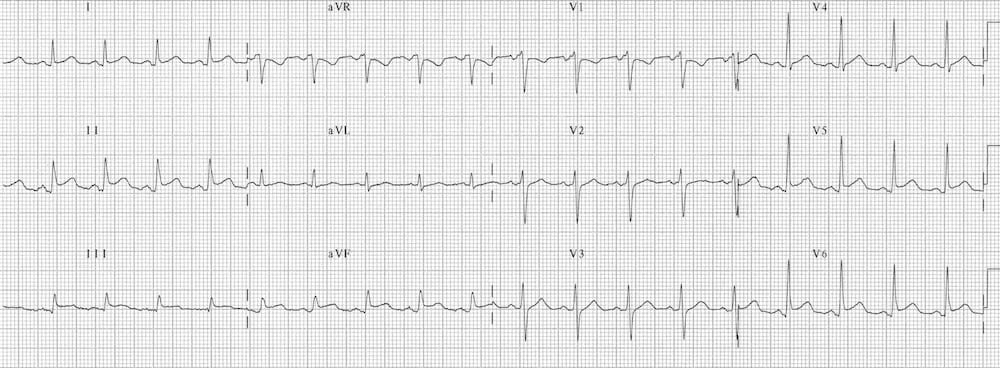
3. Atrial Fibrillation (AF)
Pathophysiology: Disorganized re-entrant circuits throughout the atria at 400-600 impulses/min. The AV node acts as a filter, resulting in an irregular ventricular response.
ECG Changes (Tintinalli's Emergency Medicine):
- Absent P waves - replaced by chaotic irregular fibrillatory baseline (f-waves)
- Irregularly irregular RR intervals - the hallmark
- Narrow QRS complexes (unless pre-existing BBB or accessory pathway)
- Ventricular rate typically 100-160 bpm if uncontrolled
- Rate may be slow if AV nodal disease or medications present
ECG - Atrial Flutter (comparison):
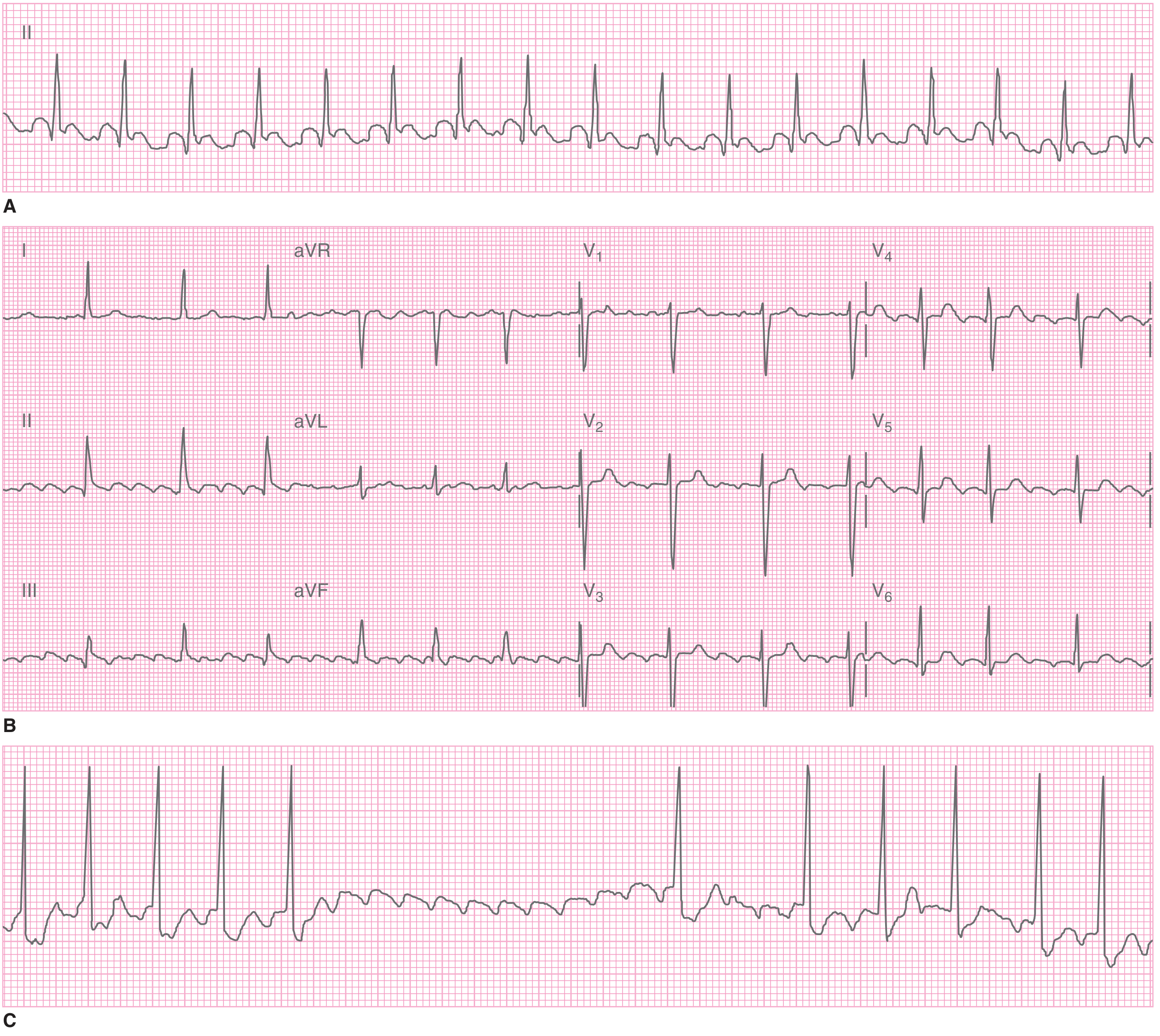
Atrial flutter (closely related to AF): A = Regular tachycardia at 155 bpm (2:1 flutter). B = Classic "sawtooth" flutter waves visible in II, III, aVF. C = Carotid massage reveals flutter waves. AF would show completely chaotic baseline without discrete P waves and completely irregular RR intervals.
4. Left Bundle Branch Block (LBBB)
Pathophysiology: Block in the left bundle branch causes abnormal ventricular depolarization: right ventricle activates first, left ventricle activates late via slow cell-to-cell conduction.
ECG Changes (diagnostic criteria):
- QRS ≥120 ms (broad complex)
- Dominant S wave in V1 (rS or QS pattern) - absence of septal Q in lateral leads
- Tall, broad, notched ("M-shaped") R wave in lateral leads (I, aVL, V5-V6)
- Discordant ST-T changes - ST/T wave in OPPOSITE direction to main QRS deflection
- No septal Q waves in I, V5-V6
Clinical significance:
- New LBBB + chest pain: examine for Sgarbossa criteria (concordant ST changes indicate MI)
- LBBB masks ischemic ECG changes
- Causes: hypertension, cardiomyopathy, aortic stenosis, MI, Lenegre disease
5. Complete Heart Block (Third-Degree AV Block)
Pathophysiology: No conduction from atria to ventricles. The atria and ventricles beat independently - an escape pacemaker (junctional or ventricular) drives the ventricles.
ECG Changes:
- P waves at regular rate (60-100 bpm normal sinus)
- QRS complexes at slower regular rate (30-45 bpm if ventricular escape; 40-60 bpm if junctional)
- Complete AV dissociation - P waves and QRS have no fixed relationship, P waves "march through" QRS
- QRS morphology: narrow if junctional escape, wide and bizarre if ventricular escape
- PR intervals vary randomly (no fixed PR)
Causes: Inferior MI (often transient due to RCA ischemia), Lyme disease, congenital, digoxin toxicity, calcific aortic stenosis, cardiac surgery.
6. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes diffuse epicardial injury. Unlike STEMI (regional), pericarditis causes widespread ST changes in almost all leads except aVR and V1.
ECG Changes (four stages):
- Stage 1: Diffuse concave ("saddle-shaped") ST elevation in I, II, III, aVF, aVL, V2-V6 + PR segment depression (pathognomonic) - due to atrial injury
- Stage 2 (days): ST normalizes, PR still depressed, T waves flatten
- Stage 3: T-wave inversions
- Stage 4 (weeks): ECG normalizes
Key differentiator from STEMI:
- Saddle-shaped (concave) vs. convex ST elevation in STEMI
- No reciprocal ST depression (except aVR shows ST elevation + PR elevation)
- PR depression present
Acute pericarditis: widespread ST elevation with concave (saddle-shaped) morphology across multiple leads, with PR depression - distinguishes this from focal STEMI.
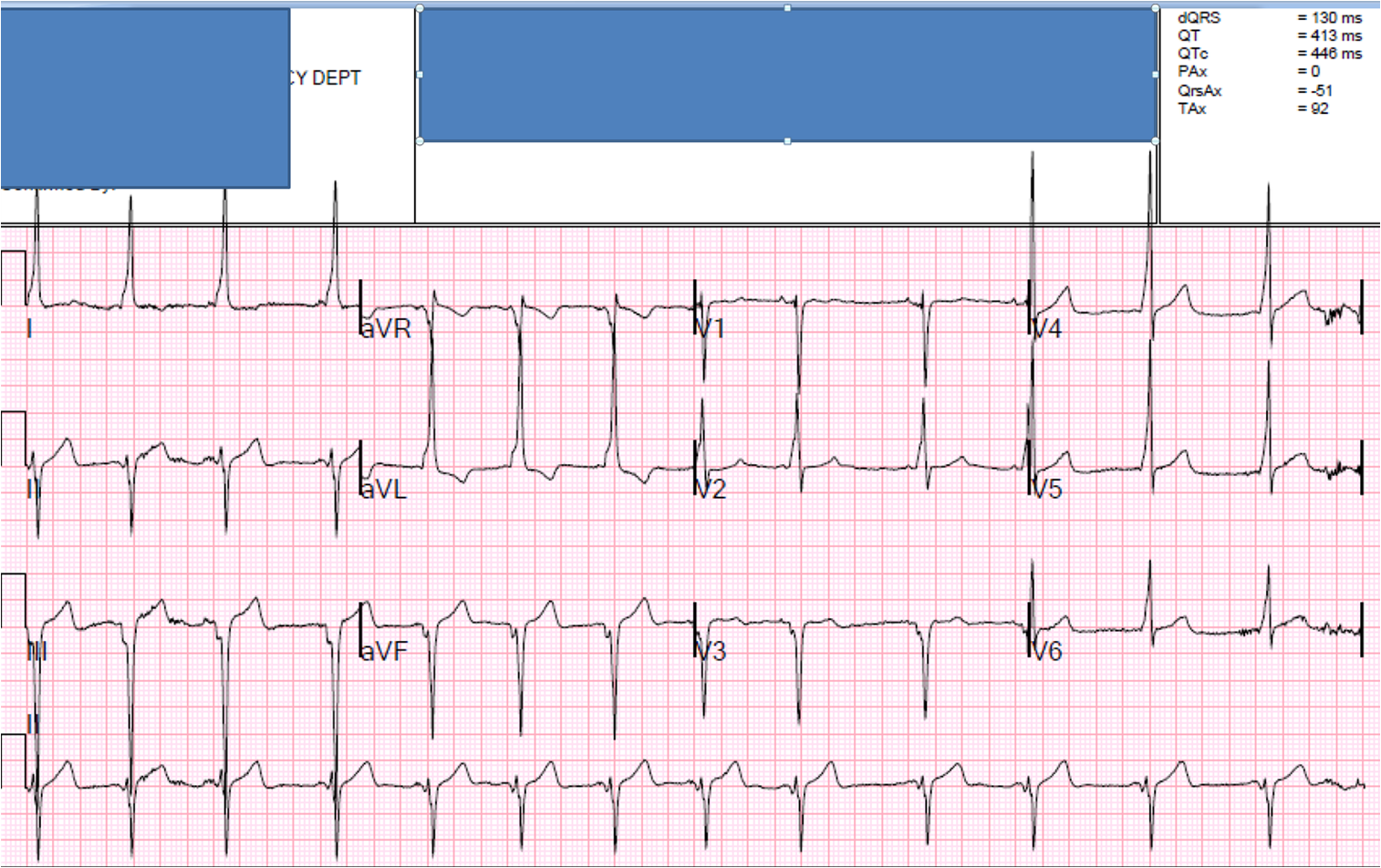
7. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Increased left ventricular muscle mass (from hypertension, aortic stenosis, HCM) generates larger electrical forces, increasing QRS voltage.
ECG Changes:
- High voltage: S wave in V1 + R wave in V5 or V6 ≥35 mm (Sokolow-Lyon criteria)
- OR: R wave in aVL ≥11 mm (Cornell criteria)
- "Strain" pattern: ST depression + T-wave inversion in lateral leads (I, aVL, V5-V6) - indicates pressure overload
- Left axis deviation common
- Broad, notched P wave (P mitrale) if left atrial enlargement coexists
- Prolonged QRS intrinsicoid deflection in V5-V6
Note: LVH also causes ST elevation in V1-V3 (leads with deep S waves) - a STEMI mimic, especially at LITFL described as a "strain" pattern.
8. Ventricular Tachycardia (VT)
Pathophysiology: Rapid, life-threatening arrhythmia originating below the Bundle of His. Most commonly from re-entry in scarred myocardium (post-MI) or structural heart disease.
ECG Changes:
- Wide QRS tachycardia (QRS ≥120 ms), rate 100-250 bpm
- Regular rhythm (usually)
- AV dissociation - P waves independent of QRS (best differentiator from SVT with aberrancy)
- Capture beats - occasional narrow QRS when sinus P wave captures ventricle
- Fusion beats - hybrid QRS when sinus and VT beat fuse
- Positive or negative precordial concordance - all V1-V6 QRS in same direction
- QRS axis often extreme (northwest axis, -90° to ±180°)
VT vs. SVT with aberrancy - key Brugada criteria:
- AV dissociation = VT
- Concordance = VT
- QRS >160 ms = strongly suggests VT
- RBBB-like pattern: taller left rabbit-ear in V1 = VT
9. Brugada Syndrome
Pathophysiology: Genetic channelopathy (usually SCN5A sodium channel mutation) causing abnormal ventricular repolarization, predisposing to VF and sudden cardiac death - especially in young Asian males at night/at rest.
ECG Changes (diagnostic "Brugada sign"):
- Type 1 (diagnostic): Coved ST elevation ≥2 mm in V1-V2 with descending ST segment and inverted T wave ("shark fin" or "coved" pattern) - diagnostic only if spontaneous
- Type 2: Saddle-back ST elevation in V1-V2 (≥0.5 mm) - not diagnostic alone
- Partial RBBB pattern
- Normal QRS in peripheral leads
- Can be unmasked by fever, sodium channel blockers (flecainide, ajmaline challenge)
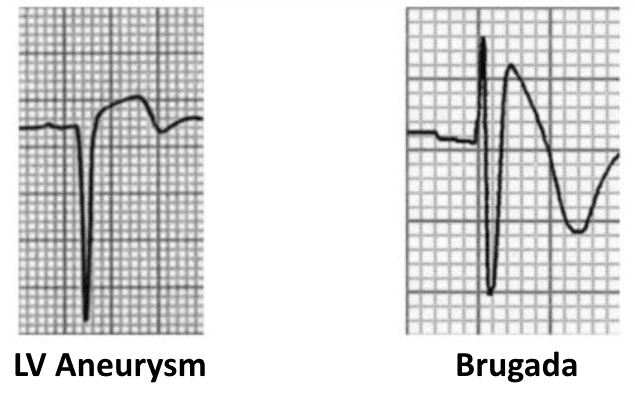
Left: LV aneurysm pattern (persistent ST elevation post-MI). Right: Brugada pattern - coved ST elevation in V1 with the characteristic "shark fin" morphology and partial RBBB.
10. Long QT Syndrome (LQTS)
Pathophysiology: Abnormal ventricular repolarization (genetic mutations in K+, Na+, or Ca2+ channels; or drug-induced) prolongs the QT interval, creating a window for early afterdepolarizations that can trigger Torsades de Pointes (polymorphic VT).
ECG Changes:
- Prolonged corrected QT interval (QTc):
- Males: QTc >440 ms (symptomatic concern); >500 ms = high risk
- Females: QTc >450 ms; >500 ms = high risk
- T-wave morphology abnormalities:
- LQTS1: Broad-based T wave
- LQTS2: Low-amplitude notched/bifid T wave
- LQTS3: Long isoelectric ST segment with late-peaking narrow T wave
- Torsades de Pointes on ECG: polymorphic VT with QRS complexes that twist around the baseline, rate 200-250 bpm
- Bradycardia or QT prolongation often visible post-exercise (LQTS1) or during sleep (LQTS3)
Formula - Bazett's correction: QTc = QT ÷ √(RR interval in seconds)
Summary Table
| # | Disease | Key ECG Finding | Leads Affected |
|---|---|---|---|
| 1 | STEMI | ST elevation (convex), Q waves | Regional (depends on artery) |
| 2 | NSTEMI/ACS | ST depression, T inversions, Wellens | Anterior/lateral |
| 3 | Atrial Fibrillation | Absent P waves, irregularly irregular RR | All leads |
| 4 | LBBB | Wide QRS, M-shaped R (lateral), rS in V1 | V1, I, aVL, V5-V6 |
| 5 | Complete Heart Block | AV dissociation, slow escape rhythm | All leads |
| 6 | Acute Pericarditis | Diffuse concave ST elevation + PR depression | I, II, III, aVF, V2-V6 |
| 7 | LVH | High voltage, lateral strain pattern | V1-V6, I, aVL |
| 8 | Ventricular Tachycardia | Wide complex tachycardia, AV dissociation | All leads |
| 9 | Brugada Syndrome | Coved ST elevation + partial RBBB | V1-V2 |
| 10 | Long QT Syndrome | QTc >450-500 ms, T-wave morphology changes | All leads |
Sources:
- Harrison's Principles of Internal Medicine 22E, p. 1915-1916 - Myocardial Ischemia and Infarction ECG
- Tintinalli's Emergency Medicine, Chapter 18 - ECG Features of Atrial Fibrillation
- Ganong's Review of Medical Physiology 26E, p. 534 - Myocardial Infarction ECG changes
- Goldman-Cecil Medicine, Electrocardiography - Bundle branch blocks, LVH, channelopathies
- LITFL ECG Library - Pericarditis, Brugada, LBBB, AF
This is a shared conversation. Sign in to Orris to start your own chat.