Discuss the role of colonic mucosal biopsy in the evaluation of patients with suspected inflammatory diseases
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching PubMed
colonic mucosal biopsy inflammatory bowel disease diagnosis
Loading Image
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compose the full detailed answer.
Colonic Mucosal Biopsy in the Evaluation of Suspected Inflammatory Diseases
1. Overview and Clinical Importance
The colonic mucosal biopsy occupies a central role in the workup of patients with suspected colonic inflammatory diseases. As stated in Goldman-Cecil Medicine: "The diagnosis of inflammatory bowel disease is contingent upon accurate histopathologic results, so biopsy of the affected area(s) is key." Biopsy findings allow the clinician to:
- Confirm the presence of mucosal inflammation
- Distinguish between the major forms of IBD (ulcerative colitis vs. Crohn's colitis)
- Exclude infectious, ischemic, drug-induced, and microscopic colitides
- Detect dysplasia and malignant transformation during surveillance
- Assess disease activity and response to therapy
2. Normal Colonic Histology as a Baseline
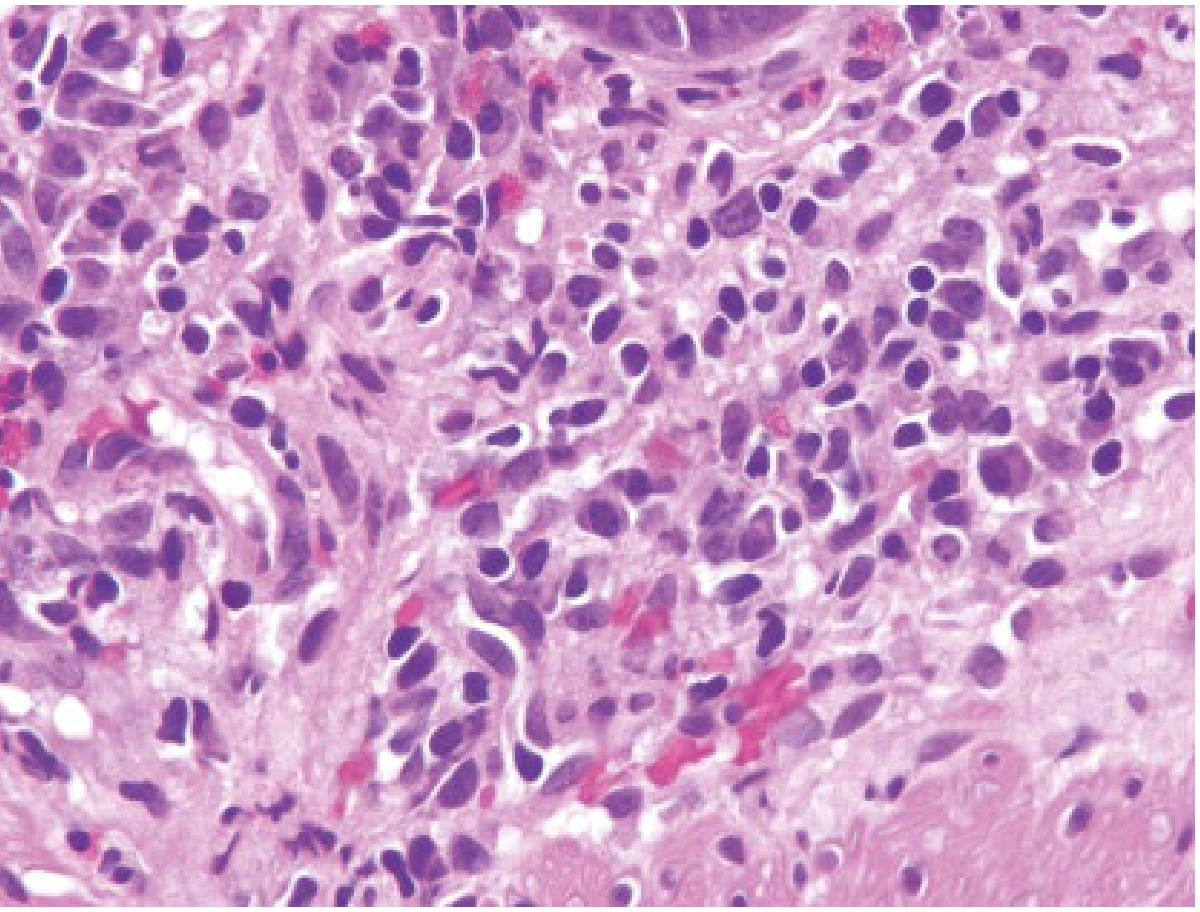
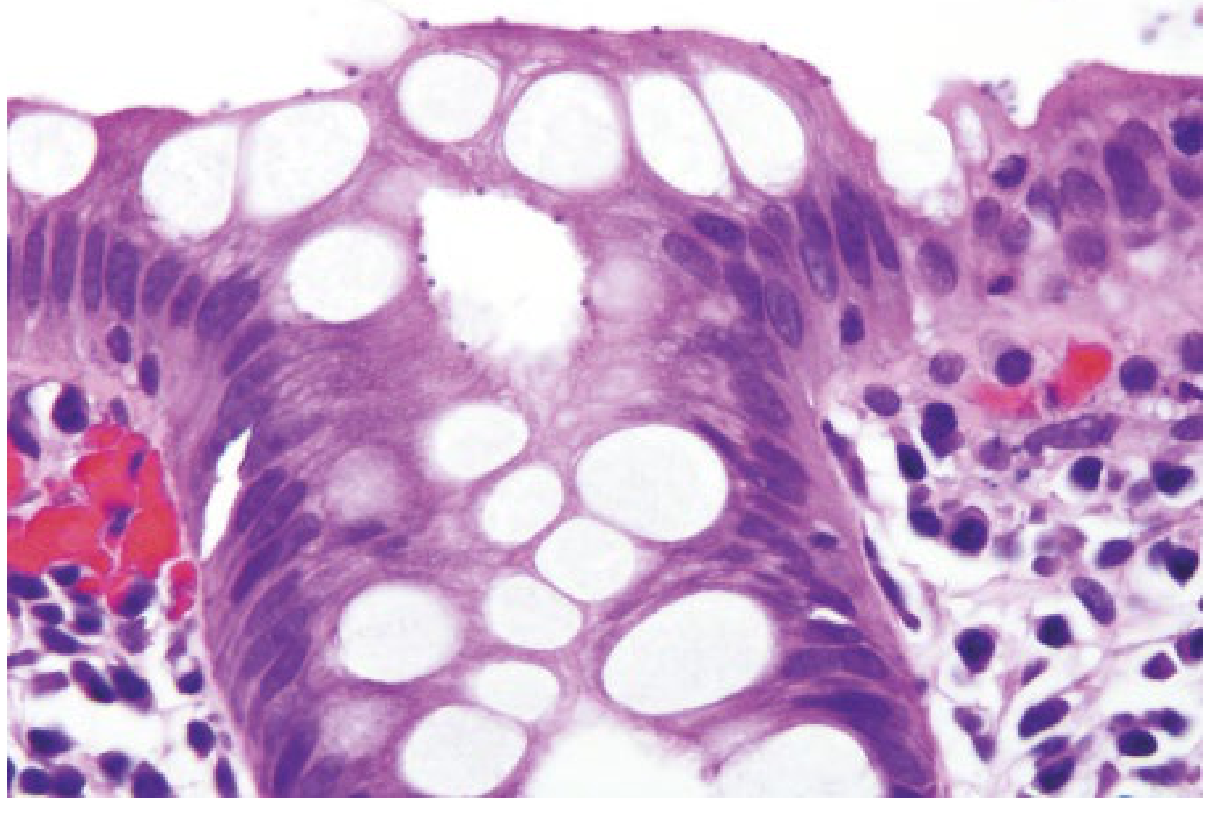
Interpreting biopsy pathology requires familiarity with regional variations in normal colonic mucosa. In the right colon, the lamina propria is normally more cellular, with abundant plasma cells throughout the full mucosal thickness, lymphocytes, eosinophils, and occasional Paneth cells. In the left colon and rectum, goblet cells predominate and the lamina propria is less cellular - plasma cells are found only beneath the surface epithelium. Lymphoid aggregates and intraepithelial lymphocytes (IELs) are normal, especially overlying lymphoid follicles. Eosinophils are present in most right colonic biopsies, with numbers varying by geographic region.
These regional differences are important because findings normal in the right colon (e.g., basal plasma cells) may be abnormal in the rectum, and vice versa.
- Yamada's Textbook of Gastroenterology, 7th ed.
3. Ulcerative Colitis (UC)
Macroscopic/Endoscopic-Histologic Correlation
UC begins in the rectum and extends proximally in a continuous, uninterrupted pattern, never leaving skip areas. Early endoscopic changes are erythema, loss of the vascular pattern, and granularity. As disease worsens, the mucosa becomes friable and ulcerated.
Histological Features of Active UC
The key findings on colonic biopsy in UC include:
| Feature | Description |
|---|---|
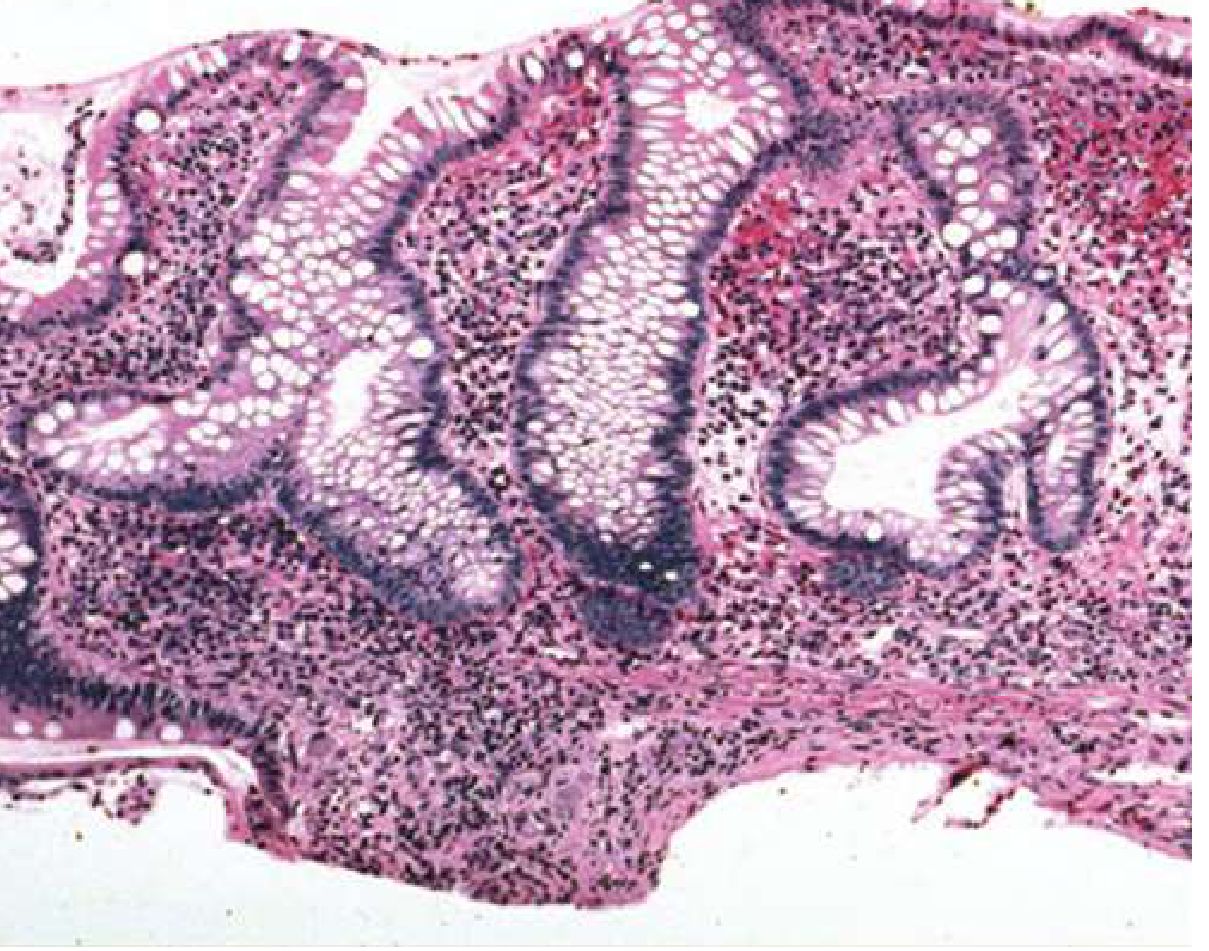
| Crypt architectural distortion | Decreased crypt numbers, branched/malformed regenerated crypts; reflects prior mucosal destruction and imperfect repair |
| Basal plasmacytosis | Plasma cells accumulate between the crypt bases and the muscularis mucosae - a hallmark of chronic mucosal injury |
| Cryptitis | Neutrophilic infiltration within crypt epithelium |
| Crypt abscesses | Neutrophil collections within crypt lumina (nonspecific but characteristic) |
| Mucin depletion | Regenerating epithelium lacks mature goblet cell mucin |
| Diffuse, continuous involvement | All biopsy fragments from the same topographic area show similar findings; inflammation is typically more severe distally |
| No granulomas | Granulomas are absent (occasional foreign-body reaction to ruptured crypt content may be seen, but lacks classic epithelioid morphology) |
Pyloric gland metaplasia is not typical in UC. Lymphoid aggregates at the mucosal-submucosal interface are commonly found.
- Yamada's Textbook of Gastroenterology, 7th ed.
- Goldman-Cecil Medicine, International Ed.
4. Crohn's Colitis
Distinguishing Features on Biopsy
Crohn's disease produces distinctly different biopsy findings compared with UC:
| Feature | Crohn's Colitis | Ulcerative Colitis |
|---|---|---|
| Pattern of involvement | Focal/patchy; skip areas | Diffuse, continuous |
| Crypt destruction | Patchy - involved and uninvolved crypts adjacent to each other | Diffuse |
| Granulomas | Infrequent but pathognomonic when present; usually poorly formed, associated with chronic inflammation | Absent |
| Aphthous erosions | Characteristic early lesions - focal surface necrosis with mixed chronic inflammatory infiltrate | Not typical |
| Submucosal inflammation | Significant submucosal chronic inflammation may be seen even with minimal mucosal change | Absent (inflammation confined to mucosa) |
| Transmural lymphoid aggregates | Present in resection specimens | Absent |
| Pyloric gland metaplasia | Common - indicates repeated inflammation and repair | Occasional |
| Fissures | May be apparent | Absent |
The critical caveat regarding granulomas: approximately 65% of patients with Crohn's disease will not exhibit granulomas on histology, and therefore their absence does not exclude Crohn's disease. Granulomas found in large numbers should raise suspicion for infectious etiologies (e.g., yersiniosis, histoplasmosis, tuberculosis) rather than Crohn's. Features favoring infection over Crohn's include granulomas centered in lymphoid follicles and granulomas with central necrosis.
- Fischer's Mastery of Surgery, 8th ed.
- Yamada's Textbook of Gastroenterology, 7th ed.
5. Differential Diagnosis on Biopsy
A major task of the colonic mucosal biopsy is to distinguish IBD from the following conditions:
5a. Infectious Colitis
- Characterized by a predominance of neutrophils in the lamina propria rather than within the crypt epithelium
- Architectural preservation is supportive of infectious over ulcerative colitis
- Overall chronic inflammation (lymphocytes/plasma cells) is less prominent
- The initial episode of UC may histologically mimic infectious colitis; therefore, infectious etiologies must be excluded before confirming UC
5b. NSAID/Medication-Induced Colitis
- NSAID ulcers are typically abrupt with no significant inflammation in adjacent mucosa and minimal chronic inflammation
- Erosions of NSAID origin have negligible acute inflammation; typically only a few neutrophils
- NSAID strictures ("diaphragms") are circumferential; biopsies show fibrosis with minimal inflammation
- Medications (NSAIDs, statins, PPIs, SSRIs) may cause focal acute colitis or ulcers throughout the colon
5c. Ischemic Colitis
The classical biopsy features of ischemic colitis include:
- Marked surface epithelial injury with mucin loss
- "Atrophic microcrypts" and crypt dropout
- Hyalinization of the lamina propria - the normal loose connective tissue is replaced by dense eosinophilic matrix ("lamina propria collapse")
- Residual glands become more closely spaced
- Lack of neutrophil-mediated crypt destruction (contrasts with UC)
- Chronic ischemic colitis can be mistaken for UC, but age, location, muscularis propria involvement, and absence of cryptitis help differentiate
5d. Microscopic Colitis (Collagenous and Lymphocytic)
Microscopic colitis describes patients with:
- Chronic watery diarrhea
- Normal colonoscopy and barium enema
- Specific microscopic features on biopsy despite a macroscopically normal colon
The term was first coined by Read et al. (1980). There are two main subtypes:
Collagenous colitis:
- Thickened subepithelial collagen band (>10 µm)
- Inflamed lamina propria and surface injury
- Predominantly affects middle-aged women (F:M = 6-8:1, median age 55 years)
- Associated with rheumatoid arthritis, thyroid disorders, celiac disease, diabetes mellitus, and NSAID use
Lymphocytic colitis:
- Increased intraepithelial lymphocytes (≥20 per 100 epithelial cells)
- Inflamed lamina propria similar to collagenous colitis
- Separated as a distinct entity by Lazenby et al. (1989)
- Similar clinical associations
Both types require biopsy for diagnosis, as the endoscope cannot identify either condition.
- Yamada's Textbook of Gastroenterology, 7th ed.
5e. Focal Active Colitis (FAC)
FAC (focal neutrophilic infiltration with or without multiple foci) is a recognized biopsy pattern that may represent:
- A precursor or early manifestation of Crohn's disease (particularly in pediatric patients - up to 27.6% went on to develop Crohn's in some series)
- Infectious diarrhea (most common in adults)
- Bowel preparation artifact
In adult patients without clinical or endoscopic features of Crohn's disease, FAC can be managed conservatively, whereas it warrants close follow-up in children.
6. Dysplasia Surveillance in Long-standing IBD
Colonic biopsy plays a specific and ongoing surveillance role in patients with long-standing UC or Crohn's colitis because of their markedly elevated risk of colorectal carcinoma (CRC).
- CRC risk in UC begins after 7 years of disease and rises approximately 10% per decade, reaching as high as 34% at 30 years in some series (more recent population data suggest 15-18% at 30 years)
- Risk correlates with duration and extent of disease - universal colitis carries the highest risk
- Crohn's ileocolitis carries a 4-20-fold increased risk over the general population
Dysplasia is the recognized precursor lesion to carcinoma in IBD, as carcinomas do not arise de novo from normal mucosa. Dysplastic changes include:
- Crypts reduced in number, irregularly branched, and crowded ("back-to-back" glands)
- Enlarged, hyperchromatic nuclei
- Increased mitoses
- Pseudostratification (nuclei at different levels, "picket-fence" appearance)
- Classified as low-grade or high-grade
Systematic mapping biopsies with random sampling throughout the colon, supplemented by targeted biopsies of visible lesions, are the standard surveillance approach.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
7. Effects of Treatment on Biopsy Interpretation
Treatment significantly alters histological appearance and can cause diagnostic difficulty:
- Treated UC may show areas of involved and uninvolved mucosa, mimicking the patchy pattern of Crohn's colitis
- Iatrogenic rectal sparing can occur in treated UC, removing the characteristic distal predilection
- Fulminant colitis (toxic UC or fulminant Crohn's): impossible to distinguish on mucosal biopsy alone, because many discriminating features (transmural lymphoid aggregates, granulomas) are deep to the mucosa
- Re-review of original pre-treatment material is essential before a definitive diagnosis of UC vs. Crohn's is made - this is especially important before ileal pouch-anal anastomosis (IPAA), since Crohn's disease is a relative contraindication
8. Biopsy Artifacts to Recognize
Colonic mucosal biopsies are subject to several interpretive pitfalls:
- Hypertonic enemas (pre-sigmoidoscopy) may cause flattened surface epithelium, mucin loss, or mild neutrophilic inflammation
- Sodium phosphate bowel prep creates aphthous-like endoscopic lesions that histologically may resemble early Crohn's disease
- Gas insufflation can produce submucosal "pseudolipomatosis" (clear bubble-like spaces)
- Biopsy forceps trauma causes mucosal hemorrhage, crush artifact that may mimic dysplasia, or empty crypts ("squeeze artifact") that may be mistaken for ischemia
9. Summary Table: Key Histological Differences
| Feature | UC | Crohn's | Infectious | Ischemic | Microscopic Colitis |
|---|---|---|---|---|---|
| Pattern | Diffuse, continuous | Focal/patchy | Variable | Left-sided watershed | Normal endoscopy |
| Crypt distortion | Prominent, diffuse | Focal | Preserved | Crypt dropout | Minimal |
| Neutrophils | Cryptitis/abscesses | Cryptitis (focal) | Lamina propria | Absent/mild | Absent |
| Basal plasmacytosis | Yes | May be patchy | No | No | No |
| Granulomas | No | Rare (35%) | Many (if TB/fungal) | No | No |
| Submucosal change | Absent | Significant | Absent | Hyalinization | Subepithelial collagen (CC) |
| Goblet cell depletion | Yes | Variable | Absent | Yes | No |
Recent Evidence
A 2025 systematic review and meta-analysis (PMID 39300818) found that histological parameters including mucosal basal plasmacytosis and eosinophilia are useful in distinguishing IBD-type colitis from non-IBD colitis, supporting the clinical utility of these biopsy findings described in the textbook literature.
Key Takeaway: The colonic mucosal biopsy is indispensable in the evaluation of suspected colonic inflammatory disease. Its roles extend from initial diagnosis and classification (UC vs. Crohn's vs. other colitides) through differential diagnosis (infection, ischemia, medication, microscopic colitis) to long-term surveillance for dysplasia. Interpretation requires integration of the histological findings with the clinical context, endoscopic appearance, distribution of disease, and history of treatment.
Sources: Goldman-Cecil Medicine (International Ed.); Yamada's Textbook of Gastroenterology (7th ed.); Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Fischer's Mastery of Surgery (8th ed.)
Discuss colorectal tumour short answers questions
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here is a comprehensive set of short-answer discussions on colorectal tumours, organized as individual exam-style topics:
Colorectal Tumours - Short Answer Questions
Q1. What are the risk factors for colorectal cancer (CRC)?
Risk factors for CRC can be divided into dietary/lifestyle and hereditary/clinical categories:
Dietary & Lifestyle:
- High animal fat and calorie intake ("Western diet") - associated with increased gut anaerobes (e.g., Fusobacterium nucleatum, Bacteroides fragilis) that convert bile acids into carcinogens
- Obesity and insulin resistance - elevated circulating IGF-I stimulates intestinal mucosal proliferation
- Physical inactivity
- Tobacco use (particularly after >35 years)
- Moderate to excessive alcohol consumption
- Vitamin D deficiency
Clinical & Hereditary:
- Inflammatory bowel disease (UC and Crohn's disease) - risk increases ~0.5-1% per year after the first 10 years; 8-30% of patients develop cancer
- Prior adenoma or carcinoma (3-5% lifetime risk of a second colorectal cancer)
- Family history of colorectal cancer
- Hereditary polyposis syndromes (FAP, MAP, Lynch syndrome)
- Streptococcus bovis bacteremia (associated with underlying colonic neoplasia)
- Age (risk increases significantly after 50 years, but screening is now recommended from age 45)
Sources: Harrison's Principles of Internal Medicine 22E; Bailey & Love's Short Practice of Surgery 28th Ed.
Q2. Classify colorectal polyps.
Colorectal polyps are classified as:
Neoplastic Polyps
| Type | Features |
|---|---|
| Tubular adenoma | Most common (75-80%); pedunculated; low malignant potential |
| Tubulovillous adenoma | Intermediate features; intermediate risk |
| Villous adenoma | Sessile, carpet-like; highest malignant potential (up to 40% risk); may secrete large volumes of mucus causing electrolyte disturbances |
| Serrated adenoma | Precursor via serrated pathway; includes sessile serrated lesions |
Non-Neoplastic Polyps
| Type | Features |
|---|---|
| Hyperplastic | Small, pale, common in rectosigmoid; no malignant potential |
| Hamartomatous | Peutz-Jeghers (STK11 gene), Juvenile polyposis; rare malignant transformation |
| Inflammatory pseudopolyps | Seen in IBD; residual mucosa between ulcers |
Risk of malignancy in an adenoma increases with:
- Size >2 cm
- Villous histology
- High-grade dysplasia
- Multiple polyps
Q3. Describe Familial Adenomatous Polyposis (FAP).
Definition: An autosomal dominant inherited syndrome caused by germline mutations in the APC gene (chromosome 5q21), characterized by hundreds to thousands of adenomatous polyps throughout the colon.
Epidemiology:
- Incidence: 1 in 10,000 births
- Accounts for <1% of all CRC
- Up to one-third of cases are de novo mutations (no family history)
- Median age of adenoma development: 17 years
- Untreated patients develop CRC at median age 40; death at mean age 44
Genetics/Molecular Pathways:
The APC protein normally forms a complex that allows degradation of beta-catenin. When APC is non-functional, beta-catenin accumulates, enters the nucleus, and induces transcription of growth factors - driving cell proliferation, adhesion, and migration. A germline mutation in one APC allele followed by a somatic "second hit" leads to the adenoma-to-carcinoma sequence.
- Mutations in the "mutation cluster region" of exon 15 produce a virulent phenotype (thousands of polyps, earlier CRC onset)
- Mutations at the 3' end produce a milder (attenuated) phenotype
Extracolonic Manifestations (variants):
| Syndrome | Additional Features |
|---|---|
| Gardner's syndrome | Osteomas, fibromas, lipomas, epidermoid cysts, desmoid tumors, ampullary cancers, congenital hypertrophy of retinal pigment epithelium (CHRPE) |
| Turcot's syndrome | CNS tumors (medulloblastoma) |
| Attenuated FAP | Fewer polyps (<100), later onset |
Management:
- Prophylactic colectomy is indicated (total colectomy with ileal pouch anal anastomosis, or subtotal colectomy with ileorectal anastomosis)
- Patients should be followed for extracolonic tumors
- NSAIDs (sulindac, celecoxib) cause polyp regression but do not reliably prevent CRC
Source: Mulholland & Greenfield's Surgery 7e; Harrison's Principles of Internal Medicine 22E
Q4. What is Lynch Syndrome (HNPCC)? How is it diagnosed?
Definition: Lynch syndrome (formerly hereditary nonpolyposis colorectal cancer - HNPCC) is the most common inherited predisposition to CRC, accounting for ~3% of all colorectal cancers. It confers up to a 17-fold increased risk of CRC.
Genetics:
- Caused by germline mutation in one of the DNA mismatch repair (MMR) genes:
- MLH1 (chromosome 3p22)
- MSH2 (chromosome 2p21-16)
- MSH6 (chromosome 2p16)
- PMS2 (chromosome 7p22)
- Also caused by EPCAM gene deletion (causes loss of MSH2 expression)
- Inherited in autosomal dominant fashion
- MMR system failure results in microsatellite instability (MSI) - accumulation of ~1000-fold more mutations compared with MMR-proficient tumors
Extracolonic Cancers: Endometrium (most frequent), ovary, stomach, small bowel, pancreaticobiliary, genitourinary, brain, and skin
Diagnosis:
- Universal tumor testing: All CRC specimens should be tested by immunohistochemistry (IHC) for MMR proteins OR by microsatellite instability PCR
- Amsterdam Criteria / Revised Bethesda Criteria: Family history criteria used for patients without a cancer diagnosis
- Germline testing: Recommended for all patients with deficient MMR on tumor sample or appropriate family history (with pre- and post-test genetic counseling)
Clinical Note: Lynch syndrome may not produce multiple polyps, making it easily missed clinically.
Source: Harrison's Principles of Internal Medicine 22E
Q5. Describe the pathology of colorectal adenocarcinoma.
Gross Pathology:
- Right-sided tumors: often polypoid/exophytic, may grow large before becoming symptomatic (present with iron-deficiency anemia, occult bleeding)
- Left-sided tumors: often annular/constricting ("apple-core" lesion on barium enema), cause obstruction and change in bowel habit
- Sigmoid/rectal tumors: commonly cause rectal bleeding, tenesmus, pencil-thin stools
Histopathology:
- Over 90% are adenocarcinomas (mucin-secreting)
- Arise via the adenoma-to-carcinoma sequence (APC mutation → K-ras activation → loss of DCC/SMAD4 → TP53 mutation → invasive carcinoma) or via the serrated pathway (BRAF mutation → MLH1 silencing → MSI-H)
- Poorly differentiated histology, venous invasion, and perineural invasion worsen prognosis
Sites (in order of frequency):
Rectum > Sigmoid colon > Descending colon > Cecum/Ascending colon > Transverse colon
Spread:
- Direct: Longitudinally along the bowel wall and radially into pericolic fat, adjacent organs
- Lymphatic: Along lymphatics to regional nodes in orderly progression from paracolic to intermediate to central nodes
- Hematogenous: Most commonly to liver via portal vein (1/3 of patients have liver metastases at diagnosis; 50% develop them at some point)
- Transcoelomic/Peritoneal: Peritoneum, ovaries (Krukenberg tumour), omentum
- Lung is the next most common metastatic site after liver; brain, bone, kidney are less common
Q6. How is colorectal cancer staged?
Dukes' Classification (historical but widely known):
| Stage | Definition | 5-Year Survival |
|---|---|---|
| A | Invasion of but not breaching the muscularis propria | ~95% |
| B | Breaching the muscularis propria; no lymph node involvement | ~75% |
| C | Lymph nodes involved | ~40-50% |
| D | Distant metastases (Dukes himself never described this; added later) | ~5% |
TNM Classification (AJCC - International Standard):
| Stage | TNM | Description |
|---|---|---|
| Stage I | T1-2 N0 M0 | Tumor within submucosa (T1) or muscularis (T2); no nodes |
| Stage II | T3-4 N0 M0 | Penetrates through muscularis into pericolic fat (T3) or adjacent organs (T4) |
| Stage III | Any T, N1-2, M0 | Regional lymph node involvement |
| Stage IV | Any T, Any N, M1 | Distant metastases (liver, lung, peritoneum, bone) |
Prognostic factors beyond stage:
- Tumor penetration through bowel wall into pericolic fat
- Poorly differentiated histology
- Perforation and/or tumor adherence to adjacent organs
- Venous invasion
- <12 lymph nodes sampled (unreliable staging)
- MSI-High / deficient MMR tumors have an improved prognosis (enhanced anti-tumor immune response)
- Right-sided colon cancer has a worse prognosis than left-sided (molecular differences)
- Tumor size itself does not independently affect prognosis when adjusted for nodal status and differentiation
Sources: Bailey & Love's 28th Ed.; Maingot's Abdominal Operations; Harrison's Principles of Internal Medicine 22E
Q7. What is the role of CEA in colorectal cancer?
Carcinoembryonic antigen (CEA) is the most important serum tumor marker for CRC.
Uses:
- Baseline preoperative level: Elevated levels at presentation are associated with worse prognosis
- Monitoring for recurrence: CEA measured at 3-month intervals for 5 years after curative resection. A rising CEA may detect occult recurrence before it becomes clinically apparent
- Assessing response to chemotherapy/targeted therapy
- Not suitable for screening in asymptomatic populations (low sensitivity and specificity; elevated CEA can occur in benign conditions such as liver disease, smoking, and pancreatitis)
Q8. How is screening for colorectal cancer performed?
Screening aims to detect polyps before malignant transformation and identify early-stage cancers in asymptomatic individuals.
Population screening (average risk - from age 45 per USPSTF 2021 update):
| Method | Notes |
|---|---|
| Fecal occult blood test (FOBT/gFOBT) | Annual; ~50% of CRCs have a negative test; 2-4% of asymptomatic persons test positive; reduces CRC mortality in RCTs |
| Fecal immunochemical test (FIT) | More sensitive than gFOBT for colorectal cancer; annual |
| Multi-target stool DNA test (Cologuard) | Tests for DNA mutations + hemoglobin; more sensitive but less specific than FIT |
| Flexible sigmoidoscopy | Every 5 years; no sedation; misses proximal lesions (~1.5% with normal sigmoidoscopy have proximal advanced neoplasm); evidence for reduction in both incidence and mortality persists >15 years |
| Colonoscopy | Every 10 years; gold standard; assesses entire colon; requires bowel prep and sedation; allows polypectomy |
| CT colonography (virtual colonoscopy) | Every 5 years; non-invasive; any lesion found requires colonoscopy for confirmation/biopsy |
| Double-contrast barium enema | Less commonly used now |
High-risk surveillance:
- FAP: Annual flexible sigmoidoscopy from age 10-12; colectomy when polyps confirmed
- Lynch syndrome: Colonoscopy every 1-2 years from age 20-25 (or 10 years before youngest case in family)
- IBD with pancolitis >8 years: Annual colonoscopy with mapping biopsies
Q9. Describe the surgical management of colon cancer.
Principles:
- Surgical resection is the standard of care for localized (non-metastatic) disease
- Aims: Wide resection with adequate margins, high ligation of feeding vessels, and removal of the draining lymph nodes
- A minimum of 12 lymph nodes must be harvested for adequate staging
- Laparoscopic/robotic approaches have largely replaced open surgery with equivalent oncologic outcomes
Operations by site:
| Site | Operation |
|---|---|
| Cecum, ascending colon | Right hemicolectomy (ligation of ileocolic and right colic vessels) |
| Hepatic flexure, proximal transverse colon | Extended right hemicolectomy (ligation of ileocolic, right colic, and middle colic vessels) |
| Splenic flexure | Segmental resection or extended right hemicolectomy |
| Descending colon | Left hemicolectomy (high ligation of IMA) |
| Sigmoid colon | Sigmoid colectomy |
Adjuvant chemotherapy:
- Stage I: Surgery alone; considered cured
- High-risk Stage II and Stage III: Adjuvant chemotherapy with fluoropyrimidine ± oxaliplatin for 3-6 months
- MSI-high rectal cancers: Checkpoint inhibitors (PD-1 antibodies) may achieve cure without surgery, radiation, or chemotherapy
Follow-up after curative resection:
- Physical exam + CEA every 3 months for 5 years
- Colonoscopy at 1 year, then every 3 years
- CT chest/abdomen/pelvis semi-annually to annually for 3 years
Q10. Describe the management of rectal cancer.
Rectal cancer (defined as tumor at or below the peritoneal reflection) has unique features because of:
- Higher risk of local recurrence compared with colon cancer
- Proximity to sphincter complex, autonomic nerves, and pelvic structures
Staging:
- TNM classification (same as colon cancer)
- Pelvic MRI is the preferred imaging modality for staging: determines T and N stage, circumferential resection margin (CRM) involvement, and tumor relation to the anterior peritoneal reflection
- CEA, contrast-enhanced CT chest/abdomen/pelvis for distant staging
- Complete colonoscopy to exclude synchronous lesions (~3% synchronous CRC, ~30% synchronous polyps)
- Multidisciplinary tumor board review is a central quality metric
Surgery:
- Low anterior resection (LAR): Sphincter-preserving; anastomosis above the dentate line; permanent colostomy avoided
- Abdominoperineal resection (APR): For tumors requiring resection of the anal sphincter; requires permanent colostomy; higher local recurrence risk
- Total Mesorectal Excision (TME): The cornerstone of modern rectal cancer surgery. Sharp dissection within the correct embryological TME plane preserves the fascia propria of the rectum and removes the entire mesorectal fat envelope with its lymph nodes. TME has dramatically reduced local recurrence rates and improved survival. For upper rectal tumors, a partial (tumor-specific) mesorectal excision with 5 cm distal mesorectal margin is acceptable.
Nerve preservation during TME:
- Hypogastric plexus (L1-L3): At risk during high ligation of IMA and posterior dissection; injury causes retrograde ejaculation
- Pelvic plexus/nervi erigentes (S2-S4): At risk during lateral dissection; injury causes erectile dysfunction and atonic bladder
- Periprostatic plexus: At risk during anterior dissection in men
Neoadjuvant Therapy:
- Stages II and III rectal cancer: Preoperative chemoradiation reduces local recurrence
- Combination long-course chemoradiotherapy (5-FU-based) followed by surgery at 6-8 weeks
- Short-course radiotherapy (5 x 5 Gy) is an alternative
- Total neoadjuvant therapy (TNT): Giving full systemic chemotherapy + radiation before surgery; achieves higher rates of complete pathological response
- Organ preservation ("watch-and-wait"): In patients achieving clinical complete response after chemoradiotherapy, surgery may be deferred. Risk of regrowth requires intensive surveillance.
- MSI-high rectal cancers: PD-1 inhibitor (dostarlimab/pembrolizumab) alone may achieve complete response without surgery
Sources: Sabiston Textbook of Surgery; Fischer's Mastery of Surgery 8th Ed.; Harrison's Principles of Internal Medicine 22E
Q11. What are the clinical features of colorectal cancer?
Right-sided (cecum/ascending colon):
- Usually asymptomatic for a long time
- Iron-deficiency anemia (chronic occult blood loss)
- Fatigue, weight loss
- Palpable right iliac fossa mass
- May present with right lower quadrant pain
Left-sided (descending/sigmoid colon):
- Change in bowel habit (alternating constipation and diarrhea)
- Rectal bleeding (fresh or altered blood mixed with stool)
- Abdominal colic
- Features of obstruction (abdominal distension, absolute constipation)
- Pencil-thin stools
Rectal:
- Fresh rectal bleeding
- Tenesmus (feeling of incomplete evacuation)
- Mucous discharge
- Sensation of rectal fullness
Advanced/systemic features:
- Hepatomegaly (liver metastases)
- Jaundice (biliary obstruction from metastases)
- Ascites (peritoneal spread)
- Cachexia, anorexia, weight loss
Q12. What is the adenoma-to-carcinoma sequence?
The progression from normal mucosa → adenomatous polyp → invasive carcinoma involves an ordered accumulation of somatic mutations over ~10 years:
- APC mutation (chromosome 5q): Loss of APC function → accumulation of beta-catenin → dysregulated crypt cell proliferation → formation of an adenoma
- K-ras mutation (chromosome 12p): Point mutation (codon 12 or 13) → constitutive activation of RAS signaling → promotes cell growth; occurs in the transition from small to large adenoma
- Loss of DCC/SMAD4 (chromosome 18q): Loss of TGF-beta signaling; associated with intermediate-to-late adenoma
- TP53 mutation (chromosome 17p): Loss of the "guardian of the genome"; enables transition from high-grade dysplasia to invasive carcinoma
This "chromosomal instability (CIN) pathway" accounts for ~80-85% of sporadic CRC.
The serrated/microsatellite instability pathway (~15%) involves:
- BRAF V600E mutation
- Widespread CpG island methylation (CIMP)
- MLH1 gene silencing by methylation → MSI-High tumors
- Associated with right-sided location, older women, better prognosis
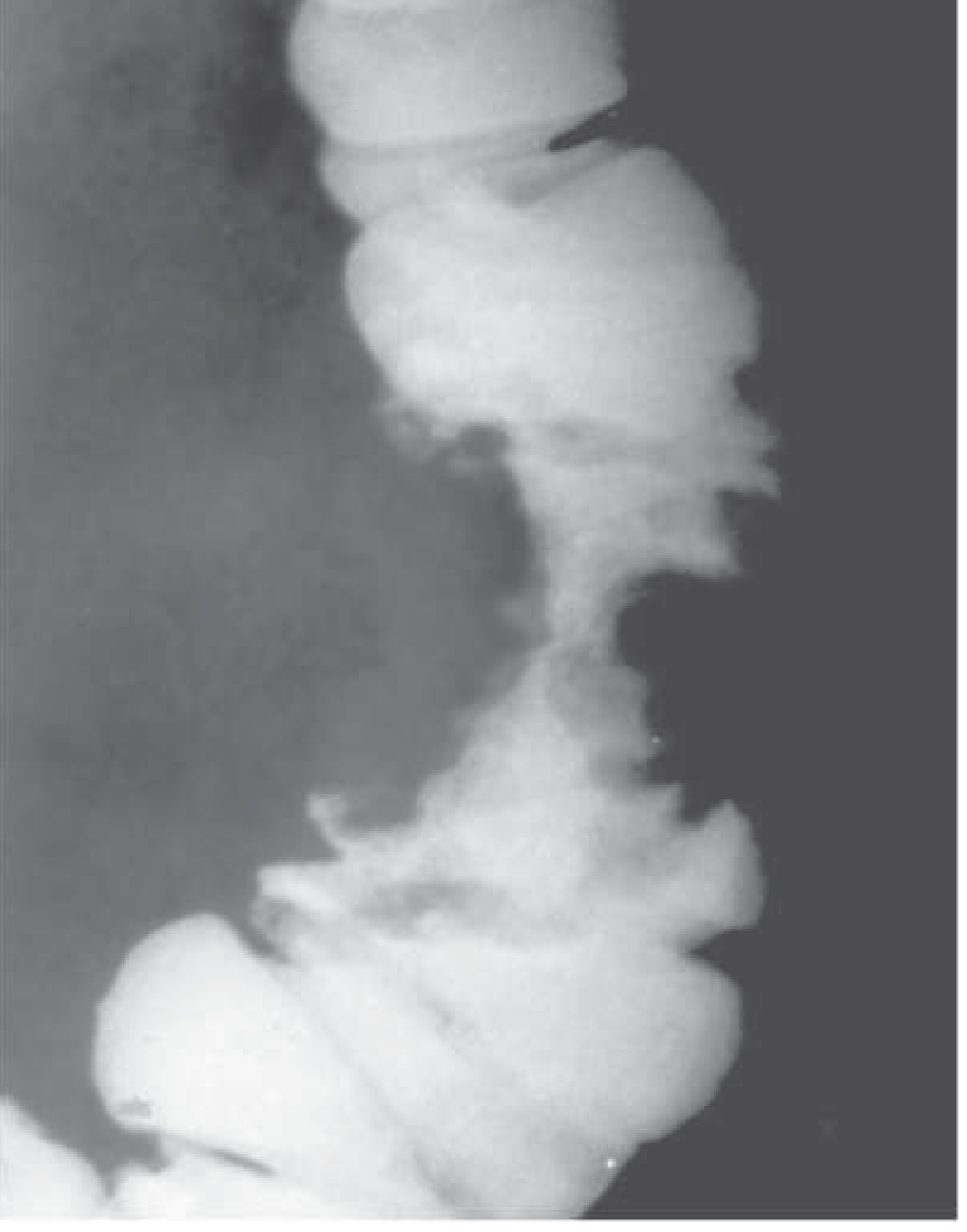
Q13. What is the "apple-core" sign and what does it indicate?
The "apple-core" or "napkin-ring" lesion is a radiological sign seen on double-contrast barium enema or CT colonography. It describes a short, annular, constricting segment of the colon with irregular, overhanging "shelf-like" edges and shouldering at both ends, resembling the core of an apple.
It is always highly suggestive of colorectal carcinoma and reflects the circumferential growth pattern of left-sided colonic adenocarcinoma. The narrowing is due to encircling tumor infiltrating the bowel wall.
Q14. Describe total mesorectal excision (TME).
Definition: TME is the surgical technique of sharp dissection within the embryological avascular plane between the visceral fascia propria of the rectum and the parietal presacral fascia, removing the rectum and its entire mesorectal fat envelope (containing blood vessels, lymphatics, and lymph nodes) as an intact package.
Significance:
- Introduced by Bill Heald in the 1980s
- Reduced local recurrence rates from ~30-40% to <10%
- Ensures adequate circumferential resection margin (CRM)
Principle: The rectum is invested by the mesorectum, which contains the draining lymph nodes most likely to harbor micrometastases. Incomplete excision leaves residual disease and causes local recurrence.
Scope:
- For mid and lower rectal tumors: Full TME down to the level of the levator ani
- For upper rectal tumors: Tumor-specific/partial mesorectal excision with at least 5 cm distal mesorectal clearance
Circumferential Resection Margin (CRM): The radial margin between the deepest point of tumor invasion and the surgical cut surface. A positive CRM (<1 mm clearance) is a strong predictor of local recurrence.
Q15. What are the complications of colorectal cancer surgery?
Intraoperative:
- Hemorrhage
- Ureteric injury
- Nerve injury (autonomic nerves - retrograde ejaculation, erectile dysfunction, atonic bladder)
- Bowel injury
Early postoperative:
- Anastomotic leak (5-15%; more common in low pelvic anastomoses)
- Wound infection
- Ileus
- Deep vein thrombosis / pulmonary embolism
- Urinary retention
Late:
- Anastomotic stricture
- Adhesion-related bowel obstruction
- Incisional hernia
- Anterior resection syndrome (urgency, frequency, fecal incontinence after LAR)
- Tumor recurrence (local recurrence more common in rectal vs. colon cancer)
- Colostomy complications (prolapse, parastomal hernia, retraction)
Key sources: Harrison's Principles of Internal Medicine 22E (2025); Bailey & Love's Short Practice of Surgery 28th Ed.; Sabiston Textbook of Surgery; Fischer's Mastery of Surgery 8th Ed.; Mulholland & Greenfield's Surgery 7e; Maingot's Abdominal Operations
Discuss colorectal tumours
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I now have all the material needed including three key diagrams. Let me now write the comprehensive discussion.
Colorectal Tumours - A Comprehensive Discussion
1. Introduction and Epidemiology
Colorectal cancer (CRC) is one of the most significant malignancies globally. In the UK, it is the second most common cause of cancer death, with approximately 42,000 new diagnoses per year. About one-third arise in the rectum and two-thirds in the colon, with a slight male preponderance (56% vs 44%). The disease occurs more frequently in resource-rich, industrialised countries, with migrants from low-incidence countries gradually assuming the higher incidence rates of their adopted nations - strongly implicating environmental (dietary) factors.
CRC is the broad term encompassing both benign tumours (polyps) and malignant tumours (predominantly adenocarcinoma). Understanding this spectrum is fundamental because most colorectal carcinomas arise from benign precursor lesions.
2. Classification of Colorectal Tumours
Benign
- Adenomatous polyps (neoplastic, with malignant potential):
- Tubular adenoma (most common, ~75%)
- Villous adenoma (highest malignant potential)
- Tubulovillous adenoma (intermediate)
- Serrated/sessile serrated lesions (distinct pathway)
- Non-neoplastic polyps (no direct malignant potential):
- Hyperplastic polyps
- Hamartomatous polyps (Peutz-Jeghers, juvenile polyps)
- Inflammatory pseudopolyps (seen in IBD)
Malignant
- Adenocarcinoma (>90% of CRC)
- Squamous cell carcinoma (anal canal, rare)
- Carcinoid/Neuroendocrine tumour
- Lymphoma (rare)
- Gastrointestinal stromal tumour (GIST)
- Kaposi sarcoma (immunocompromised patients)
3. Aetiology and Risk Factors
Most CRCs develop from adenomatous polyps through a sequence of genetic mutations influenced by environmental factors.
Hereditary Syndromes (summarised below):
| Syndrome | Polyp Distribution | Histology | Malignant Risk | Associated Lesions |
|---|---|---|---|---|
| Familial adenomatous polyposis (FAP) | Large intestine | Adenoma | Very high (100% if untreated) | - |
| Gardner's syndrome | Large and small intestines | Adenoma | Very high | Osteomas, fibromas, lipomas, epidermoid cysts, CHRPE, ampullary cancers, desmoids |
| Turcot's syndrome | Large intestine | Adenoma | Very high | Brain tumours (medulloblastoma) |
| MYH-associated polyposis (MAP) | Large intestine | Adenoma | High | None |
| Lynch syndrome (HNPCC) | Large intestine (often proximal) | Adenoma | High | Endometrial (most frequent), ovarian, gastric, urological, biliary, small bowel, brain, skin |
| Peutz-Jeghers syndrome | Small and large intestines, stomach | Hamartoma | Rare | Mucocutaneous pigmentation; ovarian, breast, pancreatic, endometrial tumours |
| Juvenile polyposis | Large and small intestines, stomach | Hamartoma (rarely progresses to adenoma) | Rare | Various congenital abnormalities |
Source: Harrison's Principles of Internal Medicine 22E (2025)
Dietary and Lifestyle Factors:
- High animal fat and red/processed meat intake - increases gut anaerobes (Fusobacterium nucleatum, Bacteroides fragilis) that convert bile acids into carcinogens
- Haem and N-nitroso compounds in meat products
- Obesity and insulin resistance - elevated IGF-I stimulates mucosal proliferation
- Sedentary lifestyle
- Cigarette smoking (especially after >35 years)
- Moderate-to-excessive alcohol intake
- Cholecystectomy (marginally increases right-sided colon cancer risk)
Clinical Risk Factors:
- Inflammatory bowel disease - risk increases at ~0.5-1% per year after 10 years of disease; 8-30% of patients may develop CRC
- Prior adenoma or colorectal carcinoma (3-5% lifetime risk of second CRC)
- Streptococcus bovis bacteremia (strong association with colonic neoplasia)
- Vitamin D deficiency
Protective Factors:
- Dietary fibre (reduces transit time, reduces carcinogen exposure)
- Aspirin/NSAIDs (inhibit prostaglandin synthesis via COX-2, associated with polyp regression and reduced incidence in cohort studies)
- Calcium and magnesium intake
- Oestrogen replacement therapy (reduces incidence but not mortality in women)
4. Molecular Pathogenesis
4a. The Adenoma-Carcinoma Sequence (Chromosomal Instability Pathway - ~85% of CRC)
The progression from normal mucosa → adenoma → invasive carcinoma takes ~10-15 years and involves an ordered accumulation of somatic mutations:
- APC mutation (chromosome 5q21) - occurs in 2/3 of colonic adenomas; earliest event. Loss of APC function allows beta-catenin to accumulate, enter the nucleus, and drive transcription of growth factors (WNT pathway activation)
- K-ras mutation (codon 12 or 13) - activation of cell signalling pathways; more common in larger lesions, suggesting it is a later event in mutagenesis
- Loss of DCC/SMAD4 (chromosome 18q) - loss of TGF-beta signalling; associated with intermediate adenoma
- TP53 mutation (chromosome 17p) - loss of the "guardian of the genome"; transition from high-grade dysplasia to invasive carcinoma
Evidence supporting the adenoma-carcinoma sequence:
- Distribution of adenomas is similar to that of cancers (70% left-sided)
- Larger adenomas are more likely to be dysplastic
- Majority of early cancers have adjacent adenomatous tissue
- Adenomas are found in one-third of specimens resected for CRC
- CRC incidence decreases within screening programmes that include colonoscopy and polypectomy
4b. Mismatch Repair Deficiency / Microsatellite Instability Pathway (~15%)
DNA mismatch repair (MMR) proteins act as "spell checkers" during DNA replication. When MMR is defective, errors accumulate throughout the genome, including in microsatellites (tandem repeat sequences). In normal cells, microsatellite length remains constant; when MMR is defective, satellites are unstable and change length, creating mutated alleles - a phenotype called microsatellite instability (MSI).
- Lynch syndrome (HNPCC): Germline mutation in one MMR gene (MLH1, MSH2, MSH6, or PMS2) plus somatic "second hit." MSH2 and MLH1 each account for ~30% of cases. Autosomal dominant inheritance. Predisposes to CRC arising in the cecum/proximal colon.
- Sporadic MSI-H CRC: Usually due to epigenetic silencing of MLH1 by promoter methylation (CIMP-high) rather than somatic mutation. Often associated with BRAF V600E mutation.
Clinical significance of MSI-H status:
- MSI-H tumours have an improved prognosis (enhanced immune surveillance)
- MSI-H rectal cancers can be treated for cure with PD-1 checkpoint inhibitors alone (without surgery, radiation, or chemotherapy) - a paradigm shift in management
- Universal tumour testing for MMR deficiency (IHC for MMR proteins or MSI PCR) is now recommended for all CRC specimens
4c. Consensus Molecular Subtypes (CMS)
An international consortium has identified four CMS of CRC:
- CMS1: MSI-high (Lynch-type or sporadic); right-sided
- CMS2: WNT and MYC signalling activation
- CMS3: Metabolic dysregulation
- CMS4: TGF-beta activation; worst prognosis
5. Pathology
5a. Distribution by Site
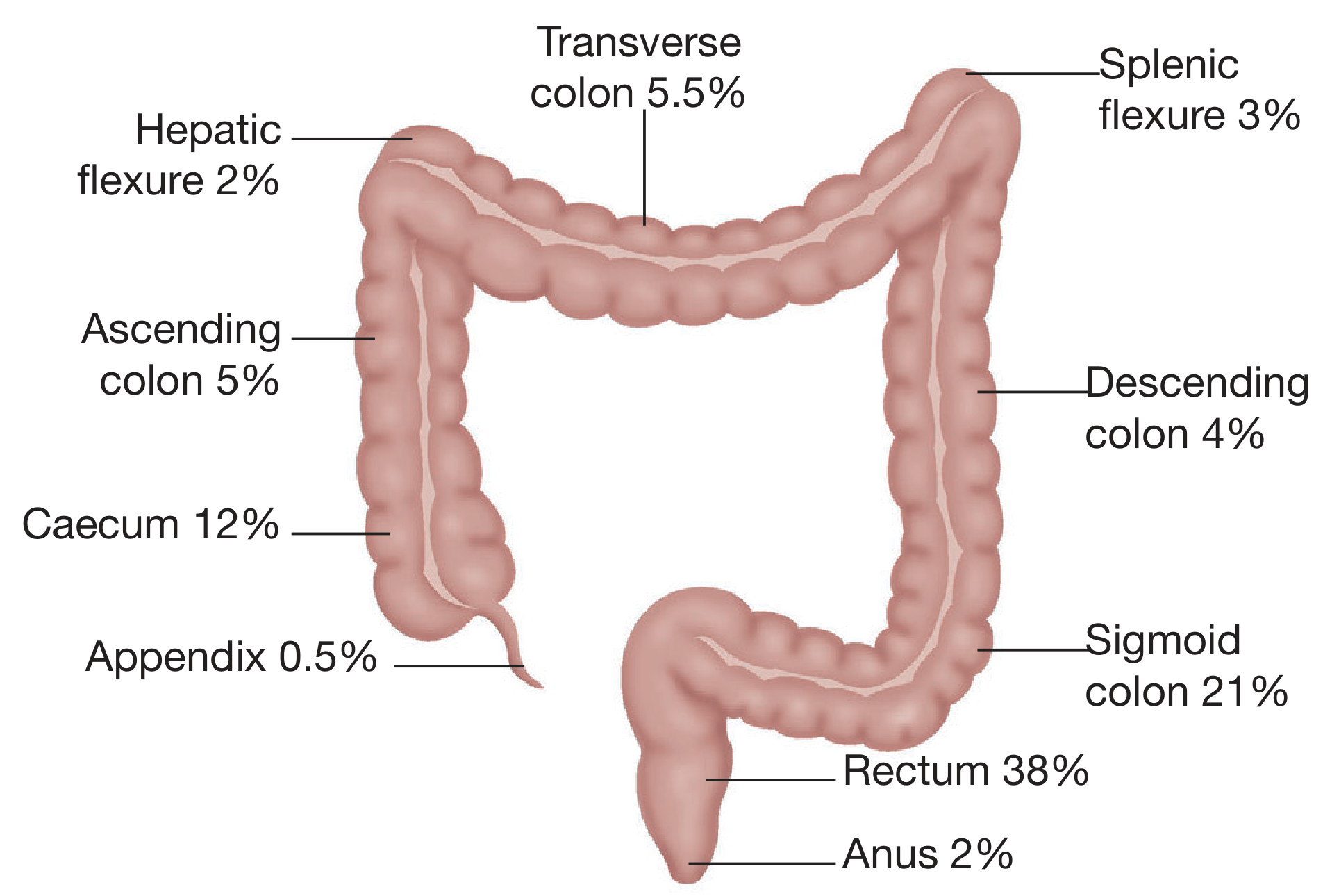
The rectum is the single most common site (38%), followed by the sigmoid colon (21%) and caecum (12%).
5b. Gross Morphology
- Right-sided tumours (caecum/ascending colon): Predominantly polypoid/exophytic masses that grow into the lumen. They bleed easily, causing chronic occult blood loss and iron-deficiency anaemia. Obstruction is less common as the stool is still liquid.
- Left-sided tumours (descending/sigmoid colon): Tend to grow in an annular, constricting ("apple-core" or "napkin ring") pattern. Cause obstruction and change in bowel habit because stool is more solid in the left colon.
- Rectal tumours: May be polypoid, ulcerating, or annular. Cause fresh rectal bleeding and tenesmus.
5c. Microscopy
Over 90% are columnar cell adenocarcinomas (mucin-secreting glands). Well-differentiated tumours show clear glandular formation; poorly differentiated tumours may show signet-ring cells or mucinous patterns. Poorly differentiated histology, perineural invasion, and venous invasion all worsen prognosis.
5d. Spread
- Local (direct): Longitudinally along the bowel wall; radially into pericolic fat, adjacent organs (bladder, uterus, posterior abdominal wall, duodenum)
- Lymphatic: Orderly progression from paracolic nodes → intermediate nodes → central/aortic nodes along the course of feeding vessels
- Haematogenous: Via portal vein to liver (most common; one-third of patients have liver metastases at diagnosis; 50% develop them at some point). Lung is the next most common site. Ovary, brain, kidney, bone are less common.
- Transcoelomic/Peritoneal: Spread along the peritoneal surface; may involve ovaries (Krukenberg tumour), omentum, peritoneum
6. Clinical Features
Symptoms vary critically depending on tumour site:
Right-sided Colon Cancer
- Iron-deficiency anaemia (occult bleeding, often without visible blood)
- Fatigue, weakness, pallor
- Palpable right iliac fossa mass
- Right-sided abdominal discomfort or pain
- Weight loss, anorexia (in advanced disease)
- The unexplained presence of iron-deficiency anaemia in any adult mandates endoscopic/radiographic visualisation of the entire large bowel
Left-sided Colon Cancer
- Change in bowel habit (alternating constipation and diarrhoea)
- Dark or altered rectal bleeding mixed with stool
- Abdominal cramping and colic
- Features of obstruction (abdominal distension, absolute constipation, vomiting)
- Radiological "apple-core" lesion on barium enema or CT colonography
Rectal Cancer
- Fresh rectal bleeding (most common presenting symptom)
- Tenesmus (sensation of incomplete evacuation)
- Mucous discharge per rectum
- Sensation of rectal fullness or mass
- Narrow/pencil-thin stools
- Note: rectal bleeding must never be attributed to haemorrhoids without a thorough examination
Features of Advanced/Metastatic Disease
- Hepatomegaly, jaundice (liver metastases)
- Ascites (peritoneal involvement)
- Supraclavicular lymphadenopathy (Virchow's node)
- Cachexia, anorexia, night sweats
7. Investigations
Blood tests:
- FBC (iron-deficiency anaemia)
- LFTs, ALP (liver metastases)
- Serum CEA - baseline must be obtained preoperatively; used for monitoring recurrence
Endoscopy:
- Colonoscopy: Gold standard; allows visualisation of entire colon, biopsy, and polypectomy. Must identify synchronous cancers (~3%) and synchronous polyps (~30%).
- Flexible sigmoidoscopy: If full colonoscopy not possible
Imaging:
- CT chest/abdomen/pelvis (contrast-enhanced): Standard for staging, assessment of lymph nodes, liver metastases
- Pelvic MRI: Mandatory for all rectal cancers - assesses T and N stage, circumferential resection margin (CRM), relationship to anterior peritoneal reflection
- Endorectal ultrasound: Useful for T-staging in rectal cancer; less accurate for nodal involvement
- CT colonography (virtual colonoscopy): Alternative when full colonoscopy not possible
- PET scan: Not routinely recommended for primary staging; useful for suspected recurrence
Histopathology:
- MMR protein immunohistochemistry (or MSI testing by PCR) on all resected CRC specimens
- Minimum 12 lymph nodes must be sampled for adequate staging
8. Staging
Dukes' Classification (historical, widely recognised)
| Stage | Definition |
|---|---|
| A | Invasion into but not breaching the muscularis propria |
| B | Breaches muscularis propria; no lymph node involvement |
| C | Lymph nodes involved (C1: apical node free; C2: apical node involved) |
| D | Distant metastases (added later; not described by Dukes himself) |
TNM Classification (AJCC - International Standard)
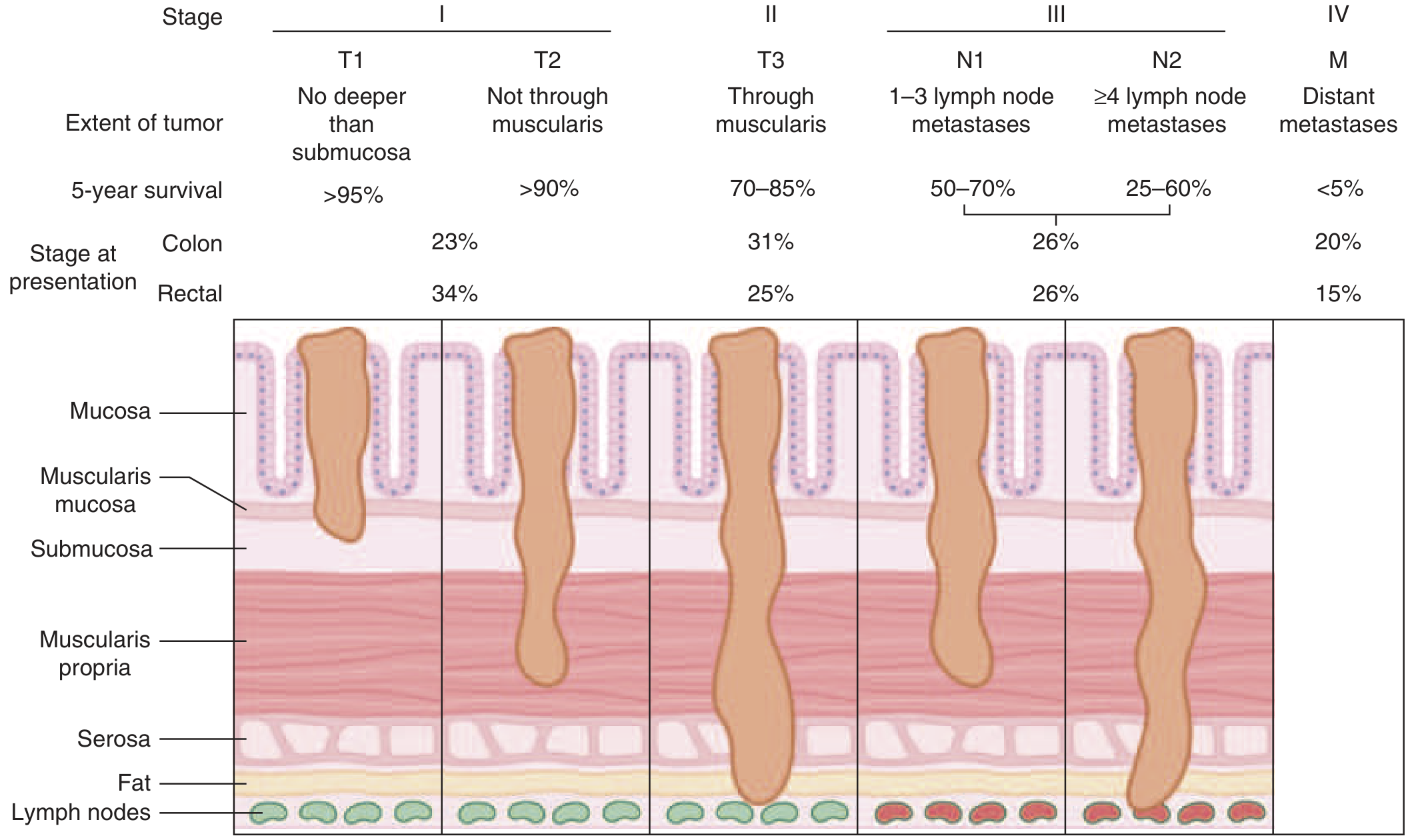
| Stage | TNM | Description | 5-Year Survival |
|---|---|---|---|
| Stage I | T1-2, N0, M0 | Confined to submucosa (T1) or muscularis (T2) | >90-95% |
| Stage II | T3-4, N0, M0 | Through muscularis into pericolic fat (T3) or adjacent organs (T4) | 70-85% |
| Stage III | Any T, N1-2, M0 | 1-3 (N1) or ≥4 (N2) positive lymph nodes | 25-70% |
| Stage IV | Any T, Any N, M1 | Distant metastases | <5% |
Key prognostic factors:
- Depth of tumour invasion (T stage)
- Number of positive lymph nodes (minimum 12 must be harvested)
- Histological grade (poorly differentiated = worse prognosis)
- Venous invasion, perineural invasion
- Circumferential resection margin (CRM) in rectal cancer
- MSI-H status - associated with improved prognosis despite right-sided location
- Perforation or obstruction at presentation (worse prognosis)
- Tumour size alone does not independently predict prognosis when adjusted for nodal status and differentiation
9. Screening
The rationale is that removal of adenomatous polyps prevents CRC and detection of early-stage cancers improves cure rates.
Recommended from age 45 (USPSTF 2021 update; earlier if high-risk)
| Method | Schedule | Notes |
|---|---|---|
| Faecal occult blood test (FOBT/gFOBT) | Annual | 50% false-negative rate; significantly reduces CRC mortality in prospective RCTs |
| Faecal immunochemical test (FIT) | Annual | More specific than gFOBT; preferred stool test |
| Multi-target stool DNA (Cologuard) | Every 1-3 years | Tests for DNA mutations + haemoglobin; more sensitive but less specific |
| Flexible sigmoidoscopy | Every 5 years | No sedation; misses ~1.5% proximal high-risk lesions; reduction in CRC incidence and mortality persists >15 years |
| Colonoscopy | Every 10 years | Gold standard; entire colon; requires bowel prep and sedation; allows polypectomy |
| CT colonography | Every 5 years | Non-invasive; any lesion requires colonoscopy for biopsy |
10. Treatment
10a. Surgical Management of Colon Cancer
Surgical resection remains the standard of care for localised disease. Principles:
- Wide resection with clear margins
- High ligation of the feeding vessel (ensures adequate lymph node clearance)
- Harvest of ≥12 lymph nodes
- Minimally invasive approaches (laparoscopic/robotic) have largely replaced open surgery
Operations by site:
| Tumour Location | Operation |
|---|---|
| Caecum / ascending colon | Right hemicolectomy |
| Hepatic flexure / proximal transverse colon | Extended right hemicolectomy |
| Splenic flexure | Segmental or extended right hemicolectomy |
| Descending colon | Left hemicolectomy (high IMA ligation) |
| Sigmoid colon | Sigmoid colectomy |
10b. Surgical Management of Rectal Cancer
Rectal cancer has unique challenges:
- Higher risk of local recurrence compared with colon cancer
- Anatomic constraints of the pelvis (ureters, bladder, prostate/vagina, iliac vessels, sacrum) make achieving negative radial margins more difficult
- Proximity of autonomic nerves
Surgical options:
- Low anterior resection (LAR): Sphincter-preserving resection; anastomosis proximal to the sphincter; a defunctioning loop ileostomy is usually fashioned temporarily
- Abdominoperineal resection (APR): Combined abdominal and perineal approach; required when the tumour invades the sphincter; results in permanent colostomy. Historically associated with high local recurrence rates.
- Local excision (transanal/TEM/TAMIS): Suitable only for select T1 tumours (<3 cm, well/moderately differentiated, no LVI); does not allow nodal assessment; local recurrence rates high (20-40%)
Total Mesorectal Excision (TME):
TME - introduced by Bill Heald - is the cornerstone of modern rectal cancer surgery. It involves:
- Sharp dissection within the embryological avascular plane between the visceral fascia propria of the rectum and the parietal presacral fascia
- Removing the entire mesorectal fat envelope (with its blood vessels, lymphatics, and lymph nodes) as an intact, undisturbed package
- This ensures removal of all potential micrometastatic disease and a clear circumferential resection margin (CRM)
- For upper rectal tumours, a partial/tumour-specific mesorectal excision with at least 5 cm distal mesorectal clearance is acceptable
- TME reduces local recurrence from ~30-40% to <10% and improves long-term survival
Autonomic nerve preservation during TME:
- Hypogastric plexus (L1-L3): At risk during high IMA ligation and posterior dissection over the sacral promontory - injury causes retrograde ejaculation
- Pelvic plexus/nervi erigentes (S2-S4): At risk during lateral dissection - injury causes erectile dysfunction and atonic bladder
- Periprostatic plexus: At risk during anterior dissection - erectile dysfunction
10c. Adjuvant and Neoadjuvant Therapy
Colon cancer:
- Stage I: Surgery alone; patients considered cured
- High-risk Stage II and Stage III: Adjuvant chemotherapy (fluoropyrimidine ± oxaliplatin for 3-6 months) improves survival by ~30%
- CEA surveillance every 3 months for 5 years post-resection
- Colonoscopy at 1 year, then every 3 years
Rectal cancer:
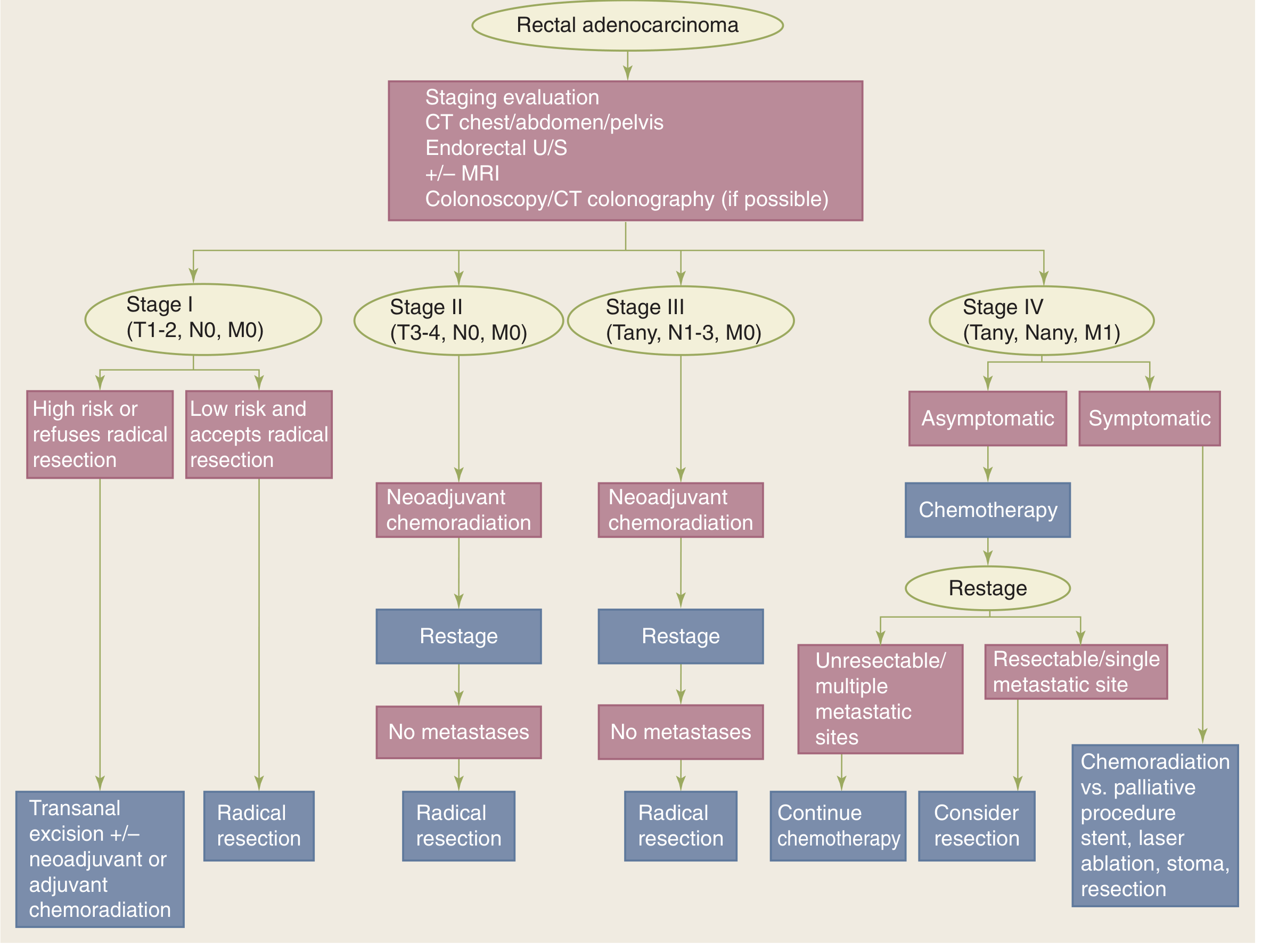
- Stage I: Radical resection; local excision only for selected low-risk T1 lesions
- Stage II-III: Neoadjuvant chemoradiation (5-FU-based long-course CRT or short-course 5×5 Gy radiotherapy) before surgery:
- Reduces local recurrence rates significantly
- Allows downsizing/downstaging, potentially enabling sphincter preservation
- Pre-operative approach preferred over post-operative due to better tumour radiosensitivity, lower toxicity, and improved compliance
- Total Neoadjuvant Therapy (TNT): Full systemic chemotherapy + radiation before surgery achieves higher complete response rates
- Watch-and-wait (organ preservation): Patients with complete clinical response after CRT may have surgery deferred; requires intensive endoscopic and MRI surveillance. Tumour regrowth occurs in ~25-30%.
- MSI-H rectal cancer: PD-1 checkpoint inhibitors (pembrolizumab, dostarlimab) achieve clinical complete response in a significant proportion, potentially avoiding surgery altogether
Metastatic (Stage IV):
- FOLFOX (5-FU + leucovorin + oxaliplatin) or FOLFIRI (5-FU + leucovorin + irinotecan) ± bevacizumab (anti-VEGF) or cetuximab/panitumumab (anti-EGFR, only for RAS wild-type)
- Resection of isolated liver or lung metastases can be curative in selected patients
- Palliative: colonic stenting, defunctioning stoma, laser ablation, best supportive care
11. Hereditary Colorectal Cancer Syndromes (Detailed)
Familial Adenomatous Polyposis (FAP)
- Gene: APC (chromosome 5q21); autosomal dominant; 1 in 10,000 births; up to 1/3 are de novo mutations
- APC function: Forms a complex that degrades beta-catenin (WNT pathway). Loss of APC → beta-catenin accumulates → nuclear translocation → drives cell proliferation
- Phenotype: Hundreds to thousands of colonic adenomas by late teenage years; 100% risk of CRC if untreated (median age 40)
- Extracolonic: Desmoid tumours, congenital hypertrophy of retinal pigment epithelium (CHRPE), osteomas (Gardner's syndrome), brain tumours (Turcot's syndrome)
- Management: Prophylactic colectomy (total colectomy + IPAA, or subtotal colectomy + ileorectal anastomosis). NSAIDs (sulindac, celecoxib) cause polyp regression but do not reliably prevent CRC. Follow-up for extracolonic manifestations.
Lynch Syndrome (HNPCC)
- Most common inherited CRC predisposition; ~3% of all CRC; up to 17-fold increased risk
- Gene: Germline mutation in MMR genes - MLH1 (Chr 3p22), MSH2 (Chr 2p21), MSH6 (Chr 2p16), PMS2 (Chr 7p22); also EPCAM deletion causing MSH2 loss
- MMR failure → microsatellite instability → ~1000-fold more mutations than MMR-proficient tumours
- Extracolonic cancers: Endometrium (most common), ovary, stomach, small bowel, urinary tract, pancreaticobiliary, brain (Turcot), skin (Muir-Torre)
- Diagnosis: Amsterdam II Criteria (3 affected relatives including 1 first-degree relative, 2 successive generations, one diagnosis <50 years, FAP excluded). Universal tumour testing by MMR IHC or MSI PCR. Germline testing with genetic counselling.
- Surveillance: Colonoscopy every 1-2 years from age 25 (MLH1/MSH2) or 35 (MSH6); every 5 years from 35 for PMS2. Gynaecological screening per 2019 Manchester Consensus.
- Surgery: Extended colectomy (rather than segmental) recommended when cancer develops, to reduce risk of metachronous CRC
12. Prognosis and Follow-up
- The liver represents the most frequent visceral site of metastasis (via the portal vein); one-third of patients have liver metastases at diagnosis, and 50% eventually develop them
- The majority of recurrences occur within the first 5 years after resection
- Anastomotic recurrences are infrequent when margins are adequate
- After curative resection, patients with a previous CRC have a 3-5% risk of a second colorectal carcinoma and a >15% risk of new adenomatous polyps during their lifetime
- Post-resection surveillance: CEA every 3 months × 5 years; CT chest/abdomen/pelvis semi-annually to annually × 3 years; colonoscopy at 1 year then every 3 years
13. Summary of Key Points
| Topic | Key Points |
|---|---|
| Most common histology | Adenocarcinoma (>90%) |
| Most common site | Rectum (38%), then sigmoid (21%) |
| Most common precursor | Adenomatous polyp (adenoma-carcinoma sequence over ~10-15 years) |
| Most common distant metastasis site | Liver (via portal vein) |
| Most important prognostic factor | Stage (depth of invasion + nodal status) |
| Most common inherited syndrome | Lynch syndrome (HNPCC) |
| Key surgical principle for rectal cancer | Total mesorectal excision (TME) |
| Key molecular test | MMR/MSI status (guides prognosis and immunotherapy eligibility) |
| Standard adjuvant chemo (colon) | FOLFOX / fluoropyrimidine ± oxaliplatin |
| Minimum lymph nodes required for staging | 12 nodes |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Bailey & Love's Short Practice of Surgery 28th Ed.; Schwartz's Principles of Surgery 11th Ed.; Robbins & Kumar Pathologic Basis of Disease; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.