Myocardial infraction
Reading File
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
myocardial infarction pathology gross specimen histology
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough answer.
Myocardial Infarction (MI)
Definition
MI — commonly called a "heart attack" — is the death of cardiac muscle due to prolonged ischemia, most often caused by atherosclerotic coronary artery disease (CAD). Roughly 800,000 individuals in the United States experience an MI each year (nearly one every 40 seconds), causing ~400,000 deaths annually. Although MIs can occur at virtually any age, 45% occur in people younger than 65 years.
— Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis
Coronary Arterial Occlusion
The typical sequence of events:
- An atheromatous plaque is disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces — exposing subendothelial collagen and necrotic plaque contents to blood.
- Platelets adhere, aggregate, and activate, releasing thromboxane A₂, ADP, and serotonin → further platelet aggregation and vasospasm.
- Coagulation activation (via tissue factor) adds to the growing thrombus.
- Within minutes, the thrombus can completely occlude the coronary lumen.
When angiography is performed within 4 hours of onset, thrombotic occlusion is found in ~90% of cases.
In ~10% of cases, MI occurs without typical atherothrombosis. Alternative mechanisms include:
- Vasospasm (e.g., cocaine, ephedrine)
- Embolism (from mural thrombus, infective endocarditis vegetations, patent foramen ovale)
- Vasculitis, sickle cell disease, amyloid deposition, aortic dissection, cardiogenic shock
Myocardial Response to Ischemia
| Feature | Time |
|---|---|
| Onset of ATP depletion | Seconds |
| Loss of contractility | < 2 minutes |
| ATP reduced to 50% of normal | 10 minutes |
| ATP reduced to 10% of normal | 40 minutes |
| Irreversible cell injury | 20–40 minutes |
| Microvascular injury | > 1 hour |
Only severe ischemia (blood flow ≤10% of normal) lasting 20–40 minutes causes irreversible necrosis. Progressive loss of viability becomes complete by 6–12 hours. The subendocardial zone is affected first because it is the last area to receive blood from epicardial vessels and is exposed to the highest intramural pressures.
— Robbins, Cotran & Kumar; Guyton & Hall Textbook of Medical Physiology
Patterns of Infarction
By Coronary Artery Involvement (in right-dominant hearts)
| Artery | Frequency | Area Infarcted |
|---|---|---|
| Left anterior descending (LAD) | 40–50% | Anterior LV wall, anterior septum, apex |
| Right coronary artery (RCA) | 30–40% | Inferior/posterior LV wall, posterior septum |
| Left circumflex (LCx) | 15–20% | Lateral LV wall |
By Depth
- STEMI (transmural / ST-elevation MI): Full-thickness necrosis; associated with complete coronary occlusion
- NSTEMI (subendocardial / non-ST-elevation MI): Partial thickness; inner layer of myocardium
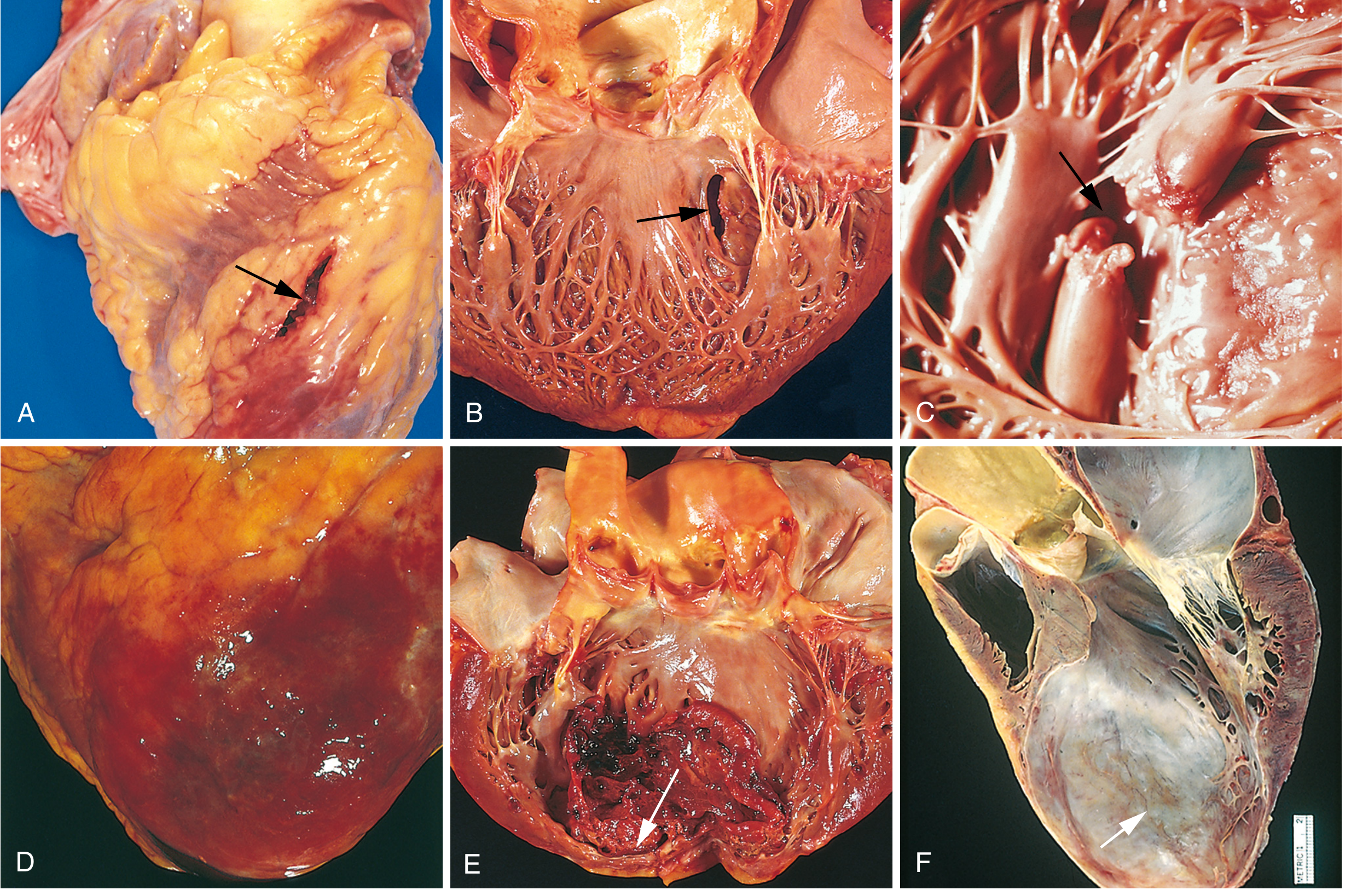
Morphologic Changes Over Time
| Time | Gross Changes | Microscopic Changes |
|---|---|---|
| < 12 hours | Usually not visible | Wavy fibers; hypereosinophilic myocytes |
| 12–24 hours | Reddish-blue discoloration (congestion) | Coagulative necrosis begins |
| 3–7 days | Yellow-tan soft area, rimmed by hyperemic granulation tissue | Neutrophil infiltration, then macrophages |
| Weeks | Progressive fibrosis | Granulation tissue → fibrous scar |
Detection technique: Triphenyl tetrazolium chloride (TTC) stain — viable myocardium stains brick-red; infarcted area appears as an unstained pale zone.
ECG Changes
Three major abnormalities occur in acute MI:
| Defect in Infarcted Cells | Current Flow | ECG Change |
|---|---|---|
| Rapid repolarization | Out of infarct | ST segment elevation |
| Decreased resting membrane potential | Into infarct | TQ depression (manifested as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
- Hallmark of acute MI: ST elevation in leads overlying the infarct; reciprocal ST depression in opposite leads
- After days–weeks: ST normalizes; Q waves appear; "failure of R wave progression" in anterior infarcts
- Non-Q-wave infarcts tend to be less severe but carry a high risk of subsequent reinfarction
— Ganong's Review of Medical Physiology
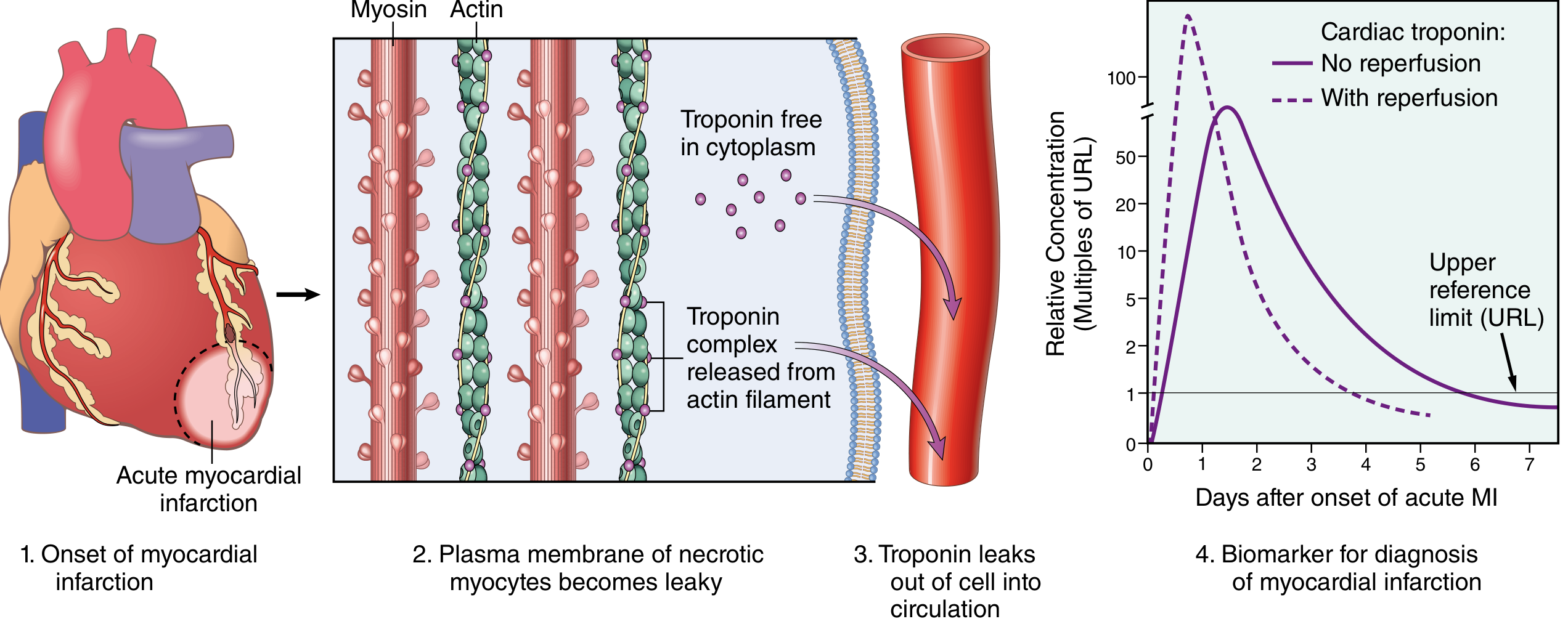
Biomarkers
The most clinically useful biomarkers are cardiac troponins I and T (cTnI, cTnT):
| Marker | Rises | Peaks | Returns to Normal |
|---|---|---|---|
| Cardiac Troponin I/T | 2–4 hours | 24–48 hours | 7–10 days |
| CK-MB | 4–6 hours | 12–24 hours | 48–72 hours |
With reperfusion, troponins may peak earlier due to rapid washout. Low-level troponin elevation ("troponin leak") can occur in CHF, PE, renal failure, and sepsis — serial measurements help distinguish etiologies.
Treatment
Initial Management (STEMI)
| Intervention | Details |
|---|---|
| Aspirin | 160–325 mg chewed immediately; then 75–162 mg/day |
| P2Y12 inhibitor | Clopidogrel, ticagrelor, or prasugrel (dual antiplatelet therapy) |
| Anticoagulation | Unfractionated heparin, LMWH, direct thrombin inhibitors, or factor Xa inhibitors |
| Oxygen | Only if SpO₂ < 90% — supplemental O₂ is NOT recommended in normoxic patients |
| Nitroglycerin (sublingual) | Up to 3 doses × 0.4 mg q5 min for ongoing ischemic pain; avoid if SBP < 90 mmHg, RV infarction, or PDE5 inhibitor use within 24 h |
| Morphine | 2–4 mg IV q5 min for pain; watch for bradycardia and hypotension |
| Beta blockers | IV metoprolol 5 mg q2–5 min × 3 doses if HR > 60, SBP > 100, PR < 0.24 s, no acute HF |
Reperfusion Therapy (cornerstone of STEMI management)
- Primary PCI (preferred): Goal = within 90 minutes of first medical contact (120 min if transfer required)
- Fibrinolysis: Used if PCI unavailable within 120 min of first medical contact
The rationale: only severe ischemia lasting 20–40 minutes causes irreversible necrosis. Early reperfusion salvages at-risk myocardium.
— Harrison's Principles of Internal Medicine 22E; Robbins, Cotran & Kumar
Complications
Nearly three-quarters of patients experience one or more complications post-MI:
| Complication | Details |
|---|---|
| Contractile dysfunction / Cardiogenic shock | Occurs in ~10% of transmural MIs; typically when ≥40% of LV is damaged |
| Arrhythmias | Ventricular fibrillation is the most common cause of early death; heart block in inferior MI |
| Papillary muscle dysfunction/rupture | Leads to acute mitral regurgitation |
| Myocardial rupture | Free wall rupture → hemopericardium/tamponade; septal rupture → VSD |
| Right ventricular infarction | Complicates RCA occlusions; causes right-sided heart failure and hypotension |
| Fibrinous pericarditis | Typical 2–4 days post-MI (Dressler syndrome appears later) |
| Mural thrombus | Over akinetic/dyskinetic segments → risk of systemic embolism |
| LV aneurysm | Late complication from scar bulging; predisposes to arrhythmia and thrombus |
Causes of Death
- Decreased cardiac output (cardiogenic shock) — systolic stretch worsens pump failure
- Pulmonary edema from acute LV failure
- Ventricular fibrillation
- Cardiac rupture (less common)
Out-of-hospital mortality for STEMI remains ~33%, most dying of arrhythmia within 1 hour before receiving care.
— Guyton & Hall Textbook of Medical Physiology; Robbins, Cotran & Kumar
Key Summary
| STEMI | NSTEMI | |
|---|---|---|
| ECG | ST elevation | ST depression or T-wave changes; no ST elevation |
| Occlusion | Complete | Partial |
| Depth | Transmural | Subendocardial |
| Troponin | Elevated | Elevated |
| In-hospital mortality | ~9% | ~6% |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology; Harrison's Principles of Internal Medicine 22E
Effect of daily smoking on a 20 year old
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cigarette smoking" AND "young adults" AND health effects
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive data from authoritative sources. Here is a thorough answer.
Effects of Daily Smoking on a 20-Year-Old
Starting and maintaining daily smoking at age 20 sets in motion a cascade of pathological changes that compound over decades. The harm is not merely a "future risk" — many effects begin within months of regular use.
What's in Cigarette Smoke
Tobacco smoke contains >7,000 chemicals, more than 60 confirmed carcinogens:
| Substance | Primary Harm |
|---|---|
| Tar / Polycyclic aromatic hydrocarbons (PAHs) | Carcinogenesis (lung, esophagus, bladder) |
| Nicotine | Addiction; ganglionic stimulation; tumor promotion; fetal neurotoxicity |
| Carbon monoxide (CO) | Impairs oxygen transport and utilization; cardiac hypoxia |
| Benzo[a]pyrene | Direct DNA adduct formation → oncogenic mutations |
| Formaldehyde / Nitrogen oxides | Ciliotoxicity; mucosal irritation |
| Nitrosamines (e.g., NNK, NNN) | Lung, esophageal, and oral carcinogenesis |
— Robbins, Cotran & Kumar Pathologic Basis of Disease
1. Addiction — Happens First
Nicotine binds to nicotinic acetylcholine receptors in the brain, triggering dopamine release and stimulating catecholamine secretion from sympathetic neurons. This produces:
- Increased heart rate, blood pressure, and cardiac output (acute effects)
- Rapid, powerful psychological dependence
- Recidivism rates > 50% even with cessation treatment
More than 80% of adult smokers began before age 18. A 20-year-old who smokes daily is already likely nicotine-dependent. The addictive effects of nicotine can persist for years after cessation.
Electronic cigarettes deliver high doses of nicotine to developing organs, including the brain — representing a major public health threat for young people who may not have otherwise smoked.
— Harrison's Principles of Internal Medicine 22E
2. Cardiovascular System
This is the leading cause of smoking-related death — more deaths from cardiovascular disease than from cancer.
- ~20% of all cardiovascular deaths in the US are caused by cigarette smoking
- Mechanisms:
- Increased platelet aggregation → thrombosis
- CO in smoke → decreased myocardial oxygen supply + hypoxia
- Nicotine → increased myocardial oxygen demand
- Decreased threshold for ventricular fibrillation
- Multiplicative risk when combined with hypertension or hypercholesterolemia
- Accelerates atherosclerosis → higher lifetime risk of MI and stroke
- Erectile dysfunction (vascular insufficiency) — even in young men
At 20 years old, atherosclerotic plaques begin to develop at an accelerated rate. What would take decades in a non-smoker is compressed into years.
3. Lungs and Respiratory System
- Cigarette smoke directly irritates the tracheobronchial mucosa → chronic bronchitis (increased mucus production, productive cough)
- Recruits leukocytes to lung tissue → increases local elastase → progressive destruction of alveolar walls → emphysema
- Together: COPD — the most common non-cancer smoking disease, irreversible
- Exacerbates asthma
- Increases risk of pulmonary tuberculosis
- Impairs mucociliary clearance (via formaldehyde and nitrogen oxides)
A 20-year-old who smokes daily begins accumulating "pack-years." COPD symptoms often don't appear until middle age — but the silent destruction begins now. Only ~50% of long-term smokers reach age 70 vs. ~75% of non-smokers.
4. Cancer Risk
Smoking causes cancers in multiple organs, including:
| Cancer Site | Mechanism |
|---|---|
| Lung, larynx | PAHs, NNK, Polonium-210 — form DNA adducts → mutations |
| Esophagus | NNN via saliva contact |
| Bladder, kidney | Carcinogen excretion through urine |
| Pancreas, stomach, colon | Systemic carcinogen absorption |
| Uterine cervix | Immunosuppression + carcinogens |
| Oral cavity / Oropharynx | Direct mucosal exposure |
Lung cancer genome sequencing of smokers reveals thousands of mutations of the type caused specifically by tobacco carcinogens.
The number of cigarettes smoked per day directly correlates with lung cancer mortality risk. Light- and low-tar cigarettes are not safer — smokers compensate by inhaling more frequently and deeply.
5. Skin, Appearance, and Musculoskeletal Effects
- Premature facial wrinkling (documented in studies of smokers vs. age-matched non-smokers)
- Impaired wound healing
- Increased risk of rheumatoid arthritis
- Reduced bone density (risk factor for osteoporosis later in life)
6. Other Systemic Effects
- Type 2 diabetes — added to the Surgeon General's official list in 2016
- Age-related macular degeneration — leading cause of blindness in older adults
- Ectopic pregnancy risk increased (fallopian tube ciliary damage)
- Impaired immune function
- Second-hand smoke: Children in the household of a smoker have significantly higher rates of respiratory illness and asthma
7. Why Starting at 20 Is Particularly Harmful
- Developing brain — The prefrontal cortex is still maturing until ~age 25. Nicotine exposure during this period alters neuroplasticity, deepens addiction, and may affect executive function.
- Long time horizon — Starting at 20 and smoking for 40+ years accumulates enormous pack-years, dramatically compounding cancer and COPD risk.
- Atherosclerosis starts early — Vascular changes begin within the first few years, not at age 50.
- Addiction locks in the habit — The earlier the habit is established, the harder cessation becomes.
8. Is Quitting Worth It?
Yes — and the earlier, the better:
| Time After Quitting | Benefit |
|---|---|
| 20 minutes | Heart rate and BP drop |
| 12 hours | CO level normalizes |
| Weeks | Lung function improves; circulation recovers |
| 5 years | Risk of heart disease drops dramatically |
| 5 years | Lung cancer mortality decreases ~20% |
| 10 years | Lung cancer risk falls 30–50% |
However, excess lung cancer risk persists for several decades after cessation because carcinogen-induced gene mutations remain. Quitting before significant damage is done — ideally before age 30 — largely eliminates this excess risk.
"Smoking cessation and avoidance would save more lives from cancer than any other public health activity." — Harrison's Principles of Internal Medicine 22E
Bottom line: For a 20-year-old, daily smoking causes immediate addiction and cardiovascular stress, and silently initiates COPD, atherosclerosis, and carcinogenesis that will manifest clinically in middle age. The habit shortens life expectancy by an average of one decade. Cessation at this age, before significant irreversible tissue damage has accumulated, offers the greatest potential for recovery.
— Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E; Fuster and Hurst's The Heart
This is a shared conversation. Sign in to Orris to start your own chat.