Pyogenic brain abscess
Reading File
Finding Sources
Finding Sources
Searching PubMed
"brain abscess" AND pyogenic
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content. Let me compile the full answer.
Pyogenic Brain Abscess
A brain abscess is a focal, suppurative infection within the brain parenchyma, typically surrounded by a vascularized fibrous capsule. The term cerebritis describes the nonencapsulated early form.
Epidemiology
Incidence is ~0.3–1.3 per 100,000 persons per year. Predisposing conditions include otitis media/mastoiditis, paranasal sinusitis, pulmonary infections, penetrating head trauma, neurosurgical procedures, and dental infections.
Etiology & Microbiology
In immunocompetent individuals:
| Organism | Approximate Frequency |
|---|---|
| Streptococcus spp. (anaerobic, aerobic, viridans — esp. S. milleri) | 40% |
| Anaerobes (Bacteroides, Fusobacterium) | 30% |
| Enterobacteriaceae (Proteus, E. coli, Klebsiella) | 25% |
| Staphylococci | 10% |
In immunocompromised hosts: Nocardia, Toxoplasma gondii, Aspergillus, Candida, Cryptococcus predominate.
Routes of Infection
A brain abscess develops by one of three mechanisms:
- Direct spread from a contiguous site — paranasal sinusitis, otitis media, mastoiditis, dental infection (accounts for the majority)
- Post-traumatic / post-neurosurgical — compound skull fractures, operative contamination (~10%)
- Hematogenous spread — from pulmonary infections (abscess, bronchiectasis), infective endocarditis, or bacteremia (~25%); congenital heart disease with right-to-left shunting bypasses pulmonary filtration
- Cryptogenic — no source identified in up to 25% of cases
Location by source:
- Otogenic → temporal lobe (55–75%) or cerebellum (20–30%); organisms: streptococci, Bacteroides, Pseudomonas, Enterobacteriaceae
- Sinogenic / frontal sinus → frontal lobe; organisms: streptococci (S. milleri), Haemophilus, Bacteroides, S. aureus
- Hematogenous → gray-white matter junction, often multiple, in the distribution of the middle cerebral artery
Pathogenesis & Stages
For bacterial invasion to occur, preexisting ischemia, necrosis, or hypoxemia in brain tissue is necessary — the intact parenchyma is relatively resistant.
| Stage | Timing | Pathology |
|---|---|---|
| Early cerebritis | Days 1–3 | Perivascular inflammatory infiltrate, central coagulative necrosis, marked edema |
| Late cerebritis | Days 4–9 | Pus formation, enlarging necrotic center, macrophage/fibroblast infiltrate, thin capsule begins forming |
| Early capsule formation | Days 10–13 | Capsule better developed on cortical side; ring enhancement appears on imaging |
| Late capsule formation | Day 14+ | Dense collagenous capsule, edema regresses, reactive gliosis develops (→ seizures) |
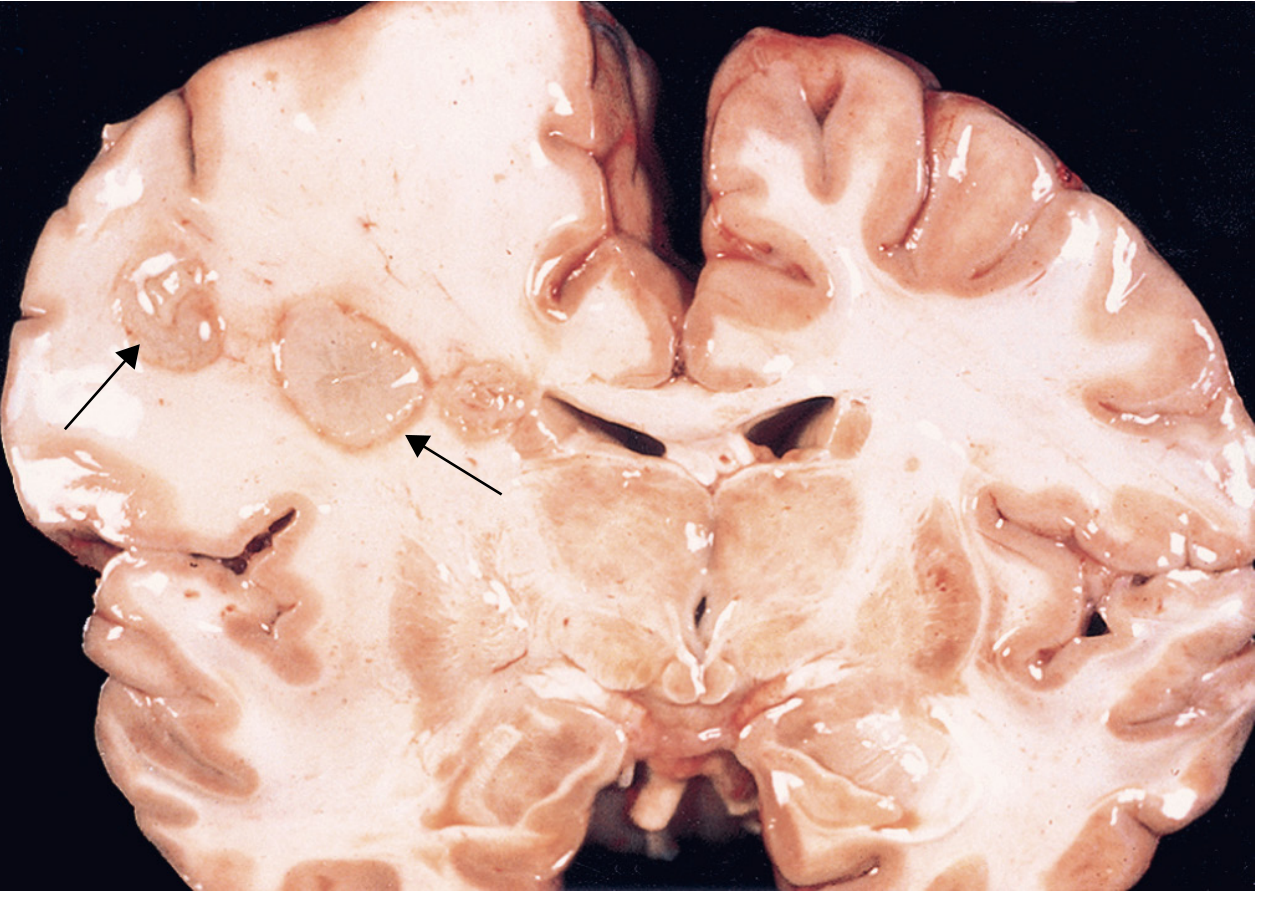
Macroscopic pathology: Discrete lesion with central pus and liquefactive necrosis, surrounded by brain swelling; exuberant neovascularization at the outer margin accounts for marked vasogenic edema.
Clinical Presentation
Brain abscess typically presents as an expanding intracranial mass lesion rather than an acute infection. Most patients present ~11–12 days after symptom onset.
Classic triad (headache + fever + focal neurologic deficit) is present in <50% of cases.
| Feature | Frequency |
|---|---|
| Headache (dull, constant, progressive) | >75% |
| Fever | ~50% |
| Focal neurologic deficits (hemiparesis, aphasia, visual field defects) | >60% |
| Seizures (new onset, focal or generalized) | 15–35% |
| Signs of raised ICP (papilledema, nausea/vomiting, drowsiness) | Variable |
Meningismus is absent unless the abscess ruptures into the ventricle or spreads to the subarachnoid space.
Localization by deficit:
- Frontal lobe → hemiparesis (most common)
- Temporal lobe → dysphasia, upper homonymous quadrantanopia
- Cerebellar → nystagmus, ataxia (signs of raised ICP often dominate)
Diagnosis
Neuroimaging
MRI is the modality of choice — superior to CT for early cerebritis and posterior fossa lesions.
| Sequence/Modality | Cerebritis | Mature Abscess |
|---|---|---|
| T1-weighted MRI | Low signal, irregular Gd-enhancement | Ring-enhancing lesion |
| T2-weighted MRI | High signal (edema) | High signal core, low-signal capsule |
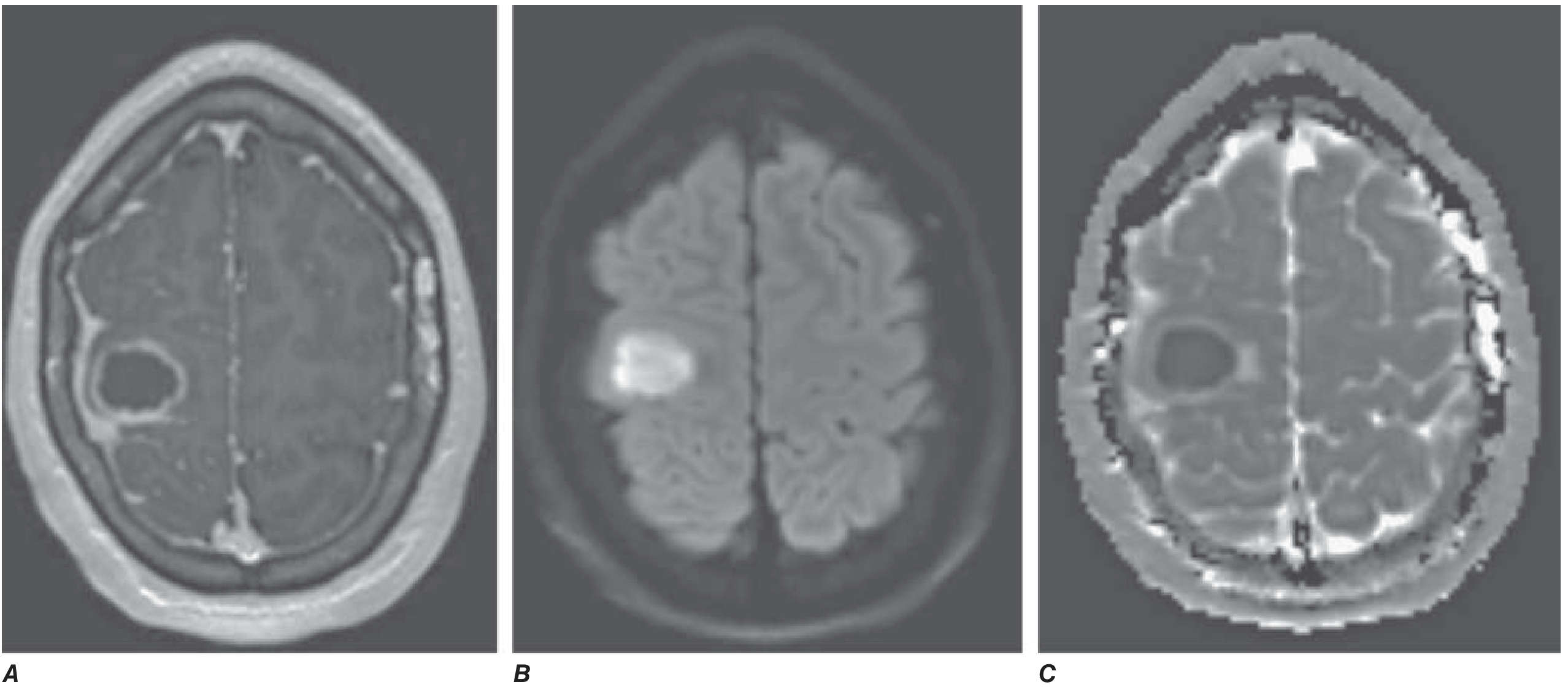
| DWI | — | Restricted diffusion (bright on DWI, dark ADC) — key distinguishing feature from tumor |
| CT (contrast) | Often normal or subtle hypodensity | Ring-enhancing mass with hypodense center |
DWI restricted diffusion is the critical feature that differentiates abscess from ring-enhancing tumors (glioblastoma, metastases) — the pus cavity restricts diffusion, whereas tumor necrosis does not.
CSF
Lumbar puncture is contraindicated if there is papilledema or evidence of mass effect (risk of herniation). When performed (e.g., if abscess has ruptured): elevated WBC, elevated protein, normal glucose — unlike bacterial meningitis.
Blood tests
- Peripheral leukocytosis and elevated CRP/ESR are common but nonspecific
- Blood cultures: positive in a minority
Treatment
Management requires combined medical and surgical therapy in most cases.
Antibiotics
Empiric IV antibiotic regimen pending culture:
| Clinical Setting | Regimen |
|---|---|
| Unknown source (community) | Metronidazole + ceftriaxone (± vancomycin if post-traumatic/nosocomial) |
| Post-traumatic / post-neurosurgical | Vancomycin + ceftazidime or meropenem |
| Otogenic / sinogenic | Metronidazole + ceftriaxone |
| Endocarditis-associated | Per valve organism (include S. aureus cover) |
Duration: 4–8 weeks of IV antibiotics (total therapy often 6–8 weeks with step-down to oral in selected cases).
Surgery
- CT/MRI-guided stereotactic aspiration: preferred approach; minimally invasive, diagnostic and therapeutic
- Surgical excision: for multiloculated abscesses, abscesses that fail aspiration, traumatic abscesses with foreign bodies, fungal abscesses
- Medical management alone: small abscesses (<2.5 cm), early cerebritis stage, surgically inaccessible location
Adjunctive therapy
- Dexamethasone: use is controversial; indicated if there is significant mass effect or cerebral herniation, but may impair capsule formation and antibiotic penetration — minimize and taper early
- Antiepileptics: prophylactic use for seizures; continue for ≥3 months post-treatment given gliosis risk
Complications
- Cerebral herniation (most fatal complication)
- Abscess rupture → ventriculitis or meningitis (dramatic worsening)
- Venous sinus thrombosis
- Seizures (post-abscess epilepsy due to gliosis)
Prognosis
With surgery and antibiotics, mortality has been reduced to <10% in modern series. Poor prognostic factors include: rapid clinical deterioration, deep/multiple abscesses, ventricular rupture, and delayed diagnosis.
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 1179 | Adams & Victor's Principles of Neurology 12E | Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.