Biomechanics of knee - 15 marks MPT level answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the data I need to write a comprehensive MPT-level answer. Let me compose it.
Biomechanics of the Knee Joint
(MPT Level - 15 Marks)
Introduction
The knee is the largest and most complex joint in the human body. It is a modified hinge joint (ginglymus) that incorporates rolling, sliding, and rotation, making its biomechanics far more sophisticated than a simple pulley. It must simultaneously provide stability for weight-bearing and mobility for locomotion, stair climbing, and sitting.
I. Osseous Geometry and Axes
Mechanical vs. Anatomical Axis
The femur has different anatomical and mechanical axes due to the proximal offset at the hip (neck-shaft angle). The anatomical axis of the femur is angled ~6-7° from the vertical mechanical axis (line from centre of femoral head to the ankle). In a normal tibia, both axes coincide. The tibiofemoral angle in the frontal plane is approximately 170-175° (5-7° of physiological valgus). This alignment directs weight-bearing forces medially and is critical in understanding osteoarthritis patterns and knee replacement mechanics.
Condylar Asymmetry
The medial and lateral femoral condyles differ in shape and size. The medial condyle is larger and extends more distally; its radius of curvature is smaller than the lateral condyle. This asymmetry is fundamental to the "screw-home" mechanism (see below). The tibial plateau is correspondingly concave medially (shallow, more stable) and convex laterally (shallow, more mobile).
II. Kinematics - Motion Analysis
Range of Motion
| Motion | Average Range | Functional Range |
|---|---|---|
| Flexion | 0-145° | 90° (117° to squat) |
| Extension | 0° (up to -3° hyperextension) | 0° |
| Internal rotation (at 90° flexion) | 30° | - |
| External rotation (at 90° flexion) | 45° | - |
(Source: Miller's Review of Orthopaedics, 9th Ed.)
Rotational mobility is maximum at 30-60° of flexion when ligamentous tension is lowest. In full extension, the knee is "locked" and rotation is minimal.
Rolling, Gliding, and Spinning
Knee motion involves a combination of three movements at the tibiofemoral surface:
- Rolling (rocking): The femoral condyles roll on the tibial surface like a wheel. If pure rolling occurred throughout, the femur would roll off the back of the tibia during flexion.
- Gliding (sliding): To prevent this, sliding occurs simultaneously in the opposite direction to rolling. This rolling-to-sliding ratio changes throughout the arc of motion - predominantly rolling in early flexion, predominantly sliding in deeper flexion.
- Spinning (axial rotation): Rotation occurs particularly during the terminal phase of extension (screw-home mechanism).
The instant centre of rotation (ICR) is not fixed - it traces a J-shaped (polycentric) curve that moves posteriorly as the knee flexes, which has major implications for prosthesis design and ligament reconstruction.
Four-Bar Linkage Model
The tibiofemoral kinematics are classically described using the four-bar linkage analogy:
- The four "bars" are the ACL, PCL, and the two tibial and femoral attachment lines
- As the knee flexes, the intersection of the cruciate ligaments defines the moving centre of rotation
- This model explains the coupled rolling-gliding motion and posterior femoral rollback during flexion
(Source: Miller's Review of Orthopaedics, 9th Ed.)
III. The Screw-Home Mechanism
This is one of the most MPT-exam-critical concepts in knee biomechanics.
Definition: During the last 10-15° of knee extension, the tibia automatically externally rotates (or, viewed from above, the femur internally rotates) approximately 5-10°, "locking" the joint into a stable, close-packed position.
Mechanism:
- Produced by the difference in radii of curvature of the medial vs. lateral femoral condyles
- The lateral condyle completes its arc of rolling before the medial condyle, forcing external tibial rotation
- The PCL acts as the rotational axis and appears to guide the screw-home mechanism during terminal extension
- The surrounding musculature, particularly the popliteus, contributes
"Unlocking": To initiate flexion from full extension, the popliteus muscle internally rotates the tibia ~5° to "unlock" the joint - described as the key to the knee.
Clinical relevance: Loss of screw-home (e.g. in ACL/PCL deficiency, arthritis) reduces terminal extension stability and may contribute to giving-way and early cartilage wear.
(Sources: Miller's Review of Orthopaedics 9th Ed.; Campbell's Operative Orthopaedics 15th Ed. 2026)
IV. Posterior Femoral Rollback
As the knee flexes, the femoral condyles roll posteriorly on the tibial plateau:
- This moves the tibiofemoral contact point posteriorly
- It is essential for achieving maximum knee flexion (>120°) - without rollback, the posterior femoral cortex would impinge on the tibial plateau
- The PCL is the primary restraint driving rollback; PCL sacrifice in total knee arthroplasty (cruciate-sacrificing TKA) impairs this mechanism and limits flexion
- The lateral condyle rolls back more than the medial condyle (consistent with the four-bar model)
V. Tibiofemoral Joint Kinetics (Forces)
Joint Reaction Forces
The tibiofemoral joint experiences forces well above body weight:
| Activity | Approximate Joint Force |
|---|---|
| Level walking | 3 × body weight |
| Stair climbing | 4 × body weight |
| Jogging | 4-5 × body weight |
| Deep squat | 7-8 × body weight |
These forces are primarily compressive, directed along the mechanical axis.
Load Distribution
The load is not uniformly distributed across the joint:
- The medial compartment bears approximately 60-70% of the total tibiofemoral load, explaining the higher prevalence of medial compartment OA
- The lateral compartment bears 30-40%
- The menisci transmit 50-75% of axial load in full extension and up to 85% at 90° of flexion
- Medial meniscus bears 30-40% of tibiofemoral load; lateral meniscus bears ~70%
- Total meniscectomy increases peak contact stresses up to 4 times above normal
- Resection of just 75% of the radial meniscal width produces contact stress increases equivalent to complete meniscectomy
(Source: Miller's Review of Orthopaedics, 9th Ed.)
VI. Patellofemoral Biomechanics
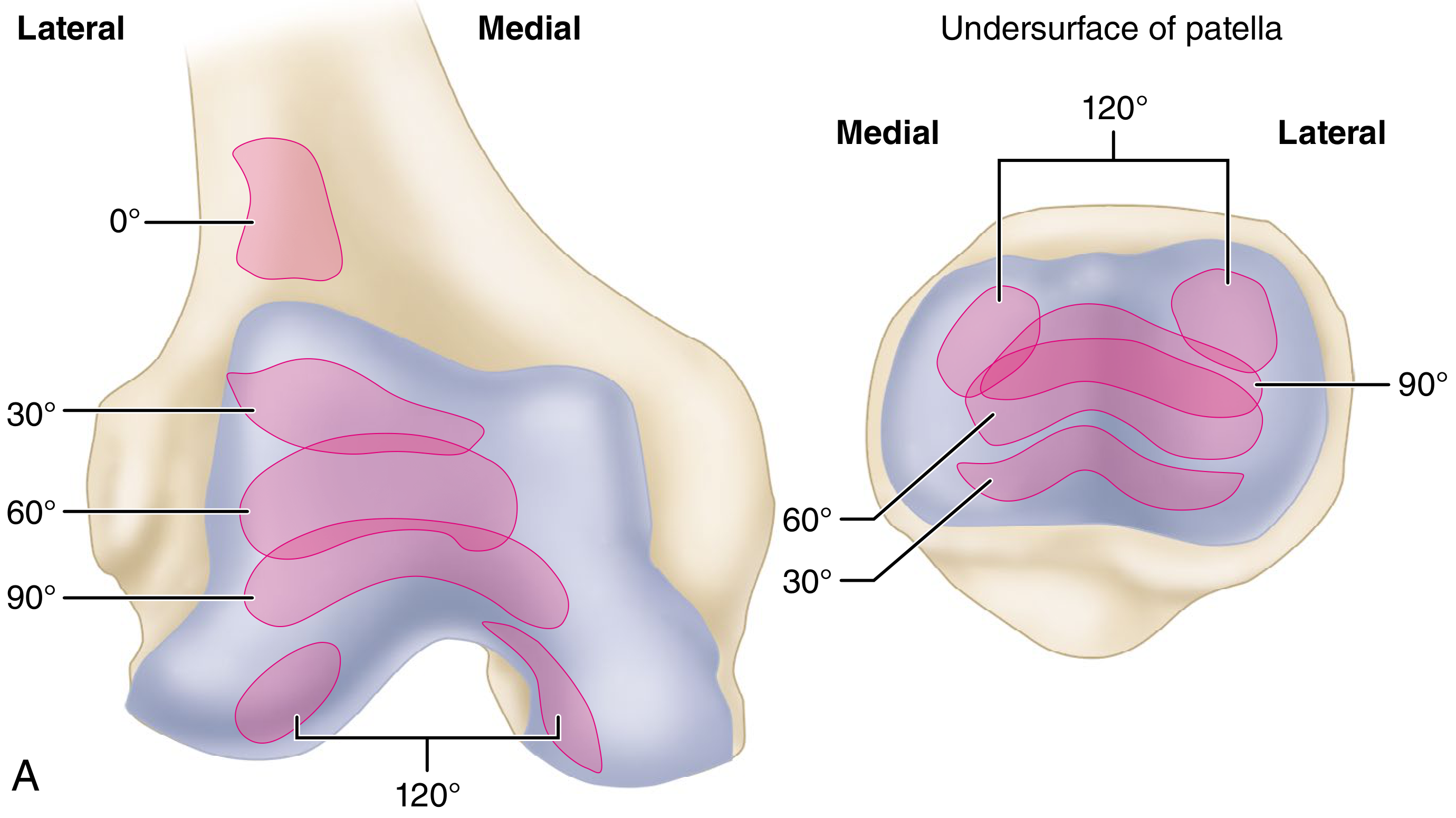
Patellofemoral contact patterns at various flexion angles (Campbell's Operative Orthopaedics, 15th Ed. 2026)
Role of the Patella
The patella is a sesamoid bone embedded in the quadriceps tendon. Its primary biomechanical functions are:
- Lever arm enhancement: Acts as a pulley that increases the mechanical advantage (moment arm) of the quadriceps by approximately 1.5-2 cm (~30%). Patellectomy decreases the power of knee extension by 30%.
- Force direction: Redirects the vector of quadriceps force from an oblique to a more vertical direction relative to the knee
- Centralising quadriceps force: Unifies the pull of the four quadriceps heads into a single vector
Patellofemoral Joint Reaction Force (PFJRF)
As the quadriceps contracts, the patellar tendon and quadriceps tendon exert tension on the patella from two directions. The patella is pushed posteriorly against the trochlear groove, generating a compressive PFJRF. This force:
- Increases with knee flexion (force vectors of quadriceps and patellar tendons become more parallel)
- Increases with quadriceps contraction force
| Activity | Approximate PFJRF |
|---|---|
| Level walking | 0.5 × BW |
| Normal walking | 1-2 × BW |
| Stair descent | 2-3 × BW |
| Squatting (up to 120° flexion) | 7-8 × BW |
| Jumping | Up to 20 × BW |
(Sources: Bailey & Love's Short Practice of Surgery, 28th Ed.; Miller's Review of Orthopaedics, 9th Ed.; Campbell's Operative Orthopaedics, 15th Ed.)
Contact Area Progression with Flexion
The area of patellar contact on the trochlea changes with flexion angle:
- 0-10°: No significant contact (patella is above the trochlea)
- ~20°: Inferior patellar surface first contacts the trochlea
- ~60°: Midportion of patella contacts trochlea
- ~90°: Superior portion contacts trochlea
- >120°: Contact shifts to medial and lateral peripheral facets only; quadriceps tendon itself contacts the trochlear groove
- A third ("odd") medial facet articulates with the medial femoral condyle at >90°
This progressive shift distributes compressive stress over a larger area with increasing flexion - a protective mechanism. The patella has the thickest articular cartilage in the body, consistent with the high forces it bears.
Q-Angle
The Q-angle (angle between quadriceps pull and patellar tendon) is normally:
- Males: ~10-12°
- Females: ~15-18°
An increased Q-angle generates a greater lateral patellar pull (valgus vector), predisposing to patellar subluxation, maltracking, and patellofemoral pain syndrome. This contributes to the higher incidence of patellofemoral problems in females.
VII. Ligament Biomechanics
Structural Properties (Tensile Strength)
| Ligament | Approximate Tensile Strength |
|---|---|
| ACL | ~2200 N (up to 2500 N in young individuals) |
| PCL | ~2500-3000 N |
| LCL | ~750 N |
| Superficial MCL | ~550 N |
| Deep MCL | ~100 N |
| POL | ~250 N |
(Source: Miller's Review of Orthopaedics, 9th Ed.)
ACL during normal walking: peak load ~170 N; with running: ~500 N.
Functional Roles
Ligaments provide passive restraints against abnormal motion:
| Direction | Primary Restraint | Secondary Restraints |
|---|---|---|
| Anterior tibial translation | ACL | Joint capsule |
| Posterior tibial translation | PCL (89% of resistance) | Meniscofemoral ligaments |
| Medial stability (valgus) | Superficial MCL | Capsule, medial meniscus, ACL/PCL |
| Lateral stability (varus) | LCL | Capsule, IT band, lateral meniscus |
| Internal rotation | ACL | - |
| External rotation | MCL | ACL/PCL |
Cruciate Ligament Kinematics
The ACL has two bundles:
- Anteromedial (AM) bundle: tight in flexion; primarily resists anterior tibial translation
- Posterolateral (PL) bundle: tight in extension; controls rotation
The PCL is more vertically oriented than the ACL and is the axis around which knee rotation occurs. It:
- Resists 89% of posterior tibial translation
- Guides the screw-home mechanism
- Restrains external, internal, and varus-valgus rotation
- Lengthens with progressive knee flexion
As the knee flexes, ligaments anterior to the flexion axis stretch and ligaments posterior to it shorten - a critical principle for reconstructed ligament placement (isometry).
VIII. Meniscal Biomechanics
The menisci (medial and lateral) are C-shaped fibrocartilaginous structures with circumferentially oriented collagen fibres. Their functions include:
- Load transmission and shock absorption: Transmit 50-75% of axial loads in extension, 85% at 90° flexion. They reduce peak contact stresses by 100-200% compared to a meniscectomised knee.
- Congruency enhancement: Deepen the tibial plateaux, improving joint congruency with the convex femoral condyles
- Secondary stabilisation: The posterior horn of the medial meniscus is a major secondary stabiliser against anterior tibial translation in the ACL-deficient knee - explaining why medial meniscus tears accelerate instability episodes
- Proprioception: Contain mechanoreceptors that contribute to neuromuscular feedback
- Lubrication: Help distribute synovial fluid across the joint surface
Key differences between medial and lateral meniscus:
- The lateral meniscus has twice the excursion of the medial meniscus during knee flexion (1.1 cm vs. 0.5 cm over a 120° arc)
- The lateral meniscus bears ~70% of the lateral compartment load; medial meniscus bears 30-40% of medial compartment load
IX. Muscle Forces Around the Knee
Quadriceps
- The dominant extensor mechanism
- At 0-60° of knee flexion, quadriceps contraction produces maximum anterior shear force on the tibia (high ACL load zone)
- This is why closed kinetic chain exercises are preferred in ACL rehabilitation (they co-activate the hamstrings, reducing net anterior tibial shear)
- During deep flexion (60-90°), the posterior shear increases (PCL load zone)
Hamstrings
- Primary dynamic restraints against anterior tibial translation (ACL synergists)
- Co-contracted with quadriceps during functional activities for joint protection
Popliteus
- Initiates flexion by internally rotating the tibia (unlocking the screw-home mechanism)
- Acts as a posterolateral stabiliser, important in preventing posterior lateral corner injury
Iliotibial Band (IT Band)
- Lateral stabiliser
- Contributes to knee extension at <30° of flexion (extensor), but becomes a flexor beyond 30°
- Important in running biomechanics; tightness causes IT band friction syndrome
X. Closed vs. Open Kinetic Chain Biomechanics
| Parameter | Open Kinetic Chain (OKC) | Closed Kinetic Chain (CKC) |
|---|---|---|
| Distal segment | Free to move | Fixed (foot on ground) |
| Example | Terminal knee extension, leg press | Squats, lunges, step-ups |
| Tibiofemoral shear | High anterior shear (0-60°) | Reduced anterior shear |
| Patellofemoral force | Lower at low flexion | Increases with flexion |
| ACL load | Higher (0-60° flexion) | Lower overall |
| Clinical use | Late-stage ACL rehab | Early-stage ACL rehab |
CKC exercises are preferred in early rehabilitation as they reduce anterior tibial shear force on the ACL while increasing joint compressive forces (improving stability).
XI. Valgus-Varus Alignment and Clinical Implications
- Genu valgum (knock knees): increases lateral compartment loading, predisposes to lateral patella subluxation, IT band syndrome
- Genu varum (bow legs): shifts load medially, strongly associated with medial compartment OA (medial tibiofemoral load increases significantly with varus deformity)
- High tibial osteotomy (HTO): corrects the mechanical axis to redistribute load away from the diseased medial compartment - directly applying these biomechanical principles
Summary Table: Key Numbers to Remember
| Parameter | Value |
|---|---|
| Tibiofemoral force - walking | 3 × BW |
| Tibiofemoral force - stairs | 4 × BW |
| PFJRF - walking | ~0.5 × BW |
| PFJRF - squatting | 7-8 × BW |
| PFJRF - jumping | Up to 20 × BW |
| Meniscal load transmission at 90° | 85% of axial load |
| Increase in contact stress after total meniscectomy | Up to 4 × |
| Screw-home rotation | 5-10° external tibial rotation |
| Patella slide during full flexion | ~7 cm caudally |
| Patellectomy - loss of extension power | ~30% |
| ACL tensile strength (young) | ~2200-2500 N |
| PCL tensile strength | ~2500-3000 N |
References
- Miller's Review of Orthopaedics, 9th Edition - Knee Biomechanics (Ligament Biomechanics, Kinematics, Meniscal Biomechanics, Kinetics)
- Campbell's Operative Orthopaedics, 15th Edition (2026) - Patellofemoral Joint Biomechanics and Functional Anatomy; PCL Biomechanics
- Bailey and Love's Short Practice of Surgery, 28th Edition - Biomechanics of the Knee Joint
- Rockwood and Green's Fractures in Adults, 10th Edition (2025) - ACL Function and Biomechanics
explain me in simple language
Here's the entire biomechanics of the knee explained in plain, simple language - like a story.
The Knee Joint - Made Simple 🦵
1. What kind of joint is the knee?
Most people think the knee is just a simple hinge - like a door. But it's much smarter than that.
When you bend and straighten your knee, three things happen at the same time:
- Rolling - like a ball rolling on the floor
- Sliding - like a ball that also skids backward to stay in place
- Rotating - like a slight twist at the end
Why both rolling AND sliding? Because if the thigh bone (femur) only rolled on the shin bone (tibia), it would literally roll off the back of the knee by the time you reach full bend. So sliding backward compensates - keeping everything in contact. Smart engineering.
2. The "Screw-Home" Mechanism - The Knee's Locking System
Think of this like a door latch.
When you fully straighten your knee, the tibia (shin bone) automatically twists outward by about 5-10 degrees. This locks the knee into a stable, rigid position - like screwing a bolt tight.
This is called the "screw-home" mechanism.
Why does this happen?
The two knuckles at the bottom of the thigh bone (femoral condyles) are different sizes. The inner one is bigger. So as you near full extension, the outer condyle finishes its movement first, forcing the shin to rotate outward as the inner one catches up.
To unlock the knee (start bending from a straight position), a small muscle at the back of the knee called the popliteus rotates the shin inward by about 5° - like turning a key to open a lock. That's literally what textbooks call it: "the key to the knee."
3. Posterior Rollback - How You Can Bend Deeply
As you bend your knee deeper, the thigh bone rolls backward on the shin bone. This is called posterior rollback.
Without this rollback, the back of your thigh bone would crash into the back of your shin bone around 90° of bend, and you could never squat or sit cross-legged.
The ligament that controls this rollback is the PCL (posterior cruciate ligament). If surgeons cut the PCL during a knee replacement, the knee can't roll back properly, so deep bending becomes limited.
4. How Much Load Does the Knee Handle?
This is where things get impressive. Your knee handles forces much greater than your body weight:
| What you're doing | Force on knee |
|---|---|
| Just standing | ~1 × your body weight |
| Walking on flat ground | 3 × body weight |
| Climbing stairs | 4 × body weight |
| Squatting deep | 7-8 × body weight |
| Jumping and landing | Up to 20 × body weight |
So if you weigh 70 kg, your knee handles up to 1400 kg during jumping. That's why the knee has thick cartilage and special shock absorbers (menisci).
5. The Menisci - The Knee's Shock Absorbers
The menisci are two C-shaped rubbery pads (one on inner side, one on outer side) sitting between the thigh bone and shin bone. Think of them as cushions or gaskets.
What do they do?
- They carry 50-75% of the load going through your knee when walking
- At 90° of bending (like sitting on a chair), they carry 85% of the load
- They also fill in the gap between the round femoral condyles and the flatter tibial plateau, making the surfaces fit better (like putting a washer on a bolt)
What happens if they're removed?
Contact stress on the cartilage goes up 4 times. This is why surgeons try to save or repair menisci rather than remove them - even removing a large chunk causes almost as much damage as removing the whole thing.
Bonus role of the medial meniscus: When your ACL (the main stabilising ligament) is torn, the inner meniscus steps up and acts as a secondary brake against the shin bone sliding forward. This is why people with ACL tears often tear their medial meniscus too - it gets overworked.
6. The Patella - The Knee's Pulley System
The kneecap (patella) is like a pulley on a crane.
When your quadriceps (thigh) muscle contracts to straighten your knee, the force travels down through the kneecap. Without the kneecap, the pull would be at a bad angle. The kneecap redirects and amplifies the force - increasing the mechanical advantage by about 30%.
Remove the kneecap (patellectomy)? You lose 30% of your extension strength. That's like suddenly having one-third less power in your thigh.
Force on the kneecap:
| Activity | Force on kneecap |
|---|---|
| Walking | ~0.5 × body weight |
| Going down stairs | 2-3 × body weight |
| Deep squatting | 7-8 × body weight |
| Jumping | Up to 20 × body weight |
The kneecap has the thickest cartilage in the entire body - it needs it, because it bears the most force per unit area.
Contact area shifts with bending angle:
- At 0° (straight): no real contact
- At 20°: the bottom of the kneecap first touches the groove
- At 60°: middle of kneecap contacts
- At 90°: top of kneecap contacts
- Beyond 120°: only the edges contact, and the quadriceps tendon itself starts pushing against the groove
This is intelligent design - the contact area keeps moving, so no single spot gets overloaded all the time.
7. The Ligaments - The Ropes Holding Everything Together
Think of ligaments as non-elastic ropes that prevent the bones from moving in the wrong direction.
| Ligament | Job | Strength |
|---|---|---|
| ACL (front cross-rope) | Stops shin bone sliding forward | ~2200 N |
| PCL (back cross-rope) | Stops shin bone sliding backward | ~2500-3000 N |
| MCL (inner side rope) | Stops the knee buckling inward | ~550 N |
| LCL (outer side rope) | Stops the knee buckling outward | ~750 N |
The ACL under normal use:
- Walking: ~170 N of load (well within its strength)
- Running: ~500 N
- Ultimate failure strength: ~2200 N
When you twist suddenly while your foot is planted - like in football or basketball - the ACL can snap. This often happens near its failure strength limit.
The cruciates work together like an X-shaped linkage. As the knee bends, this X-cross makes the thigh bone roll and slide correctly. Cutting either cruciate disturbs this whole system.
8. The Alignment - Why Bow Legs and Knock Knees Matter
Imagine you're loading a bridge. If the load goes through the centre, both sides carry equal weight. If you shift the load to one side, that side gets overloaded and breaks faster.
- Bow legs (varus) = load shifts to the inner (medial) compartment → medial cartilage wears out → medial knee arthritis (the most common type)
- Knock knees (valgus) = load shifts to the outer (lateral) compartment → less common OA pattern
High tibial osteotomy (HTO) - surgeons cut and re-angle the shin bone to shift the load back to the healthier side. Pure applied biomechanics.
9. Open vs. Closed Chain - Why Squats are Better Than Leg Extensions for ACL Rehab
| Leg Extension (Open Chain) | Squat (Closed Chain) | |
|---|---|---|
| Foot | Free in air | Fixed on ground |
| Shin bone movement | Slides forward (pulls ACL) | Stays put |
| ACL stress | HIGH (especially 0-60°) | LOWER |
| Used in | Late rehab | Early rehab |
When the foot is fixed on the ground (closed chain), the hamstrings and other muscles automatically co-activate, protecting the ACL. That is why post-ACL surgery physiotherapy starts with squats and lunges, not leg extension machine exercises.
The Whole Story in 6 Lines
- The knee rolls, slides AND rotates - it's not just a hinge.
- It locks itself straight (screw-home) and needs the popliteus to unlock.
- The femoral condyles roll backward (rollback) to allow deep bending.
- Forces through the knee reach 3-8× body weight in daily activities.
- The menisci absorb 50-85% of load; losing them quadruples cartilage stress.
- The patella amplifies quadriceps force by 30% - remove it and you lose 30% of extension strength.
That covers the entire biomechanics of the knee in a way that actually makes sense. If you want me to go deeper on any one section - like just patellofemoral mechanics, or ligament kinematics, or clinical application to rehab - just ask.
This is a shared conversation. Sign in to Orris to start your own chat.