Define Tone in cns
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Here is a thorough, well-structured answer.
Tone (Muscle Tone) in the CNS
Definition
Muscle tone (tonus) is defined as the resistance of a muscle to passive stretch at rest. It represents the baseline level of tension maintained in skeletal muscles even when no voluntary movement is occurring. Somewhere between the extremes of complete flaccidity (zero resistance) and spasticity (exaggerated resistance) lies the ill-defined zone of normal tone.
"The resistance of a muscle to stretch is often referred to as its tone or tonus."
- Ganong's Review of Medical Physiology, 26th Ed.
Neural Basis of Tone - The Key Components
Tone depends on the integrity of a reflex arc involving:
| Component | Role |
|---|---|
| Alpha (α) motor neurons | Large anterior horn cells - innervate extrafusal muscle fibers; their discharge produces actual contraction |
| Gamma (γ) motor neurons | Smaller anterior horn cells - innervate intrafusal fibers of the muscle spindle; tonically active at rest, keeping spindles taut and sensitive |
| Muscle spindles | Sensory receptors within muscle; detect changes in muscle length |
| Ia afferent fibers | Carry stretch signals from spindles to α motor neurons (monosynaptic arc) |
| Golgi tendon organs (GTOs) | Detect tension - mediate the inverse stretch reflex to prevent overstretching |
| Descending supraspinal pathways | Modulate the α and γ motor neurons from above |
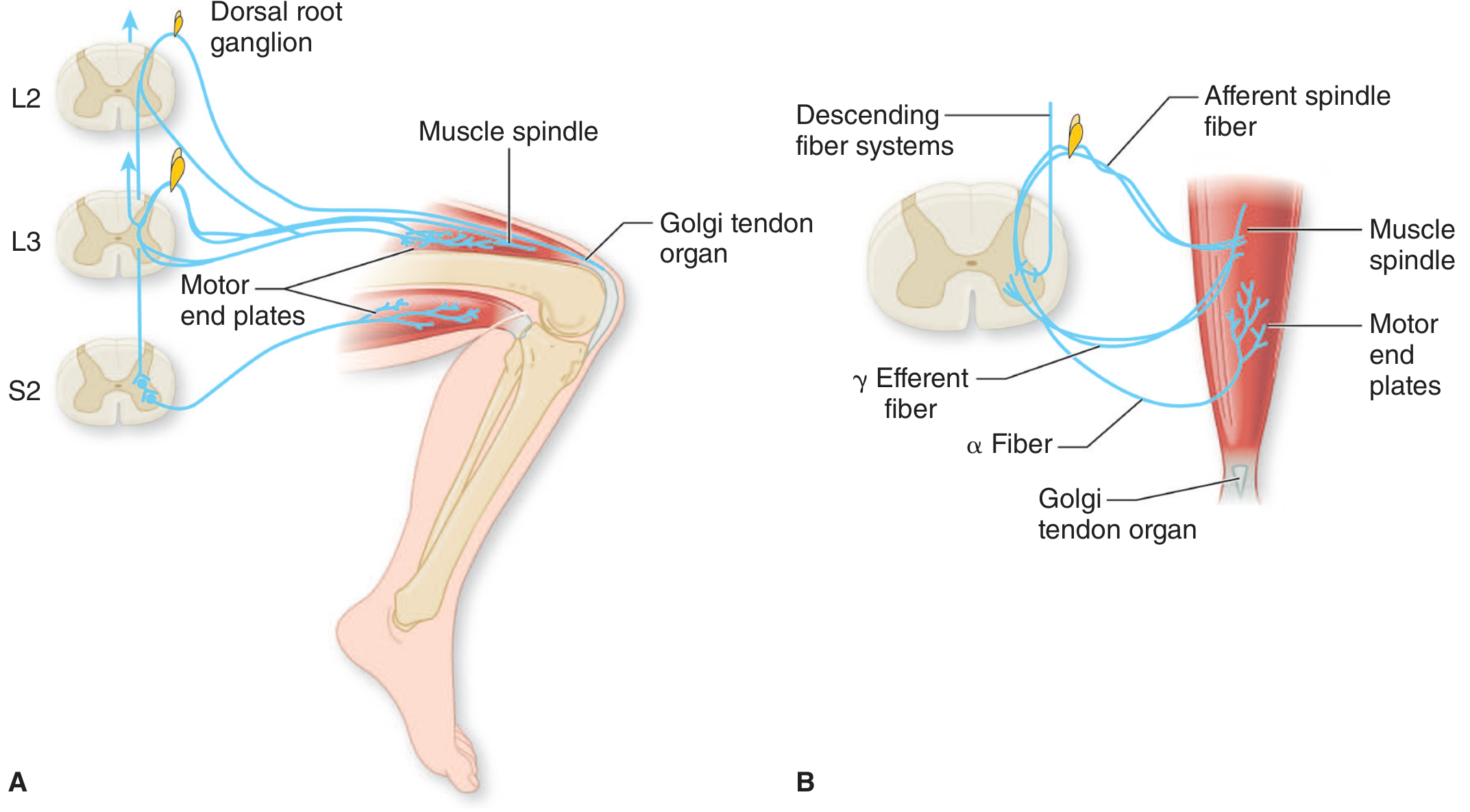
The stretch reflex arc. (A) Patellar reflex; (B) γ efferent fibers maintain spindle sensitivity via intrafusal muscle fibers. - Adams & Victor's Principles of Neurology, 12th Ed.
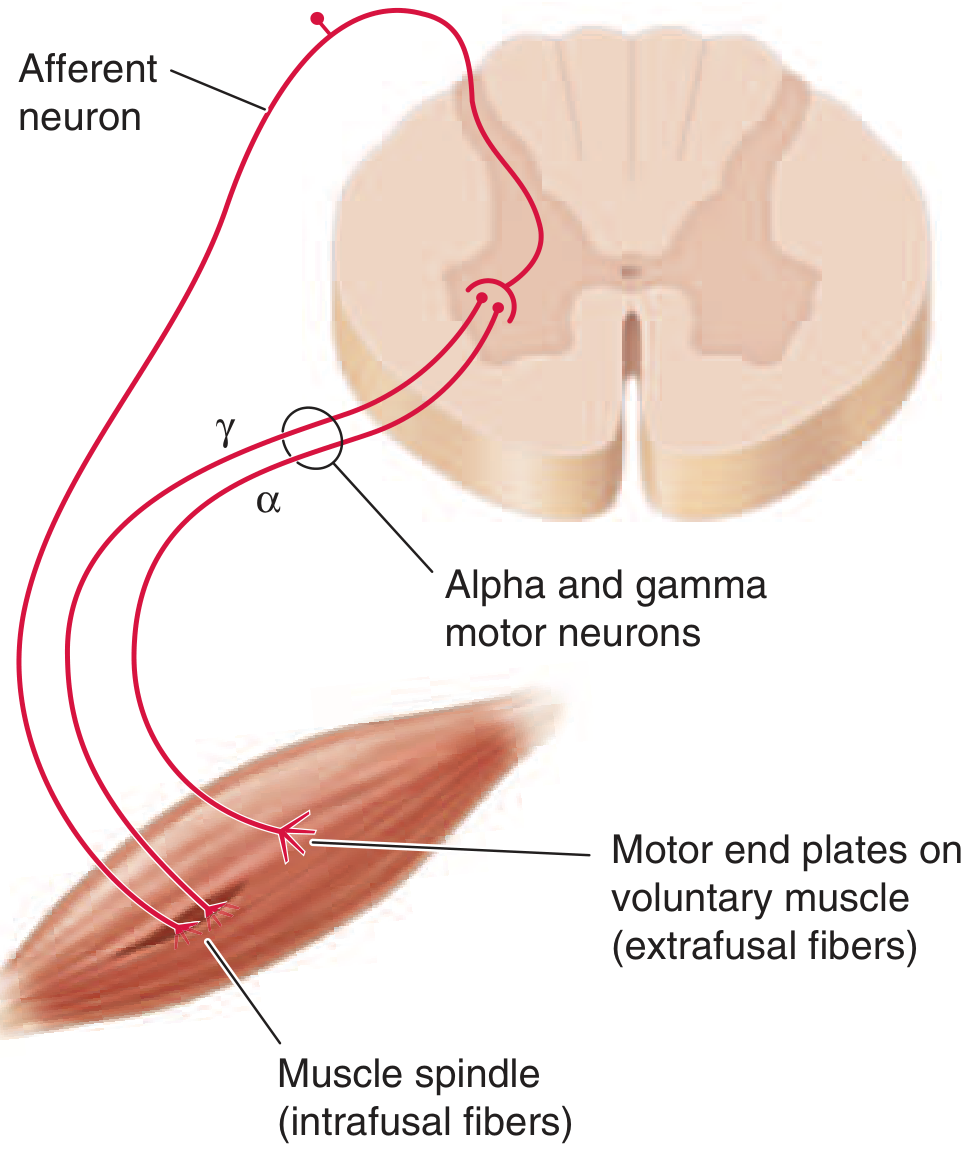
α motor neurons innervate extrafusal fibers; γ motor neurons innervate intrafusal (spindle) fibers. Together they regulate tone and stretch reflexes. - Harrison's Principles of Internal Medicine, 22nd Ed.
Mechanism of Normal Tone
- γ motor neurons fire tonically at rest, keeping the intrafusal fibers of muscle spindles under continuous mild tension.
- This tonic stretch keeps the spindle Ia afferents active, delivering a low-level excitatory drive to α motor neurons.
- α motor neurons respond with a low level of efferent firing, maintaining background muscle contraction - this is tone.
- Descending supraspinal pathways (corticospinal, reticulospinal, vestibulospinal, rubrospinal) continuously modulate this loop from above.
"Some gamma motor neurons are tonically active at rest, keeping the intrafusal muscle fibers taut and more sensitive to active and passive changes in muscle length."
- Adams & Victor's Principles of Neurology, 12th Ed.
CNS Control - Supraspinal Influences on Tone
| Pathway | Effect on Tone |
|---|---|
| Corticospinal (pyramidal) | Facilitatory to distal muscles; lesion causes initial hypotonia followed by spasticity |
| Reticulospinal | Medullary reticulospinal - inhibitory; Pontine reticulospinal - facilitatory (to extensors) |
| Vestibulospinal | Strongly facilitatory - excites extensor (antigravity) tone |
| Rubrospinal | Facilitatory to flexors of distal limbs |
| Basal ganglia | Modulate tone via thalamo-cortical loop; lesions cause rigidity |
| Cerebellum | Facilitates γ motor neuron activity; lesions cause hypotonia |
"Bulbospinal upper motor neurons influence strength and tone but are not part of the pyramidal system. The descending ventromedial bulbospinal pathways originate in the tectum, vestibular nuclei, and reticular formation and are involved in the maintenance of posture."
- Harrison's Principles of Internal Medicine, 22nd Ed.
Abnormalities of Tone
1. Hypotonia (Decreased Tone)
- Definition: Reduced resistance to passive movement; muscles feel "floppy."
- Causes:
- Lower motor neuron (LMN) lesion: peripheral nerve or anterior horn cell damage
- Posterior column / proprioceptive pathway damage
- Acute upper motor neuron (UMN) lesions - spinal shock phase
- Cerebellar lesions (ipsilateral hypotonia)
- Severe hypotonia allows passive hyperextension of joints.
2. Spasticity (UMN type Hypertonia)
- Definition: Velocity-dependent increase in tonic stretch reflexes with exaggerated tendon jerks.
- Mechanism: Loss of descending inhibitory (mainly reticulospinal) influence on α motor neurons → hyperactive stretch reflex.
- Clasp-knife phenomenon: On rapid passive stretch, there is initial resistance, then sudden release - caused by activation of the inverse stretch reflex (GTOs) and Ib inhibitory interneurons.
- Features: Increased tone with free interval, velocity-dependent, brisk tendon reflexes, Babinski sign.
- Causes: Stroke, spinal cord injury, cerebral palsy, multiple sclerosis.
"Rapid passive displacement of the extremity results in increased resistance followed by relaxation (clasp-knife phenomenon). Resistance varies with the speed and direction of passive motion."
- Bradley & Daroff's Neurology in Clinical Practice
3. Rigidity (Extrapyramidal type Hypertonia)
- Definition: Increased resistance to passive movement that is uniform throughout the range of motion and not velocity-dependent, affecting both flexors and extensors equally.
- Lead-pipe rigidity: Smooth, uniform resistance like bending a lead pipe.
- Cogwheel rigidity: Ratchet-like, rhythmically interrupted resistance - represents tremor superimposed on rigidity (seen in Parkinson's disease).
- Mechanism: Overactivity of the stretch reflex due to loss of basal ganglia inhibition on the thalamo-cortical loop; γ motor neuron hyperactivity.
- Features: No free interval, not velocity-dependent, tendon reflexes NOT enhanced, limb does not resume original position after manipulation.
- Causes: Parkinson's disease, Wilson's disease, neuroleptic drugs, MSA, PSP.
"The increased resistance on passive movement that characterizes rigidity is not preceded by an initial free interval and has an even or uniform quality throughout the range of movement, like bending a lead pipe."
- Adams & Victor's Principles of Neurology, 12th Ed.
4. Paratonia (Gegenhalten)
- The patient appears to actively resist passive movement in any direction.
- Seen in frontal lobe disease, dementia, confusional states.
- Reflects inability to relax, not a true basal ganglia disorder.
Comparison: Spasticity vs. Rigidity
| Feature | Spasticity (UMN) | Rigidity (Extrapyramidal) |
|---|---|---|
| Velocity dependence | Yes (faster = more resistance) | No |
| Distribution | Flexors > extensors (UL); extensors > flexors (LL) | Both flexors and extensors equally |
| Free interval | Yes | No |
| Clasp-knife | Present | Absent |
| Tendon reflexes | Exaggerated | Normal or mildly increased |
| Babinski | Present | Absent |
| Cogwheeling | No | Common (Parkinson's) |
| Lesion site | Corticospinal tract | Basal ganglia / extrapyramidal |
Clinical Examination of Tone
- Inspection: Spontaneous posture - spasticity causes fixed flexed posture of upper limbs.
- Palpation: Hypertonic muscles feel firm; hypotonic muscles feel "doughy."
- Passive movement: Ask the patient to relax completely. Move the limb passively through its full range at varying speeds.
- Normal: uniform, low-level resistance throughout, same at all velocities.
- Spastic: resistance increases with faster movement; clasp-knife release.
- Rigid: even, "lead-pipe" resistance at all velocities.
- Hypotonic: abnormally easy passive movement; joints may hyperextend.
- Heel-dragging test (lower limb): In a supine patient, grasp behind the knee and lift briskly. Normally the heel stays in contact with the table; in spasticity the heel rises off the table.
Summary
Tone in the CNS is the background resistance of muscle to stretch, arising from tonic activity of γ motor neurons maintaining spindle sensitivity, feeding back through Ia afferents onto α motor neurons, all under continuous modulation by supraspinal pathways. When CNS pathways are disrupted, tone becomes either excessively increased (spasticity from corticospinal lesions, or rigidity from extrapyramidal lesions) or decreased (hypotonia from cerebellar, acute UMN, or LMN lesions).
Sources: Adams & Victor's Principles of Neurology, 12th Ed. | Ganong's Review of Medical Physiology, 26th Ed. | Bradley & Daroff's Neurology in Clinical Practice | Harrison's Principles of Internal Medicine, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.