Placenta previa
Reading File
Finding Sources
Searching PubMed
"placenta previa"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have thorough content from multiple authoritative sources. Let me compile the comprehensive answer.
Placenta Previa
Definition
Placenta previa occurs when the placenta implants over the internal os of the cervix. A low-lying placenta is defined when the placental edge lies within 2 cm of the internal os but does not cover it. The older classification into complete, partial, and marginal subtypes is no longer recommended - current terminology simply distinguishes "placenta previa" (covering the os) from "low-lying placenta" (within 2 cm). If the placental edge is more than 20 mm from the os, it is reported as normal.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
- Grainger & Allison's Diagnostic Radiology, p. 915
Incidence
- Affects ~0.5% of all third-trimester pregnancies
- Diagnosed in ~10% of mid-trimester sonograms
- At least 90% of cases identified as low-lying or previa in early pregnancy resolve by the third trimester - a phenomenon called "placental migration" (trophotropism toward the fundus with regression of the lower portion)
Risk Factors
| Risk Factor | Increased Risk |
|---|---|
| Previous placenta previa | 8x |
| Previous cesarean section | 1.5-15x |
| Maternal age >35 years | 4.7x |
| Maternal age >40 years | 9x |
| Previous suction curettage/abortion | 1.3x |
| Multiparity | 1.1-1.7x |
| Smoking, cocaine use | Increased |
| Assisted reproductive technology | Increased |
The underlying mechanism involves prior endometrial damage and uterine scarring - curettage, surgical insult, or multiple prior pregnancies - predisposing to lower segment implantation. Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
Pathophysiology
Bleeding arises when marginal placental vessels in the lower uterine segment are torn as:
- The lower uterine wall elongates with advancing gestation
- The cervix effaces and dilates in prelabor/labor
- Intercourse or vaginal examination disrupts the cervical-placental junction
Early bleeding episodes tend to be self-limited. Central/complete previa (~20% of cases) carries the highest risk of severe hemorrhage and maternal/fetal exsanguination.
Clinical Features
- Classic presentation: Painless, bright-red vaginal bleeding in the second or third trimester - often sudden and without preceding trauma
- Several small "herald bleeds" may precede major hemorrhage
- In ~20% of cases, mild uterine irritability is present
- In up to 10% of cases, there is no bleeding until labor onset
- NEVER perform digital or speculum vaginal examination until placenta previa is excluded by ultrasound - this can precipitate catastrophic hemorrhage
Rosen's Emergency Medicine, p. 3356
Diagnosis
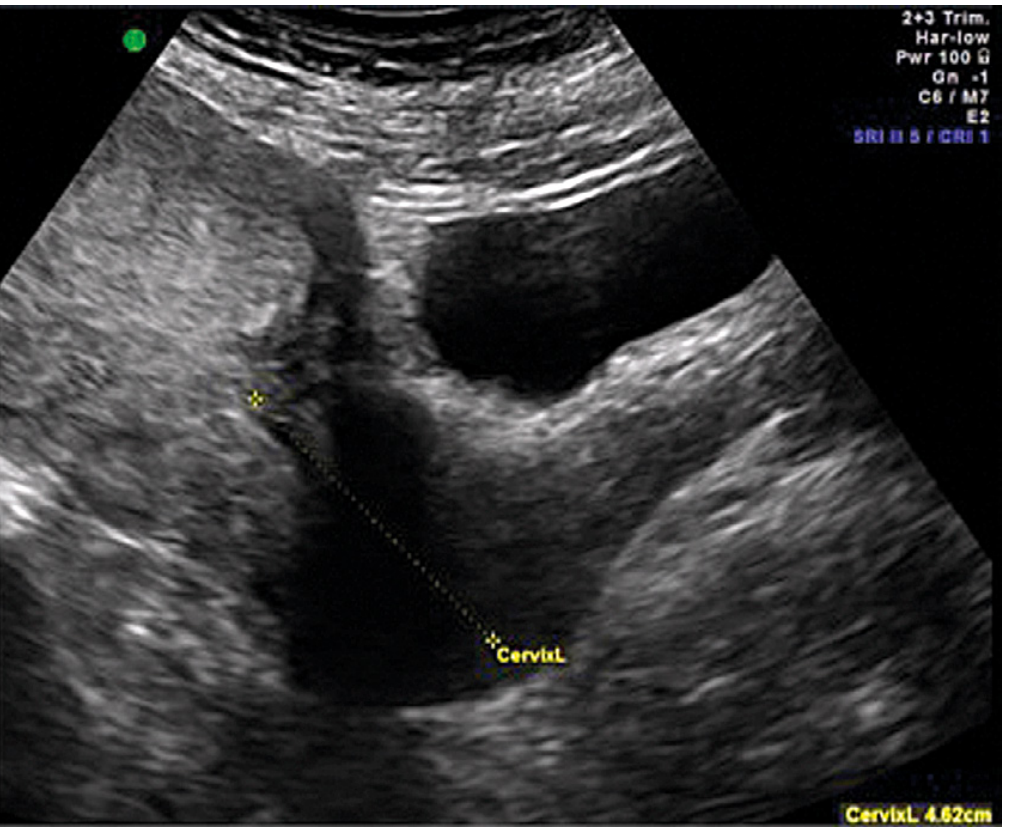
Transvaginal ultrasound (TVUS) is the gold standard:
- Safe, accurate, and provides precise measurement of the placental edge-to-os distance
- The bladder must be emptied first (a full bladder can compress the lower segment and mimic or exaggerate previa)
- Abdominal US at mid-trimester may suggest previa but TVUS is required for definitive diagnosis
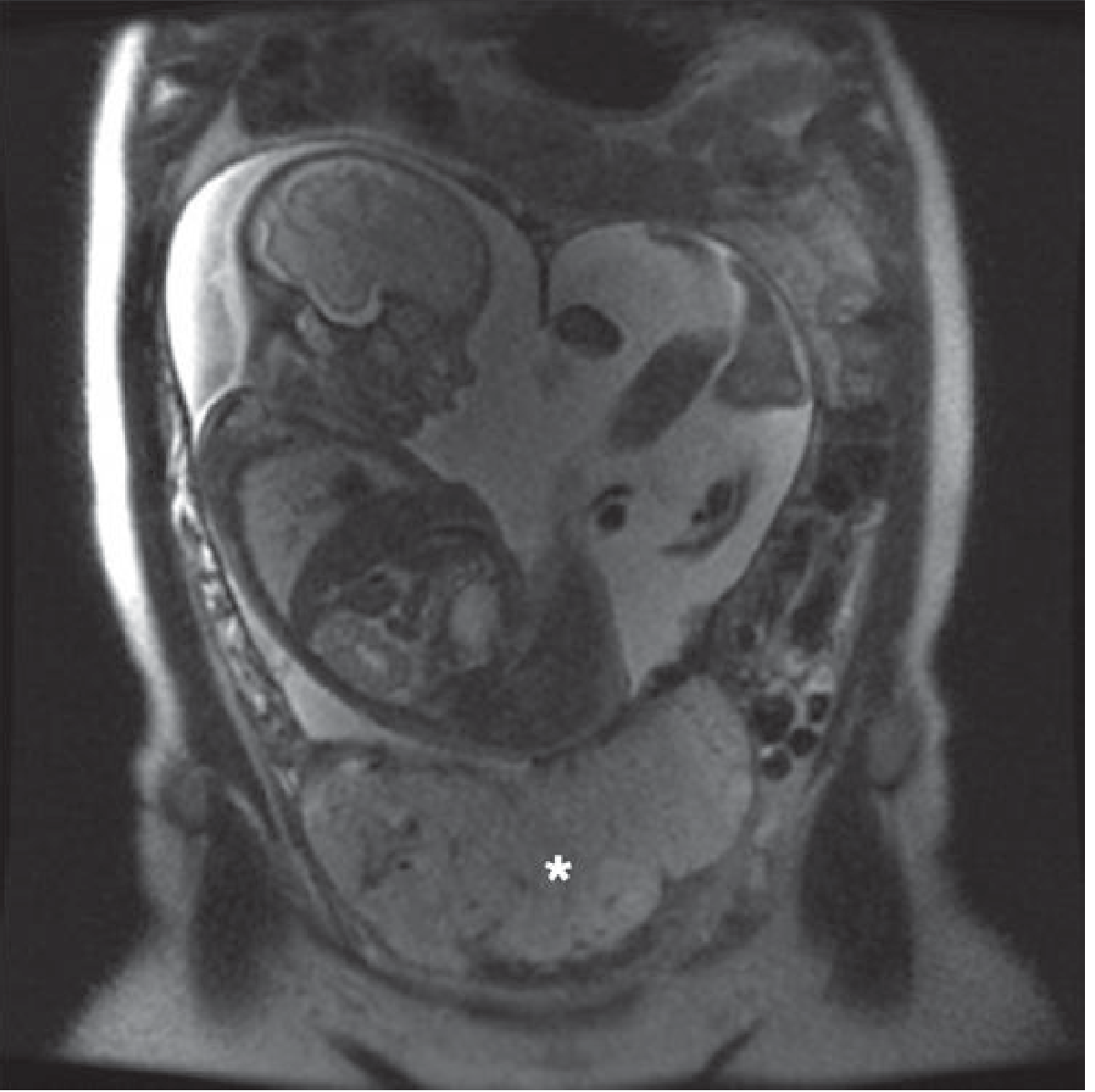
MRI is reserved for equivocal cases or when placenta accreta spectrum (PAS) is suspected.
Differential Diagnosis
- Low-lying placenta (not covering the os)
- Placental abruption (typically painful bleeding, board-like uterus)
- Vasa previa
- Uterine contraction mimicking low-lying placenta
- Succenturiate lobe
- Local cervical/vaginal lesions (hemorrhoids, cervical ectropion)
Associated Conditions
- Placenta accreta spectrum - always screen for this when previa is present, especially with prior cesarean scars
- Vasa previa - umbilical vessels in the membranes overlying the os; risk of fetal exsanguination at membrane rupture
Management
Acute/Emergency (active bleeding)
- Two large-bore IV lines + IV fluid resuscitation
- Labs: CBC, coagulation studies (PT/PTT, fibrinogen, platelets), type and crossmatch
- Normal fibrinogen in pregnancy is 400-450 mg/dL; values below 300 mg/dL indicate significant coagulopathy
- 4 units type-specific or O-negative blood made immediately available; 2 units FFP thawed
- Continuous fetal monitoring
- Rh immune globulin (300 mcg) if Rh-negative and not yet administered
- Obstetric consultation immediately; transfer to appropriate facility if needed
Expectant Management (stable, preterm)
- Hospital admission until bleeding-free for at least 48 hours; then possible outpatient management in carefully selected, stable patients
- Betamethasone for fetal lung maturity if <34 weeks
- Pelvic rest (avoid intercourse, vigorous activity)
- Tocolytics (beta-mimetics or magnesium sulfate) can be used if uterine contractions are present - associated with pregnancy prolongation by ~4 weeks after initial bleed
- Cervical cerclage is NOT recommended (no clear benefit)
- A second significant bleed usually warrants readmission until delivery
Delivery
- Cesarean section is indicated for all women with placenta within 2 cm of the cervical os at term
- A woman whose placenta is more than 2 cm from the os may labor safely
- Delivery should be performed by the most experienced team available given the high risk of intraoperative hemorrhage
- Lower segment transverse incision is standard; if the placenta is anterior, the cord should be clamped immediately after uterine entry; a vertical incision may be preferable in some anterior cases
- Planned delivery at 36-37 weeks is typical for stable previa (risk of hemorrhage vs. prematurity balanced)
Creasy & Resnik's Maternal-Fetal Medicine, p. 1018-1019
Complications
- Antepartum hemorrhage - leading cause
- Postpartum hemorrhage (lower segment atony even without intrapartum bleeding)
- Placenta accreta spectrum (especially with prior uterine scars)
- Preterm birth
- Malpresentation (transverse lie, breech) - placenta occupies the lower segment
- Maternal death (rare in modern obstetrics)
- Perinatal mortality from preterm delivery or fetal exsanguination
Key Clinical Pearls
- Never do a digital vaginal exam in unexplained second/third trimester bleeding until US excludes previa
- TVUS is safe and more accurate than transabdominal US - empty the bladder first
- Most mid-trimester previas resolve - only ~0.5% persist to the third trimester
- Placenta previa + prior cesarean = high risk for placenta accreta - plan delivery at a center with blood bank and surgical expertise
- Low-lying placenta still increases postpartum hemorrhage risk due to lower segment atony
Recent Evidence Note: A 2025 systematic review (PMID 40472373) confirms that postpartum hemorrhage risk is significantly elevated even with low-lying placenta (not just frank previa), supporting active management at delivery. A 2024 meta-analysis (PMID 39305990) found first- and second-trimester aneuploidy screening biomarkers may help predict placenta previa and accreta risk - an emerging area of research.
This is a shared conversation. Sign in to Orris to start your own chat.