Trichomycosis axillaris
Reading File
Finding Sources
Searching PubMed
trichomycosis axillaris
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of trichomycosis axillaris drawn from three dermatology/urology textbooks.
Trichomycosis Axillaris
Synonyms: Trichobacteriosis axillaris, trichomycosis pubis (when pubic hair is involved)
Despite its name, this is not a fungal infection - it is a bacterial condition caused by Corynebacterium species.
Etiology and Pathogenesis
Trichomycosis axillaris is a superficial bacterial infection of axillary and, less frequently, pubic hair shafts, caused by Corynebacterium species (principally C. tenax, a Gram-positive rod). Occasionally, scalp hairs in infants can be affected. Large numbers of corynebacteria form compact concretions that adhere firmly to the hair shaft. Hyperhidrosis is a major predisposing factor, as the warm, moist apocrine-gland-rich environment of the axilla favors bacterial colonization.
Clinical Features
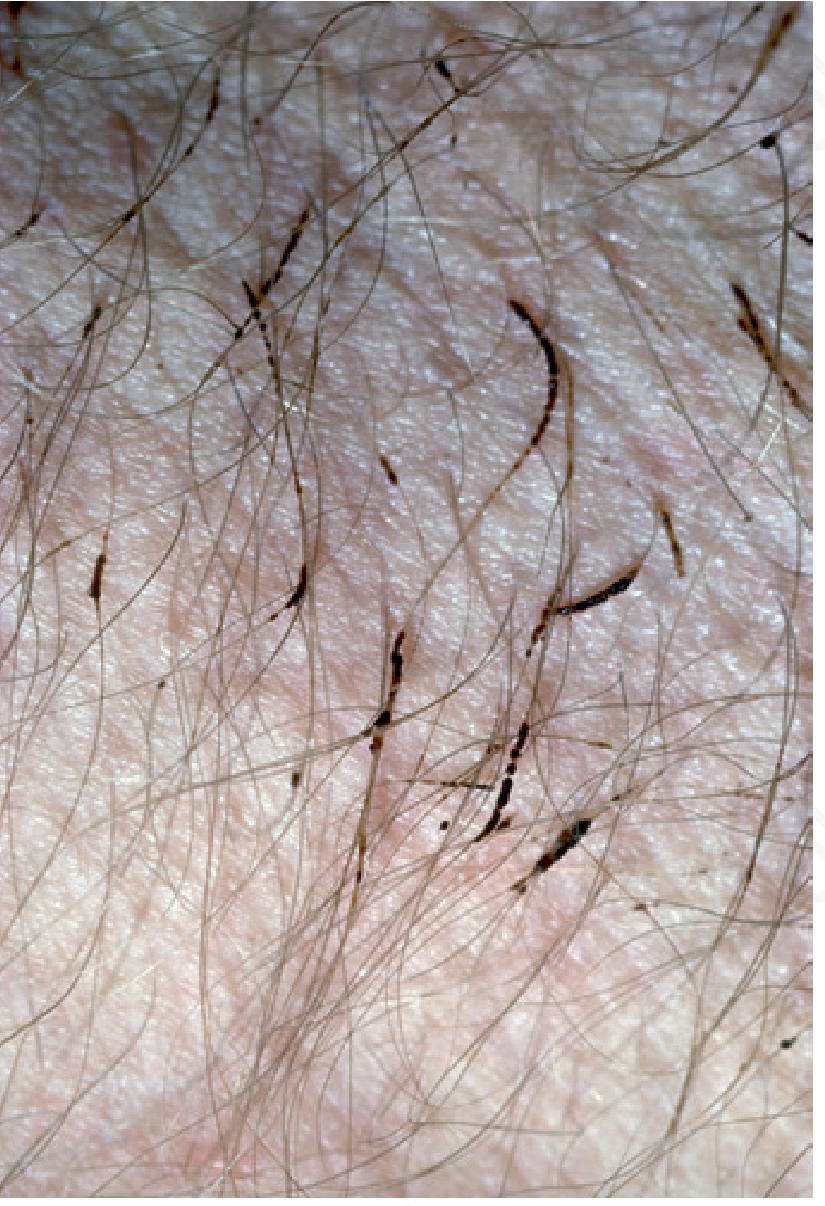
- Hair shaft nodules or cylindrical sheaths - discrete, 1-2 mm concretions firmly attached to the hair shaft, visible to the naked eye
- Color variants: yellow (most common), red, or black - the color corresponds to pigment produced by different Corynebacterium strains
- Characteristic odor - often the presenting complaint; the apocrine sweat is altered by bacterial metabolism
- Chromhidrosis-like staining - sweat may take on a red/yellow color and stain clothing
- Hyperhidrosis of the affected region is almost always present
- Yellowish discoloration of the axillary skin may be noted
- The condition frequently goes unnoticed by the patient
Diagnosis
| Method | Finding |
|---|---|
| Clinical examination | Colored nodules/sheaths on hair shafts |
| Magnification | Distinguishes from pediculosis and piedra |
| Wood's lamp | Pale yellow fluorescence |
| Gram stain of concretions | Gram-positive rods (corynebacteria) |
| KOH | Negative (rules out fungal piedra) |
Differential diagnosis: White piedra (Trichosporon spp.), black piedra (Piedraia hortae), pediculosis pubis (nits/lice), hair casts.
Associated Conditions
Trichomycosis axillaris may coexist with other corynebacterial infections - a "corynebacterial triad":
- Erythrasma (C. minutissimum - coral-red fluorescence on Wood's lamp)
- Pitted keratolysis (plantar surface pitting and odor)
- Trichomycosis axillaris
All three share hyperhidrosis and poor hygiene as risk factors.
Treatment
| Approach | Details |
|---|---|
| Shaving | Fastest and most immediately effective; instant cure by removing the infected hair |
| Topical antibiotics | Clindamycin 1% gel/solution or erythromycin - first-line |
| Benzoyl peroxide | Antibacterial and astringent properties |
| Naftifine | Has both antifungal and antibacterial properties |
| Antibacterial cleansers | Prevent recurrences |
| Hyperhidrosis control | Topical aluminum chloride; addresses underlying predisposing factor |
| Oral erythromycin | 500-1000 mg/day for refractory cases |
The combination of a topical antibiotic plus a modality that decreases hyperhidrosis gives the best sustained results. Shaving alone provides immediate improvement but recurrence is common unless sweating is also addressed.
Key Points Summary
- Despite the name "-mycosis," it is bacterial (corynebacterial), not fungal
- Predisposed by hyperhidrosis and apocrine-rich skin sites
- Yellow > red > black nodular concretions on hair shafts
- Wood's lamp: pale yellow fluorescence (vs. coral-red of erythrasma)
- Treatment: shave + topical clindamycin/erythromycin ± benzoyl peroxide
- Part of the corynebacterial triad with erythrasma and pitted keratolysis
Sources: Andrews' Diseases of the Skin (Clinical Dermatology); Dermatology 2-Volume Set 5e; Campbell-Walsh-Wein Urology
Recent literature (2023-2025) continues to confirm Corynebacterium as the sole causative genus and supports topical antibiotics plus hygiene measures as the standard of care (PMID 37900398 - comprehensive 2023 review; PMID 40125056 - 2025 clinicoetiological study).
This is a shared conversation. Sign in to Orris to start your own chat.