Congenital subglottic stenosis in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
"subglottic stenosis"[MeSH Terms] AND congenital
Reading File
Reading File
Reading File
Searching PubMed
"subglottic stenosis" AND congenital AND laryngotracheal
Reading File
Finding Sources
Reading Article
PMID: 42128760
Reading Article
PMID: 36347385
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
congenital subglottic stenosis RGUHS ENT exam Dhingra Hazarika classification management 2024
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
CONGENITAL SUBGLOTTIC STENOSIS
20-Mark Answer | RGUHS ENT Examination
1. DEFINITION
Subglottic stenosis (SGS) is narrowing of the laryngeal lumen at the level of the subglottis - the space extending from the lower surface of the true vocal cords to the lower border of the cricoid cartilage (the narrowest part of the pediatric airway).
Congenital SGS is defined as:
- A cricoid diameter of < 4 mm in a full-term neonate (normal: 4.5-5.5 mm)
- < 3.5 mm in a premature infant
- Present in an airway with NO prior history of endotracheal intubation, surgery, trauma, or other acquired cause
(Cummings Otolaryngology, Chapter 209; Scott-Brown's Vol 2, Chapter 30)
2. INCIDENCE AND IMPORTANCE
- Third most common congenital laryngeal anomaly, after laryngomalacia (1st) and vocal fold immobility (2nd)
- Constitutes only ~5% of all SGS (the vast majority are acquired)
- True incidence is underestimated because many affected neonates are intubated for respiratory distress at birth, thus technically converting to "acquired" or combined stenosis
- Down syndrome (Trisomy 21) has a high association with congenital SGS (elliptical cricoid)
- 22q11 deletion (DiGeorge syndrome) is associated with anterior glottic webs with subglottic extension
(Cummings, Ch. 209; Scott-Brown Vol 2, Ch. 30; KJ Lee's Essential Otolaryngology)
3. EMBRYOLOGY AND PATHOGENESIS
The subglottis develops from the mesoderm of the 4th and 6th branchial arches, with the cricoid cartilage forming from the 6th arch. Canalization of the laryngeal lumen occurs through dissolution of the epithelial lamina between the 8th and 12th weeks of gestation.
Congenital SGS results from:
- Defective canalization of the cricoid cartilage and/or conus elasticus
- Failure of recanalization of the epithelial plug that temporarily obliterates the laryngeal lumen during the 2nd-3rd month of fetal life
- Associated chromosomal anomalies affecting cartilage development
(Scott-Brown's Vol 2, Ch. 30; Dhingra Diseases of ENT Head & Neck Surgery)
Flowchart 1: Embryological basis
Normal laryngeal development
|
8th-12th week: Epithelial lamina dissolves → normal lumen
|
┌────────┴────────┐
Failure of Cartilage
canalization malformation
| |
Membranous Cartilaginous
type SGS type SGS
4. PATHOLOGICAL CLASSIFICATION
Congenital SGS is divided into two main types:
A. MEMBRANOUS TYPE (Soft / Fibrous)
- Fibrous soft tissue thickening of the subglottic mucosa
- Caused by increased fibrous connective tissue or hyperplastic dilated mucous glands without inflammatory reaction
- Usually circumferential, narrowest area 2-3 mm below the true vocal cords
- May extend upward to involve the true vocal cords
- Better prognosis; may respond to endoscopic treatment
B. CARTILAGINOUS TYPE (Hard / Structural)
More variable; subtypes include:
- Thickened/deformed cricoid - a shelf-like plate of cartilage partially filling the concave inner surface of the cricoid, extending posteriorly as a solid rigid sheet, leaving only a small posterior opening (most common)
- Elliptical/small cricoid - narrow transverse diameter (seen in Trisomy 21); small anteroposterior diameter
- Trapped first tracheal ring - may produce anterior subglottic shelf and lateral narrowing; clinically variable
- Anterior cricoid thickening - gross thickening of the anterior cricoid lamina
Key point (Scott-Brown): Cartilaginous congenital SGS is a strict contraindication to dilatation or laser resection - attempted dilatation inevitably worsens the condition as the thickened ring cannot be expanded.
(Cummings Ch. 209; Scott-Brown Vol 2 Ch. 30)
Figure 1 - Endoscopic photograph: Congenital SGS with anterior cricoid thickening (Scott-Brown's)

Figure 30.4 - Congenital SGS showing anterior cricoid thickening (Scott-Brown's Vol 2)
Figure 2 - Endoscopic photograph: Congenital SGS with elliptical thickened cricoid
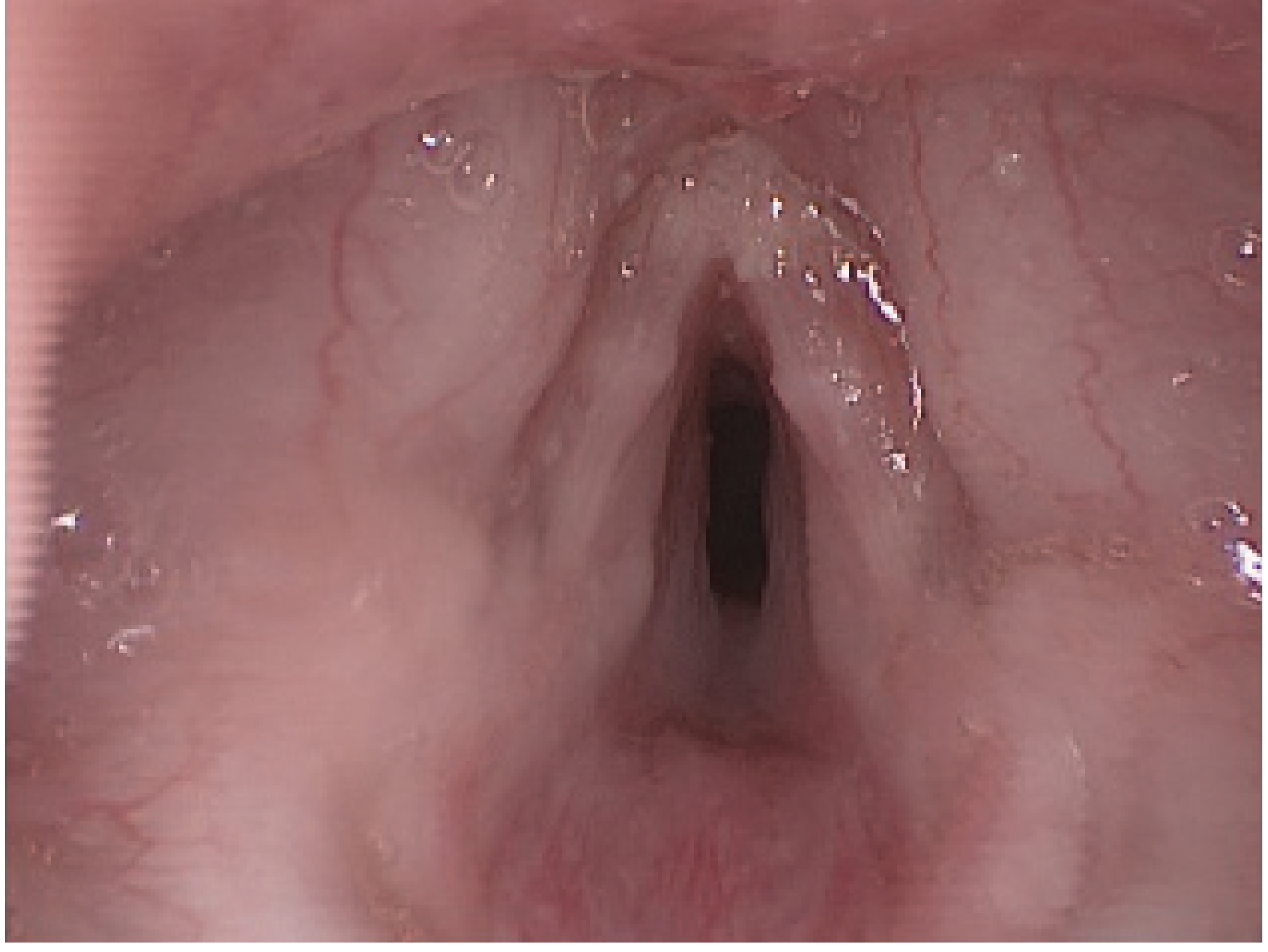
Figure 30.5 - Congenital SGS showing small elliptical thickened cricoid with excessive submucosal soft tissue (Scott-Brown's Vol 2)
5. CLINICAL FEATURES
Symptoms depend on the degree of narrowing and may be present at birth or emerge in the first weeks/months:
Severe stenosis (Grade III-IV):
- Respiratory distress at birth - cyanosis, use of accessory muscles
- Biphasic stridor (both inspiratory and expiratory) - due to fixed narrowing
- Requires immediate airway intervention
Mild to moderate stenosis (Grade I-II):
- Inspiratory stridor emerging weeks to months after birth (increased activity, higher ventilatory needs)
- Recurrent "croup" (recurrent laryngotracheobronchitis) - caused by superimposed mucosal edema from URTIs in an already narrow airway
- Child may be symptom-free between episodes
- Key clinical pearl (Dhingra/Hazarika): Recurrent or atypical "croup" in an infant under 3 months should raise suspicion for underlying SGS
- Infants usually become symptomatic within 3 months of birth due to increased activity and greater ventilation requirements
- Feeding difficulties, failure to thrive (in severe cases)
Flowchart 2: Clinical Presentation by Severity
Congenital SGS
|
┌────┴─────────┐
Severe Mild-Moderate
(Grade III-IV) (Grade I-II)
| |
Stridor at Stridor with activity
birth or URTI ("recurrent croup")
Cyanosis Well between episodes
Resp distress Symptoms emerge 1-3 months
| |
Immediate Watchful waiting
intervention + symptomatic Rx
6. DIAGNOSIS
A. History
- Onset, severity, progression of stridor
- Episodes of "croup" or respiratory distress
- Birth history - gestational age, intubation history (absence required for congenital SGS diagnosis)
- Family history, syndromic features (Down syndrome, 22q11)
B. Physical Examination
- Biphasic stridor (fixed obstruction)
- Subcostal/intercostal retractions
- Cyanosis in severe cases
- Presence of other syndromic features
C. Investigations
1. Plain X-ray neck/chest (soft tissue lateral):
- Subglottic narrowing on AP view ("steeple sign")
- Useful initial screening
2. Flexible fibreoptic laryngoscopy (FFL):
- Office-based assessment
- Assess vocal cord mobility, supraglottic anatomy, dynamic collapse
- Does NOT adequately visualize the subglottis
3. Microlaryngoscopy and Bronchoscopy (MLB) - GOLD STANDARD
- Under general anesthesia
- Exact location of stenosis measured relative to vocal cords, tracheostome, and carina
- Normal tracheal rings above tracheostome are counted
- Passing endotracheal tubes of known sizes to size the stricture (Myer-Cotton grading)
- Assessment of vocal cord mobility
- Identifies associated anomalies (laryngeal clefts, tracheomalacia)
4. CT scan of the neck:
- Assess cartilaginous integrity
- Multi-level disease, associated anomalies
- Virtual bronchoscopy
5. Pulmonary Function Tests (if applicable):
- Flow-volume loops show characteristic flattening of inspiratory limb in fixed upper airway obstruction
(Cummings Ch. 209; Scott-Brown Vol 2 Ch. 30; Scott-Brown Adult Vol, Ch. 76)
7. GRADING - THE MYER-COTTON CLASSIFICATION
The Myer-Cotton grading system (1994) is the most widely used staging system for pediatric SGS. It grades stenosis based on the percentage of cross-sectional area obstruction, determined by comparing the largest endotracheal tube that passes the stenosis with the expected tube for the patient's age.
| Grade | Obstruction | Description |
|---|---|---|
| Grade I | 0-50% | Mild obstruction |
| Grade II | 51-70% | Moderate obstruction |
| Grade III | 71-99% | Severe obstruction (identifiable but markedly reduced lumen) |
| Grade IV | 100% (no detectable lumen) | Complete obstruction |
Figure 3 - Myer-Cotton Grading System (Diagrammatic)
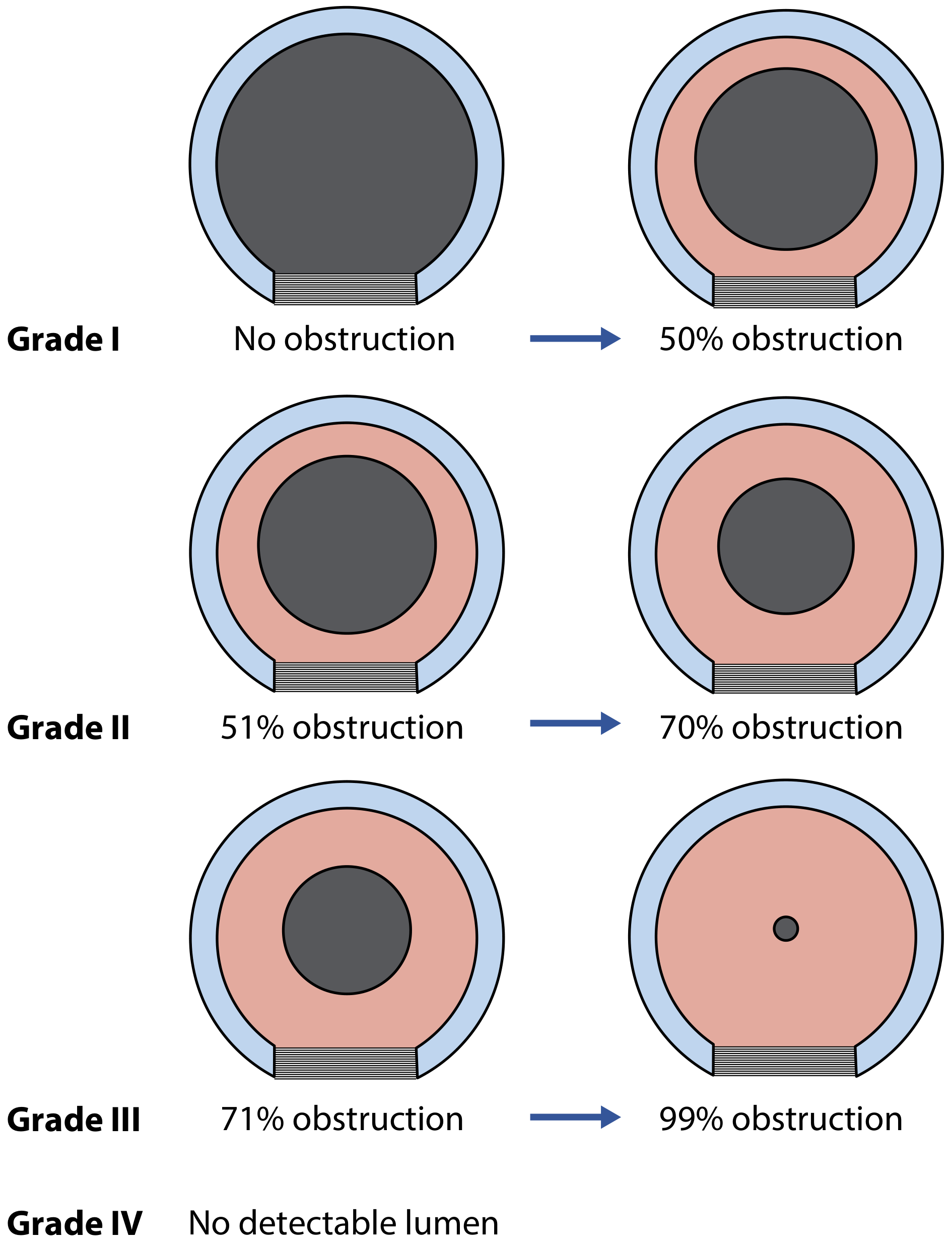
Figure 76.2 - Myer-Cotton grading system for subglottic stenosis (Scott-Brown's Adult Vol, Ch. 76)
Figure 4 - Endoscopic appearances of each Myer-Cotton grade
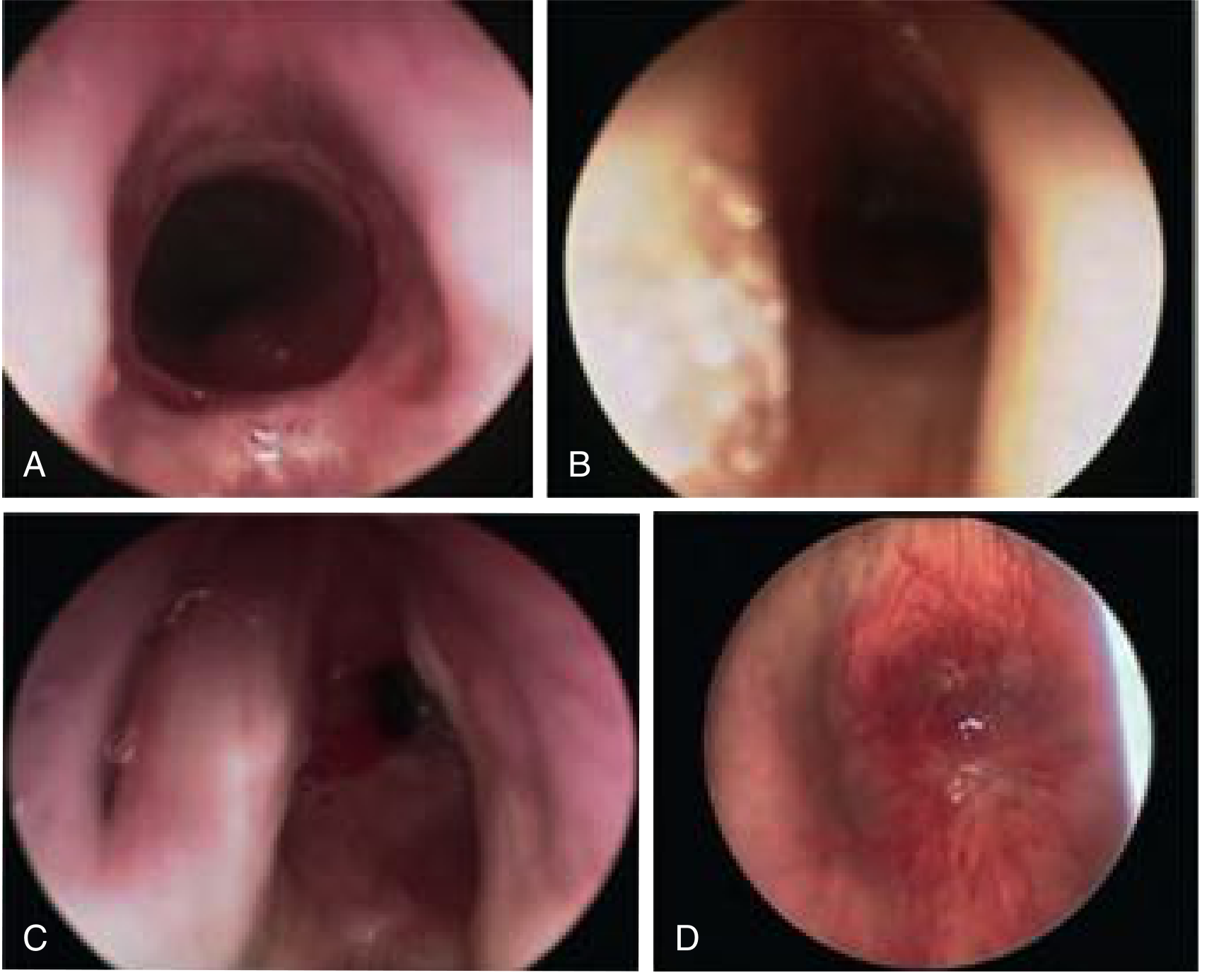
Fig. 209.6 - Endoscopic views: (A) Grade I <50%, (B) Grade II 51-70%, (C) Grade III >71%, (D) Grade IV complete obstruction (Cummings, Ch. 209)
Grading formula:
The lumen cross-sectional area = πr². Reducing the radius from 4 mm to 3 mm decreases the airway area by 40% - illustrating why even 1 mm of narrowing is clinically significant in infants.
8. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing features |
|---|---|
| Subglottic hemangioma | Asymmetric, often left-sided, "steeple sign" on X-ray, cutaneous hemangiomas (beard distribution), progressive enlargement then resolution, responds to propranolol |
| Subglottic cysts | Post-intubation; appear as smooth rounded masses |
| Recurrent croup | No fixed anatomical narrowing on MLB |
| Laryngomalacia | Supraglottic; inspiratory only stridor; improves prone; gets better with age |
| Vascular ring | Extrinsic compression; confirmed on CT/MRI angiography |
| Foreign body | History; radiological evidence |
9. MANAGEMENT
Management is individualized based on:
- Patient's age and overall health
- Severity grade (Myer-Cotton)
- Type (membranous vs. cartilaginous)
- Associated congenital anomalies
- Length and location of stenosis
Key principle (Cummings): Congenital SGS has greater chance of spontaneous resolution than acquired SGS and is associated with fewer symptoms. Many cases can be managed conservatively with watchful waiting.
Figure 5 - Management Algorithm (Cummings, Fig. 209.7)
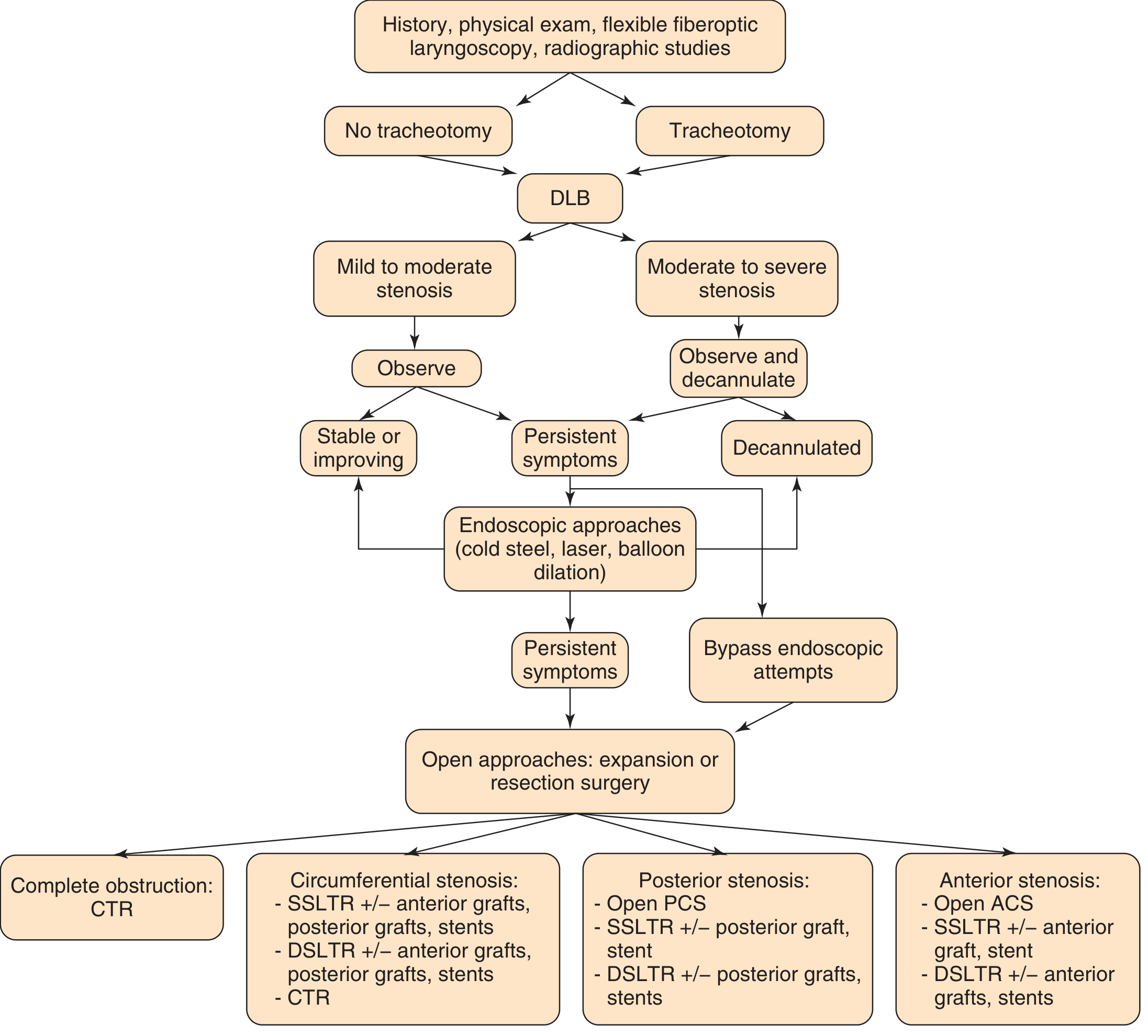
Fig. 209.7 - General algorithm for management of laryngeal stenosis (Cummings, Ch. 209)
A. CONSERVATIVE (WATCHFUL WAITING)
Indications: Grade I, mild Grade II, especially membranous type
- As the child grows, the airway lumen expands proportionally
- Vigorous management of URTIs:
- Inhaled/oral/parenteral corticosteroids (reduce mucosal edema)
- Nebulized racemic epinephrine (vasoconstriction, reduces edema)
- Antibiotics as indicated
- Regular follow-up with repeat MLB
- Less than half of patients with congenital SGS require tracheotomy
B. ENDOSCOPIC MANAGEMENT
Indications: Mild-moderate stenosis (Grade I-II), soft/membranous type; selected Grade III membranous
Techniques:
- Balloon dilation - applies radial pressure to the airway lumen; sized by patient age; preferred over rigid dilation which applies shearing force
- CO2 laser / Cold steel radial incisions - incisions at 12, 3, and 9 o'clock positions through scar while preserving cricoid cartilage
- Intralesional steroid injection - triamcinolone/mitomycin-C; controversial evidence for efficacy
- Mitomycin-C topical application - inhibits DNA/protein synthesis; reduces scar reformation; most effective on fresh/young scar
Contraindication: Cartilaginous congenital SGS - dilatation/laser cannot expand the thickened cartilaginous ring and will worsen the condition
(Scott-Brown Vol 2, Ch. 30; Cummings Ch. 209)
Figure 6 - Endoscopic repair: radial incisions and balloon dilation
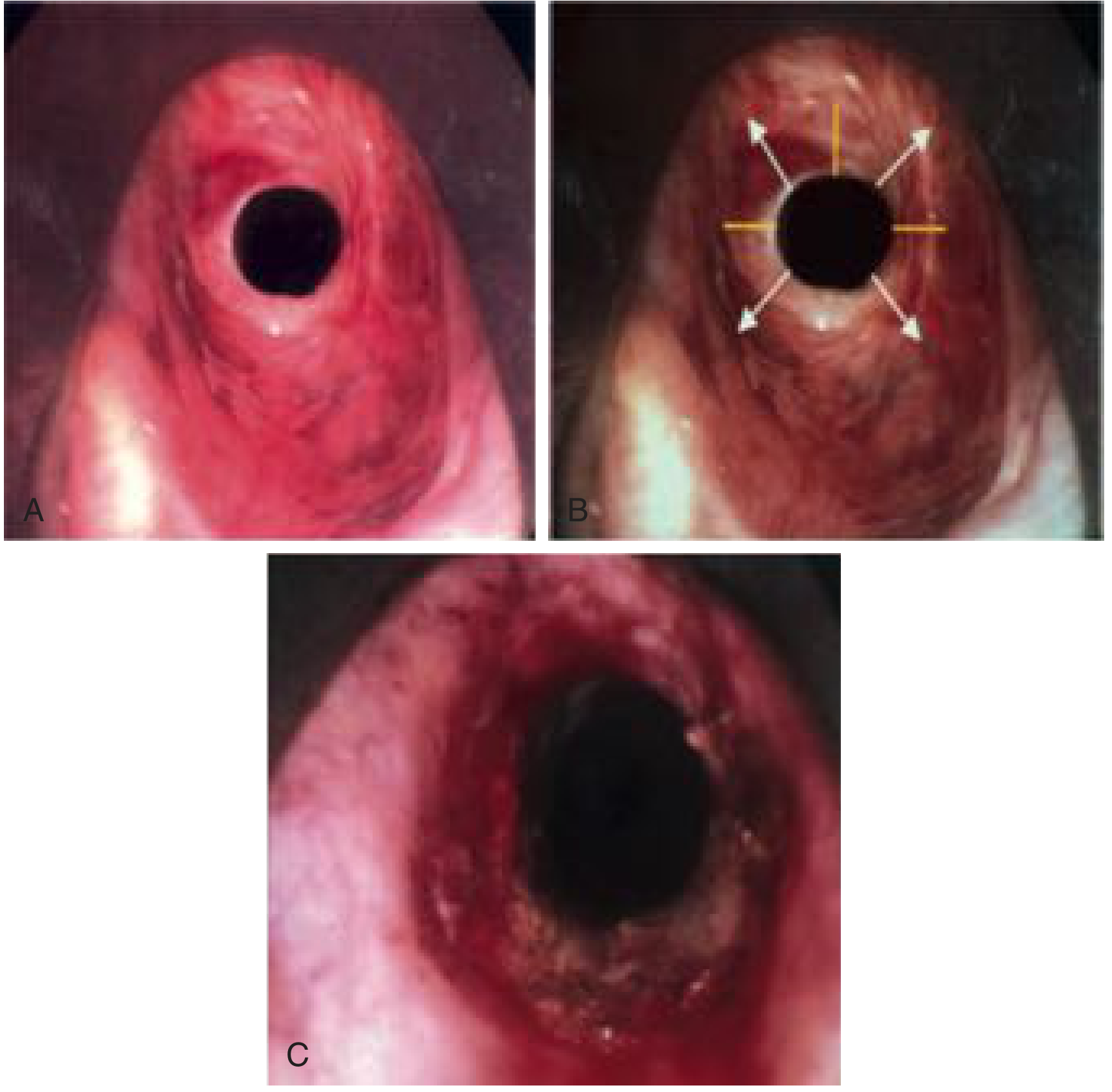
Fig. 209.8 - Endoscopic repair: (A) Preoperative view, (B) Planned radial incisions at 12, 3, 9 o'clock, (C) After cuts and balloon dilation (Cummings, Ch. 209)
C. ANTERIOR CRICOID SPLIT (ACS)
Description (Cotton, 1980): Midline vertical incision through the anterior cricoid cartilage, lower 2 thyroid cartilage rings, and upper 2 tracheal rings. No cartilage graft inserted. Endotracheal tube acts as a stent.
Indications (Classic Cotton criteria):
- Weight >1500 g
- Failed extubation x2
- No supplemental O2 required for >10 days
- No acute respiratory illness
- No congestive heart failure
- Steroid and diuretic therapy not required for >10 days
D. LARYNGOTRACHEAL RECONSTRUCTION (LTR) - MAINSTAY OF SURGICAL TREATMENT
Devised primarily by Cotton (early 1980s); evolved from the castellated laryngotracheoplasty of Evans and Todd (1970s).
Principle: Augmentation of the laryngotracheal complex by anterior and/or posterior midline incision of the cricoid with insertion of costal cartilage grafts to expand the airway.
LTR by Grade:
| Grade | Procedure |
|---|---|
| Grade I | Usually no surgical intervention required |
| Grade II | LTR with anterior costal cartilage graft ± posterior cricoid split |
| Mild Grade III | Anterior graft + posterior cricoid split ± posterior cartilage graft |
| Severe Grade III (pinhole) | Anterior + posterior cartilage grafts |
| Grade IV | Anterior + posterior grafts + prolonged stenting |
Two-stage LTR (DSLTR): Tracheotomy maintained; laryngotracheal stent placed; stent removed weeks later; tracheotomy decannulated after confirming airway adequacy.
Single-stage LTR (SSLTR): No tracheotomy; endotracheal tube used as internal stent for 5-7 days; preferred in specialist centers with appropriate anesthesia support.
For congenital SGS specifically (Scott-Brown): LTR may be combined with submucosal resection of cartilage to "core out" the thickened anterior cricoid ring. Stenting is essential in this situation.
E. PARTIAL CRICOTRACHEAL RESECTION (PCTR / CTR)
Introduced to pediatrics by Monnier et al. (early 1990s).
Principle: Complete resection of the stenotic cricoid segment with end-to-end anastomosis of the tracheal stump to the thyroid cartilage. Since the stenotic segment is entirely removed, the Myer-Cotton grade is NOT a predictor of success/failure (unlike LTR).
Indications: Severe Grade III and Grade IV; failed LTR; longer segment involvement.
Results (Scott-Brown):
- Decannulation rate: 98% for primary PCTR
- Decannulation rate: 94% for salvage PCTR after failed prior reconstruction
F. TRACHEOTOMY
Indications: Severe airway compromise; while awaiting definitive repair; inoperable cases.
- Placed between 2nd and 3rd tracheal rings ideally
- Smallest tube permitting adequate ventilation to minimize further injury
- Long-term tracheotomy in children leads to speech delay, tracheomalacia, suprastomal collapse
Flowchart 3: Surgical Decision by Grade (Scott-Brown Vol 2)
Congenital SGS
|
┌──────┬─────────┬────────────┐
Grade I Grade II Grade III Grade IV
| | | |
Observe LTR Mild III: Ant + Post
+ Ant graft + grafts +
Ant Post split prolonged
graft ± Post graft stenting
Severe III: OR PCTR
Ant + Post
grafts
OR PCTR
10. OUTCOMES
- Grade I and II: >90% success with LTR (Scott-Brown)
- Grade III and IV: 80-90% success with LTR
- PCTR: ~98% decannulation for primary; ~94% for revision surgery
- Congenital SGS generally has better prognosis than acquired SGS
- The best chance for successful repair lies in the initial operation - repeat surgery is more complex
11. ASSOCIATED CONDITIONS
| Condition | Mechanism |
|---|---|
| Down syndrome (Trisomy 21) | Elliptical cricoid cartilage |
| 22q11 deletion (DiGeorge) | Anterior glottic web with subglottic extension |
| Laryngeal cleft | Occult posterior LC + absent posterior cricoid cartilage |
| Laryngeal atresia | Extreme form of failed canalization |
| Laryngeal webs | Incomplete canalization at glottic-subglottic level |
12. RECENT ADVANCES (2021-2026)
Based on Kennedy AA & Smith MM, Otolaryngol Clin North Am (2026) and Smith MM & Buck LS, Expert Rev Respir Med (2022):
-
Multidisciplinary team (MDT) approach - now considered essential: otolaryngology, speech-language pathology, gastroenterology (GERD management), pulmonology, anesthesia, and cardiology as needed
-
Balloon dilation as primary endoscopic tool - preferred over rigid dilation due to radial pressure application; used even for Grade III stenosis to defer or avoid open surgery
-
Propranolol for subglottic hemangioma (key differential) - oral propranolol has become first-line, avoiding tracheotomy and open surgery
-
Tracheal transplantation - emerging research area for severe/complex laryngotracheal stenosis; still experimental
-
3D-printed costal cartilage scaffolds - under investigation as graft substitute in LTR
-
Revision airway surgery - increasingly recognized challenge as children age post-reconstruction; unique anatomical and functional considerations
-
Single-stage LTR expanding - more centers performing SSLTR avoiding long-term tracheotomy; requires dedicated anesthetic expertise
-
Thulium and fiber-based CO2 lasers - improved accuracy and access to difficult sites compared to conventional CO2 laser delivery systems
-
GERD management - anti-reflux therapy routinely used perioperatively (though direct causal evidence remains controversial); uncontrolled GERD is associated with worse LTR outcomes
-
Genetic testing - increasing recognition of chromosomal/syndromic associations (Trisomy 21, 22q11) warrants genetic workup in all congenital SGS cases
13. SUMMARY TABLE (Exam Quick Reference)
| Feature | Detail |
|---|---|
| Definition | Cricoid diameter <4 mm (full-term) or <3.5 mm (preterm) |
| Incidence | 3rd most common congenital laryngeal anomaly; 5% of all SGS |
| Types | Membranous (fibrous/soft) and Cartilaginous (hard/structural) |
| Commonest type | Thickened/deformed cricoid cartilage |
| Grading | Myer-Cotton: Grade I (0-50%), II (51-70%), III (71-99%), IV (100%) |
| Diagnosis | MLB (gold standard) |
| Key clinical feature | Recurrent croup / biphasic stridor |
| Spontaneous resolution | More likely than acquired SGS |
| Contraindication | Dilatation in cartilaginous type |
| Surgery of choice | LTR (laryngotracheal reconstruction) with costal cartilage graft |
| Alternative | PCTR (partial cricotracheal resection) for severe cases |
| Best outcomes | PCTR: 98% decannulation rate |
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed. - Chapters 206, 209
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed., Vol 2 - Chapter 30
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed., Adult Vol - Chapter 76
- KJ Lee's Essential Otolaryngology, 11th Ed.
- Myer CM, O'Connor DM, Cotton RT: Proposed grading system for SGS based on endotracheal tube sizes. Ann Otol Rhinol Laryngol 1994;103:319
- Cotton RT: Management of SGS in infancy and childhood. Ann Otol Rhinol Laryngol 1978;87:649
- Kennedy AA, Smith MM. Subglottic Stenosis. Otolaryngol Clin North Am. 2026. PMID: 42128760
- Smith MM, Buck LS. Update on diagnosis and management of pediatric laryngotracheal stenosis. Expert Rev Respir Med. 2022. PMID: 36347385
- Dhingra PL: Diseases of Ear, Nose and Throat & Head and Neck Surgery
- Hazarika P: Textbook of ENT and Head & Neck Surgery
RGUHS Examination Tip: For a 20-mark answer on congenital SGS, examiners expect: definition with measurements, embryological basis, pathological classification (membranous vs. cartilaginous), Myer-Cotton grading with the diagram, clinical features, MLB as the gold standard for diagnosis, and a logical management plan by grade (watchful waiting → ACS → LTR → PCTR). Always mention that cartilaginous type is a contraindication to dilatation. Recent advances should include propranolol for hemangioma, MDT approach, and tracheal transplantation research.
This is a shared conversation. Sign in to Orris to start your own chat.