A patient presents with vomiting after meals and visible peristalsis in epigastrium. What is the likely condition? Explain the anatomical basis. Mention one congenital and one acquired cause.”
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have comprehensive information from multiple authoritative textbooks. Here is the full synthesized answer:
Gastric Outlet Obstruction (GOO)
Likely Condition
The clinical picture — postprandial vomiting (non-bilious, food-containing) combined with visible left-to-right peristaltic waves across the epigastrium — is characteristic of Gastric Outlet Obstruction (GOO). The obstructed stomach attempts to force its contents past the narrowed pylorus, generating exaggerated peristaltic waves visible through the abdominal wall.
Anatomical Basis
The stomach empties through the pyloric canal, a ~2–3 cm muscular channel that terminates at the pyloric sphincter — a thickened ring of circular smooth muscle that controls gastric emptying. This structure lies at the junction of the stomach and the first part of the duodenum, just to the right of the midline at the level of the transpyloric plane (L1).
When the pyloric canal is narrowed or obstructed:
- Gastric distension occurs as contents accumulate proximally.
- The stomach mounts increasingly forceful peristalsis against the obstruction — visible through the thin anterior abdominal wall as epigastric peristaltic waves moving from left (fundus) to right (pylorus).
- Eventually, intragastric pressure overcomes the lower esophageal sphincter, producing projectile vomiting of undigested, non-bilious gastric contents (bile cannot reflux past the obstruction from below).
- The vomitus is non-bilious because the block is proximal to the ampulla of Vater — bile and pancreatic juice cannot enter.
Anatomically, hyperplasia or fibrosis of the muscularis propria of the pyloric region causes outflow tract obstruction; this may be worsened by mucosal/submucosal edema.
"In some cases, abnormal left-to-right peristaltic waves are seen across the upper abdomen just prior to emesis." — Robbins, Cotran & Kumar: Pathologic Basis of Disease
Congenital Cause: Hypertrophic Pyloric Stenosis (HPS)
| Feature | Detail |
|---|---|
| Pathology | Hyperplasia + hypertrophy of the circular (and to a lesser degree, longitudinal) muscularis propria of the pylorus |
| Incidence | ~1 in 300–900 live births; male:female = 4–5:1 |
| Presentation | 3rd–6th week of life; forceful projectile non-bilious vomiting after feeds; infant re-demands feeding immediately |
| Signs | Visible peristaltic waves; palpable firm "olive-shaped" mass in RUQ/epigastrium (up to 90% of cases) |
| Metabolic | Hypochloremic, hypokalemic metabolic alkalosis from loss of gastric HCl |
| Genetics | High concordance in monozygotic twins; GWAS-linked genes; erythromycin/azithromycin in first 2 weeks is a risk factor |
| Diagnosis | Ultrasound (gold standard): pyloric muscle thickness ≥4 mm, canal length ≥16 mm |
| Treatment | Ramstedt pyloromyotomy — longitudinal incision through the pyloric muscularis (curative) |
"The circular muscles and, to a lesser degree, the longitudinal muscles in the pyloric region are hypertrophied…This results in severe stenosis of the pyloric canal and obstruction of the passage of food." — The Developing Human: Clinically Oriented Embryology
Acquired Cause: Peptic Ulcer Disease (PUD)–related Pyloric Stenosis
| Feature | Detail |
|---|---|
| Pathology | Fibrous scarring/stricture of the pyloric channel from repeated peptic ulceration and healing; can also occur from acute edema around an active pyloric channel ulcer |
| Mechanism | Chronic inflammation → fibrosis → fixed narrowing of pyloric lumen |
| Presentation | Adults; history of epigastric pain, antacid use; gradual onset of postprandial vomiting; succussion splash on examination |
| Other acquired causes | Carcinoma of distal stomach/pancreas causing malignant infiltration or extrinsic compression; antral gastritis |
| Treatment | H. pylori eradication + PPI; endoscopic balloon dilation; surgery (gastrojejunostomy or antrectomy) for refractory cases |
"Acquired pyloric stenosis occurs in adults because of antral gastritis or peptic ulcers close to the pylorus. Other causes include carcinomas of the distal stomach and pancreas that narrow the pyloric channel due to fibrosis or malignant infiltration." — Robbins, Cotran & Kumar: Pathologic Basis of Disease
Imaging — Hypertrophic Pyloric Stenosis
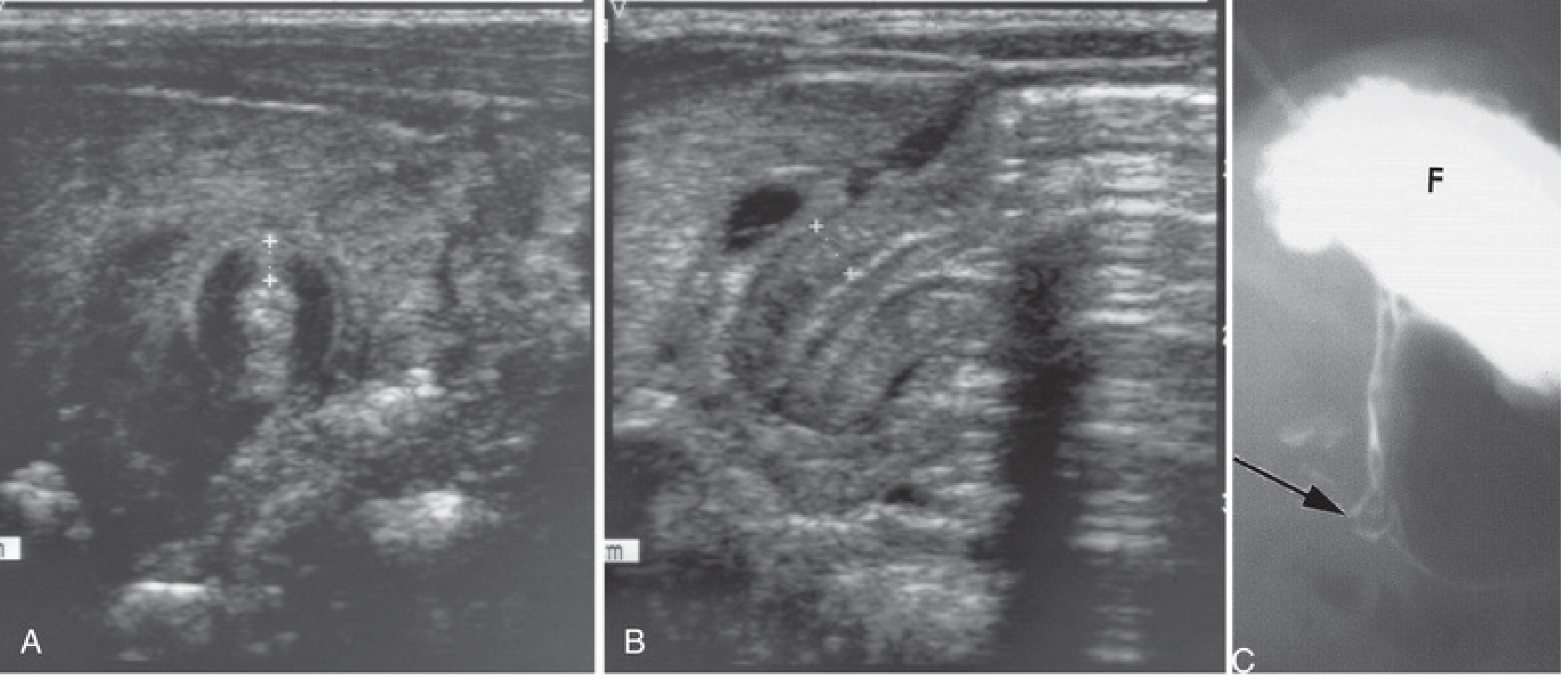
(A) Transverse ultrasound: pyloric muscle wall thickness >4 mm. (B) Horizontal ultrasound: pyloric channel length >14 mm. (C) Contrast radiograph: narrowed pyloric end (arrow) with markedly distended gastric fundus (F) — The Developing Human: Clinically Oriented Embryology
Summary Table
| Feature | Congenital (HPS) | Acquired (PUD Stricture) |
|---|---|---|
| Age | 3–6 weeks of life | Adults (30–60 yrs) |
| Onset | Progressive over days | Insidious over weeks–months |
| Vomiting | Projectile, non-bilious, post-feed | Non-bilious, postprandial |
| Mass | Palpable "olive" | Absent |
| Succussion splash | May be present | Characteristically present |
| Metabolic disturbance | Hypochloremic, hypokalemic alkalosis | Same if prolonged |
| Key investigation | Ultrasound | Endoscopy + biopsy |
| Treatment | Pyloromyotomy | Medical/endoscopic/surgical |
Sources: Robbins, Cotran & Kumar: Pathologic Basis of Disease | The Developing Human: Clinically Oriented Embryology | Current Surgical Therapy 14e | Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.