A 72-year-old male with complaints of chest pain showing ST elevation in the ECG. What are the differentials?
Reading File
Finding Sources
Finding Sources
Searching PubMed
ST elevation differential diagnosis
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, clinically organized answer based on Rosen's Emergency Medicine, The Washington Manual of Medical Therapeutics, and supporting sources.
Differentials for ST Elevation with Chest Pain in a 72-Year-Old Male
In any adult presenting with chest pain and ST elevation, STEMI must be assumed until proven otherwise - but recognizing the full differential is essential to avoid misdiagnosis and inappropriate reperfusion therapy.
1. STEMI (ST-Elevation Myocardial Infarction) - Most Important to Rule In/Out
This is the top priority. The classic convex ("tombstone" or domed) ST morphology with reciprocal changes in contralateral leads is characteristic. Coronary territory localization:
- Anterior wall: ST elevation in V1-V4 (LAD territory)
- Inferior wall: ST elevation in II, III, aVF (RCA or LCx)
- Lateral wall: ST elevation in I, aVL, V5-V6 (LCx)
- Posterior MI: ST depression in V1-V3 (mirror image)
- Right ventricular MI: ST elevation in right-sided leads (RV3-RV6) - always check right-sided leads in inferior STEMI
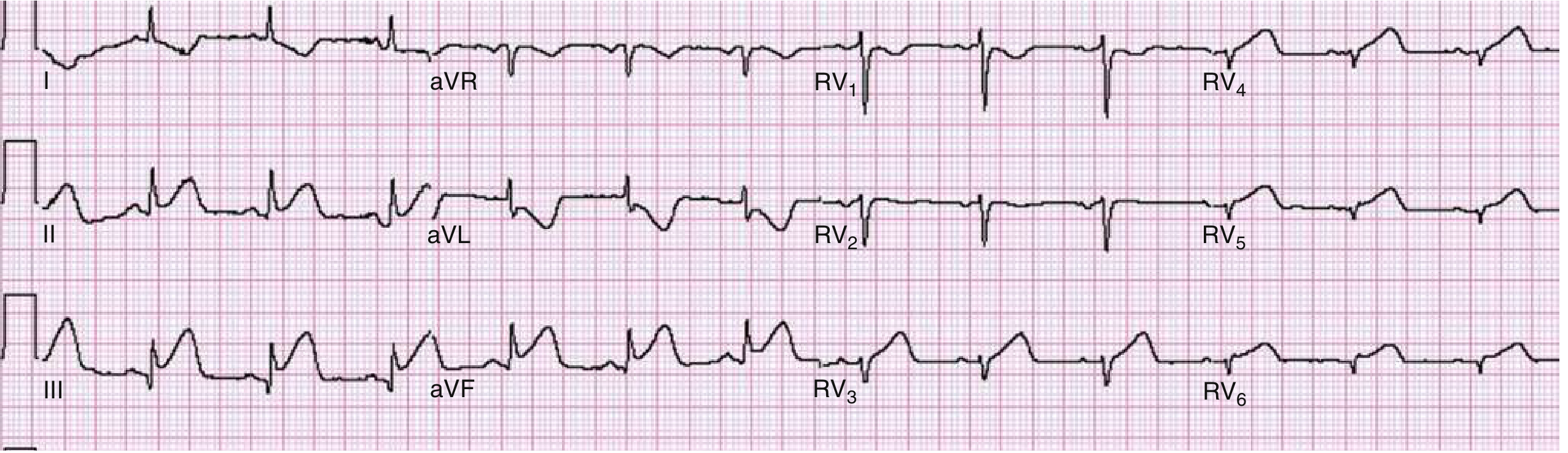
Right ventricular infarction - ST elevation in right-sided precordial leads (Rosen's EM)
Key feature: Convex/domed ST morphology + reciprocal ST depression + regional distribution.
2. Pericarditis
Diffuse ST elevation (present in nearly all leads except aVR, where it is depressed). Key distinguishing features:
- ST segments are concave (saddle-shaped), not convex
- ST elevation usually <5 mm
- PR segment depression in inferior leads and V6 - insensitive but specific
- PR segment elevation in aVR
- No reciprocal changes
- Pleuritic, positional chest pain (worse supine, better leaning forward)
"Convex or domed ST segment morphology strongly suggests STEMI" - Rosen's Emergency Medicine
In a 72-year-old, viral pericarditis is less common; consider uremic pericarditis, post-MI (Dressler syndrome), or malignancy-related.
3. Aortic Dissection (with Coronary Involvement)
Critical mimic in elderly males. If dissection extends to involve the right coronary ostium, it produces an inferior STEMI pattern. This is a high-stakes differential because fibrinolytic therapy would be catastrophic. Clues:
- Tearing, ripping pain radiating to the back
- Blood pressure differential between arms
- Widened mediastinum on CXR
- New aortic regurgitation murmur
4. Left Ventricular Aneurysm (LVA)
A complication of prior MI. The ECG shows persistent ST elevation with Q waves in the same territory (often anterior). Key distinction: this is a chronic finding with temporal stability - there is no acute change. The ST elevation of LVA is regional (not diffuse), and the patient may have a known history of MI or heart failure.
5. Acute Myocarditis
The ECG can show ST elevation virtually indistinguishable from STEMI, and troponin is elevated. As Harrison's notes, "the combination of chest pain, ECG changes, and elevated troponin is typical of both acute myocarditis and myocardial infarction." Workup includes cardiac MRI with late gadolinium enhancement. Coronary angiography is often needed to exclude obstructive CAD.
6. Left Bundle Branch Block (LBBB) / Left Ventricular Hypertrophy (LVH)
Both produce secondary ST-T changes, including ST elevation in the right precordial leads (V1-V3) and ST depression in lateral leads. This is called discordant ST change - normal in LBBB/LVH. The Sgarbossa criteria help identify superimposed STEMI on LBBB (concordant ST elevation ≥1 mm, or ST elevation ≥5 mm in discordant leads). In a 72-year-old with hypertension or cardiomegaly, LVH is common.
7. Prinzmetal (Vasospastic) Angina
Coronary artery spasm produces transient ST elevation that resolves spontaneously or with nitrates. It typically occurs at rest, often at night or in early morning, and is not provoked by exertion. The coronary arteries may be angiographically normal. Less common in elderly males than in younger patients, but possible - especially with cocaine use (a classic cause at any age).
8. Pulmonary Embolism
PE can produce ST elevation - typically in lead III and V1, and occasionally aVR. The classic S1Q3T3 pattern plus sinus tachycardia is more characteristic. Right heart strain pattern (V1-V4 ST changes, new RBBB) may be seen. In a 72-year-old with chest pain, hypoxia, and tachycardia, PE must be considered even if the ECG shows ST changes.
9. Brugada Syndrome
A channelopathy producing a characteristic coved-type ST elevation in V1-V3 that can be confused with anterior STEMI. It is associated with sudden cardiac death due to ventricular fibrillation. While it typically presents in younger adults, it can be unmasked later in life by fever, medications (Class IA/IC antiarrhythmics, TCAs, beta-blockers), or electrolyte abnormalities.
10. Hyperkalemia
Severe hyperkalemia produces a progression of ECG changes: peaked T waves → widened QRS → sine-wave pattern → ST elevation → VF/asystole. In a 72-year-old with CKD, this is worth checking immediately. It is reversible with treatment.
11. Benign Early Repolarization (BER)
A normal ECG variant with concave ST elevation (J-point notching), symmetric tall T waves, predominantly in V2-V5, and relative temporal stability. BER is a diagnosis of exclusion in the acute setting - it is less likely in a 72-year-old presenting with new chest pain. In general, BER tends to regress with advancing age.
12. Other Less Common Causes
| Cause | Mechanism / Clue |
|---|---|
| Ventricular paced rhythm | Pacemaker spike before QRS; discordant ST changes |
| Osborn waves (hypothermia) | Positive deflection at J point; hypothermia history |
| Acute cerebral hemorrhage (Intracranial) | Diffuse, often dramatic ST-T changes; associated neurological findings |
| Post-electrical cardioversion | Transient ST elevation immediately after DC cardioversion |
| Hypertrophic cardiomyopathy | ST changes with outflow obstruction murmur |
| Takotsubo cardiomyopathy | Stress-induced; ST elevation + apical ballooning; common in elderly patients after emotional/physiological stress |
Prioritization in This Patient
Given that the patient is a 72-year-old male, the following should be the immediate focus:
- STEMI - treat as STEMI until proven otherwise; activate cath lab
- Aortic dissection - rule out before any anticoagulation; chest X-ray + CT-aorta if suspected
- Pericarditis/Myocarditis - diffuse ST elevation + concavity + PR depression
- Pulmonary embolism - especially if tachycardic and hypoxic
- LV aneurysm - if prior MI history with stable, chronic ST changes
Key workup: Serial ECGs, high-sensitivity troponin, CXR, bedside echo (assesses wall motion, pericardial effusion, aortic root), and blood pressure in both arms. Do NOT delay reperfusion therapy while awaiting troponin results if the ECG is diagnostic.
Sources: Rosen's Emergency Medicine, Table 64.3 and ECG Differential Diagnosis of ST Segment Elevation (pp. 1002-1007); The Washington Manual of Medical Therapeutics, Differential Diagnosis of ST-Segment Elevation (p. 149); Harrison's Principles of Internal Medicine 22E, Presentation and Diagnosis.
This is a shared conversation. Sign in to Orris to start your own chat.