CSF Rhinnorhea
Reading File
Finding Sources
Searching PubMed
"CSF rhinorrhea" AND management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
CSF rhinorrhea etiology diagnosis management endoscopic repair
Searching Images
CSF rhinorrhea skull base defect endoscopic repair
Reading Web Page
https://emedicine.medscape.com/article/861126-treatment
I now have comprehensive information to provide a detailed answer. Let me compile it.
CSF Rhinorrhea
Definition
CSF rhinorrhea is the clear nasal discharge resulting from an abnormal communication (fistula) between the subarachnoid space and the nasal cavity or paranasal sinuses, caused by simultaneous defects in the dura, arachnoid, and skull base. It may occur via the anterior cranial fossa directly, or indirectly from the middle/posterior fossa via the Eustachian tube.
Etiology & Classification
| Category | Examples |
|---|---|
| Traumatic (most common, ~80%) | Fronto-basal skull fractures, penetrating injuries |
| Iatrogenic/Postoperative | FESS, pituitary surgery, craniotomy, spinal procedures |
| Spontaneous/Idiopathic | Often associated with elevated ICP (obese patients, obstructive sleep apnea, idiopathic intracranial hypertension) |
| Tumour-related | Meningioma en plaque eroding skull base, pituitary tumours |
| Congenital | Encephalocele, meningocele through skull base |
Common leak sites (anterior to posterior):
- Cribriform plate / horizontal lamella — most common (fovea ethmoidalis)
- Posterior ethmoid roof
- Sphenoid sinus (sella, lateral recess)
- Frontal sinus posterior table
Clinical Features
- Unilateral, clear, profuse, watery nasal discharge — salty or metallic taste
- Positional: increases when leaning forward ("reservoir sign") or valsalva
- Associated features: anosmia/hyposmia (cribriform plate defect), headache, history of trauma or prior sinus/skull base surgery
- Halo sign: CSF spreads with a clear halo around blood on filter paper
Diagnosis
Biochemical Testing
| Test | Notes |
|---|---|
| Beta-2 transferrin assay | Gold standard — high sensitivity & specificity; CSF-specific isoform not found in serum, nasal secretions, or tears |
| Beta-trace protein | Alternative; elevated in CSF |
| Glucose oxidase (dipstick) | Low specificity — not recommended as sole test |
Imaging
| Modality | Role |
|---|---|
| High-resolution CT (fine-cut coronal) | First-line — identifies bony defect, sinus opacification at leak site; technique of choice for localization |
| MRI with T2/CISS sequences | Detects soft tissue herniation (encephalocele, meningocele), dural enhancement; complements CT |
| MR cisternography | Useful for intermittent leaks; shows CSF tracking |
| CT cisternography (intrathecal contrast) | High sensitivity for active leaks; invasive; used when non-invasive imaging inconclusive |
| Intrathecal fluorescein | Intraoperative use — confirms site of leak endoscopically |
Endoscopic Examination
Nasal endoscopy is essential for direct visualization of the leak site and mucosal assessment prior to surgery.
Complications
- Meningitis — most feared complication (typically Streptococcus pneumoniae, Haemophilus influenzae)
- Risk ~10% in first 3 weeks post-trauma
- Rises to ~40% in non-traumatic/spontaneous CSF rhinorrhea
- Iatrogenic leaks carry ~20% meningitis risk if managed non-surgically long-term
- Pneumocephalus
- Brain abscess
- Recurrent meningitis
Management
1. Conservative (Traumatic CSF Rhinorrhea)
- 5–7 day trial for post-traumatic leaks (majority resolve spontaneously)
- Head of bed elevated 15–30°
- Avoidance of nose blowing, sneezing, straining, heavy lifting
- Stool softeners
- Lumbar drainage (CSF diversion) — for persistent or high-flow leaks
- Antibiotic prophylaxis: controversial; not universally recommended
Leaks persisting >7 days have significantly increased meningitis risk → surgical repair warranted.
2. Surgical Repair — Indications
- All spontaneous or iatrogenic CSF leaks (surgical repair recommended unless contraindicated)
- Traumatic leak failing conservative management (>7 days)
- Large bony defect identified at time of injury
- Recurrent meningitis
- Intracranial complications
3. Endoscopic Repair (Preferred Approach)
Success rate: 90–97% with significantly lower morbidity than open craniotomy.
Steps:
- Identify the leak site (fluorescein-assisted endoscopy, pre-op imaging)
- Remove adjacent sinus mucosa to create denuded bone for graft adherence
- Remove residual bony partitions to create a flat surface
- Graft placement:
- Small defects: Free mucosal graft (middle turbinate, nasal floor), fat graft, fascial graft (fascia lata, temporalis), absorbable packing
- Large defects / high-flow / elevated ICP: Vascularized pedicled nasoseptal flap (NSF) — based on distal branch of sphenopalatine artery; provides robust, well-vascularized repair
- Multi-layer closure: Fat/fascia underlay + overlay graft secured with absorbable collagen packing ± nonabsorbable sponge layer
- Postoperative: lumbar drain may be left for 3–5 days; head CT ± MRI to rule out intracranial bleeding
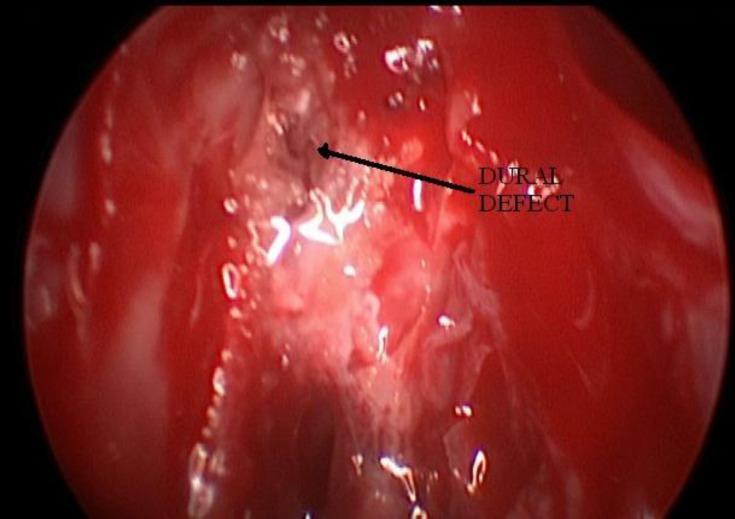
Endoscopic view showing a dural defect (arrow) during CSF rhinorrhea repair — the small dark focal point within erythematous ethmoidal tissue.

Composite: (A) CSF leak at right olfactory fissure; (B) 1.2 cm cribriform plate defect with dural exposure; (C) Multi-layer closure with abdominal fat graft.

Clival CSF leak repair: (a) Fluorescein identifies dural defect; (b) Bovine pericardium onlay graft; (c) Pedicled nasoseptal flap completing multi-layer closure.
4. Open (Intracranial) Approaches
- Frontal craniotomy (Dandy, 1926) — historical; still used when endoscopic access limited
- Extracranial approaches — declining use
- Required for: defects not accessible endoscopically, associated intracranial pathology
5. Postoperative Care (Iatrogenic Leaks)
Per KJ Lee's Essential Otolaryngology:
- Early repair is mandatory — iatrogenic leaks have 20% meningitis incidence with non-surgical management
- Neurosurgical and infectious disease consultations
- Post-op head CT and MRI to exclude intracranial complications
Recurrence & Factors for Failure
- Multiple simultaneous leak sites (not identified intraoperatively)
- Large defect (>3 cm)
- Persistent elevated ICP (spontaneous rhinorrhea patients — obesity, IIH)
- Chronic cough
- Recurrence rate with endoscopic repair: ~6%; revision endoscopic success ~97%
Spontaneous CSF Rhinorrhea — Special Considerations
Patients with spontaneous leaks frequently have elevated ICP (idiopathic intracranial hypertension). Surgical repair alone does not address the underlying cause. Multidisciplinary management should include:
- Neurology/neurosurgery consultation (ICP monitoring, CSF diversion)
- Weight management
- Sleep apnea evaluation
- Acetazolamide or other ICP-lowering agents
Recent Evidence
A 2026 meta-analysis (PMID 40650638) confirms favorable outcomes of endoscopic management for spontaneous CSF rhinorrhea, reinforcing endoscopy as the standard of care. A 2024 systematic review (PMID 39738756) examines evidence-based approaches in low- and middle-income settings, highlighting resource-appropriate management pathways.
Sources: K.J. Lee's Essential Otolaryngology, 11th ed.; Cummings Otolaryngology Head and Neck Surgery; Medscape Reference; PMC; Springer Nature Reference Works.
This is a shared conversation. Sign in to Orris to start your own chat.