Can you make a detailed notes on puberty normal and abnormal
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed to compile thorough, detailed notes. Let me compile the comprehensive notes.
Puberty: Normal and Abnormal - Detailed Notes
Sources: Medical Physiology (Boron & Boulpaep), Ganong's Review of Medical Physiology 26th Ed., Harrison's Principles of Internal Medicine 22E (2025), Textbook of Family Medicine 9e, Goldman-Cecil Medicine
PART 1: NORMAL PUBERTY
1.1 Definition
Puberty is the transition between the juvenile and adult states during which an individual becomes capable of reproduction. It involves both the physical maturation of the gonads and the development of secondary sexual characteristics. The terms "puberty" and "adolescence" are often used interchangeably, though strictly defined, puberty is the moment when endocrine and gametogenic functions first allow reproduction.
1.2 Two Key Physiological Processes
Puberty involves two distinct but overlapping physiological processes:
1. Gonadarche
- Physical and functional maturation of the gonads
- Gonads begin producing gametes and sex steroids
- Driven by rising FSH and LH from the anterior pituitary
- In males: leads to spermarche (initiation of sperm production)
- In females: leads to folliculogenesis, thelarche (breast development), and menarche (first menstrual period)
2. Adrenarche
- Increased production of adrenal androgens: DHEA, DHEAS, and androstenedione (A4) by the adrenal cortex
- Peculiar to humans and great apes; occurs in both sexes during prepuberty (ages 6-8 years)
- Induces pubarche (growth of pubic and axillary hair)
- Adrenarche begins at age 8-10 in girls and 10-12 in boys
- DHEA peaks at ~age 25 in women, slightly later in men, then declines
- Absence of adrenarche does NOT prevent gonadarche or reproductive competence
1.3 Hormonal Axis - Control of Puberty
The HPG Axis:
- The hypothalamus contains GnRH neurons controlled by higher brain centers integrating multiple physiological signals
- Before puberty: GnRH and gonadotropin levels are low because the HPG axis is highly sensitive to negative feedback by gonadal steroids - even low levels of sex steroids suffice to suppress LH/FSH
- At puberty onset: sensitivity of the HPG axis to negative feedback DECREASES, allowing GnRH pulsatility to emerge
- Earliest event of puberty = onset of pulsatile GnRH release during REM sleep, which gradually extends throughout the day
- Rising FSH and LH from the pituitary then stimulate gonadarche
Key regulators of GnRH secretion (genetic):
- Kisspeptin (KISS1) and its receptor (KISS1R) - positive regulators
- MKRN3 (makorin ring finger protein 3) - inhibitory; mutations cause early puberty
- TAC3, TACR3 - regulate GnRH secretion
- Congenital defects in GnRH neuron migration: ANOS1, PROK2, FGFR1, FGF8, CHD7
Hormonal changes across puberty (Ganong):
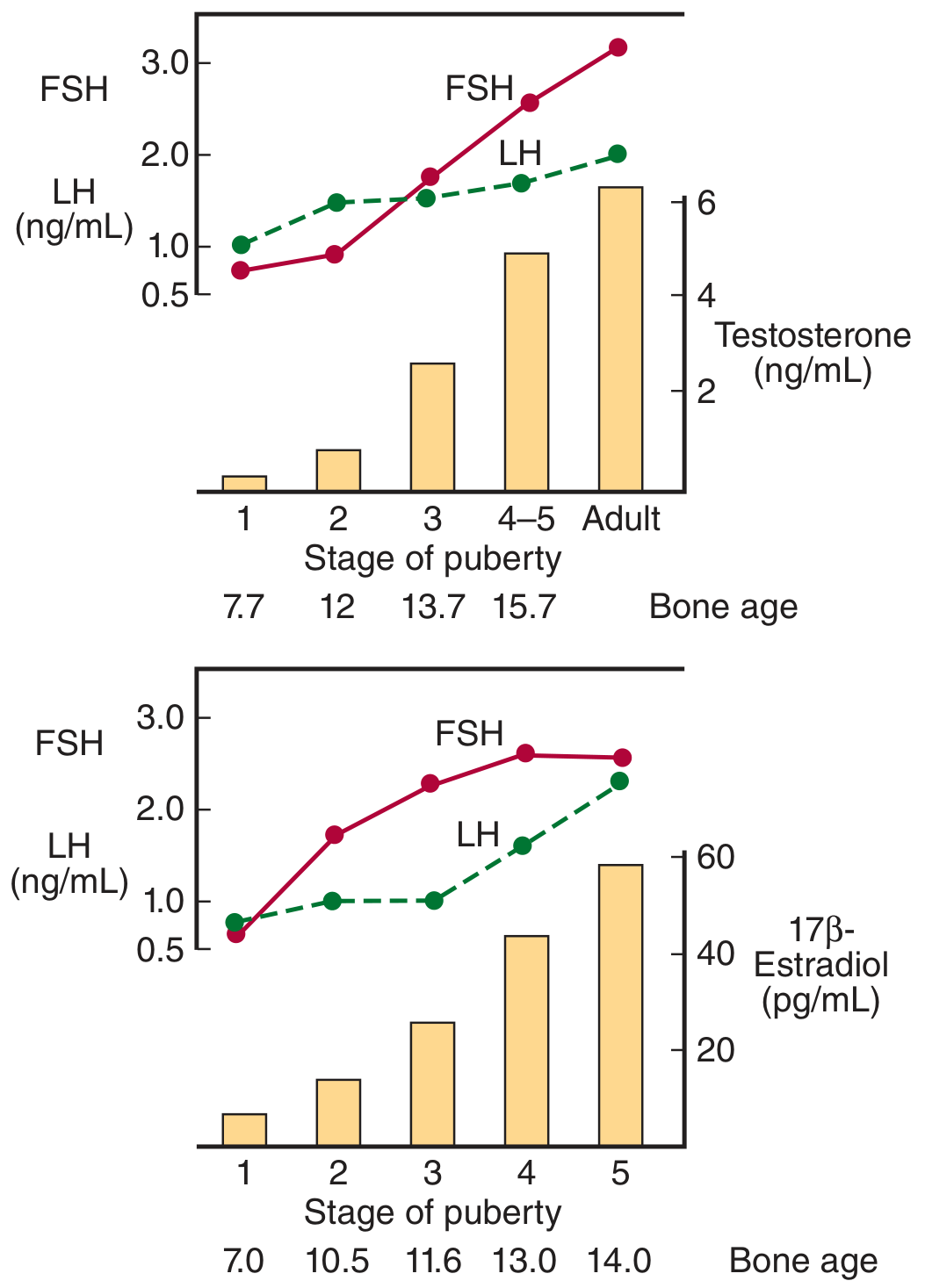
In boys, testosterone rises steeply from Tanner stage 2 onward (bone age ~12). In girls, 17β-estradiol rises from stage 3 onward (bone age ~11.6), with peak levels at stage 5.
1.4 Timing of Normal Puberty
| Parameter | Girls | Boys |
|---|---|---|
| Normal onset | 8-13 years | 9-14 years |
| Precocious if before | 8 years (White), 6 years (Black) | 9 years |
| Delayed if no signs by | 12 years (thelarche) | 14 years (testicular enlargement) |
- Puberty age has been declining in developed countries at 1-3 months per decade for over 175 years
- Adrenarche is the first step (ages 6-10); gonadarche follows
1.5 Tanner Stages
Tanner stages describe the sequential development of secondary sexual characteristics. There are 5 stages.
TANNER STAGES - GIRLS (Breast + Pubic Hair)
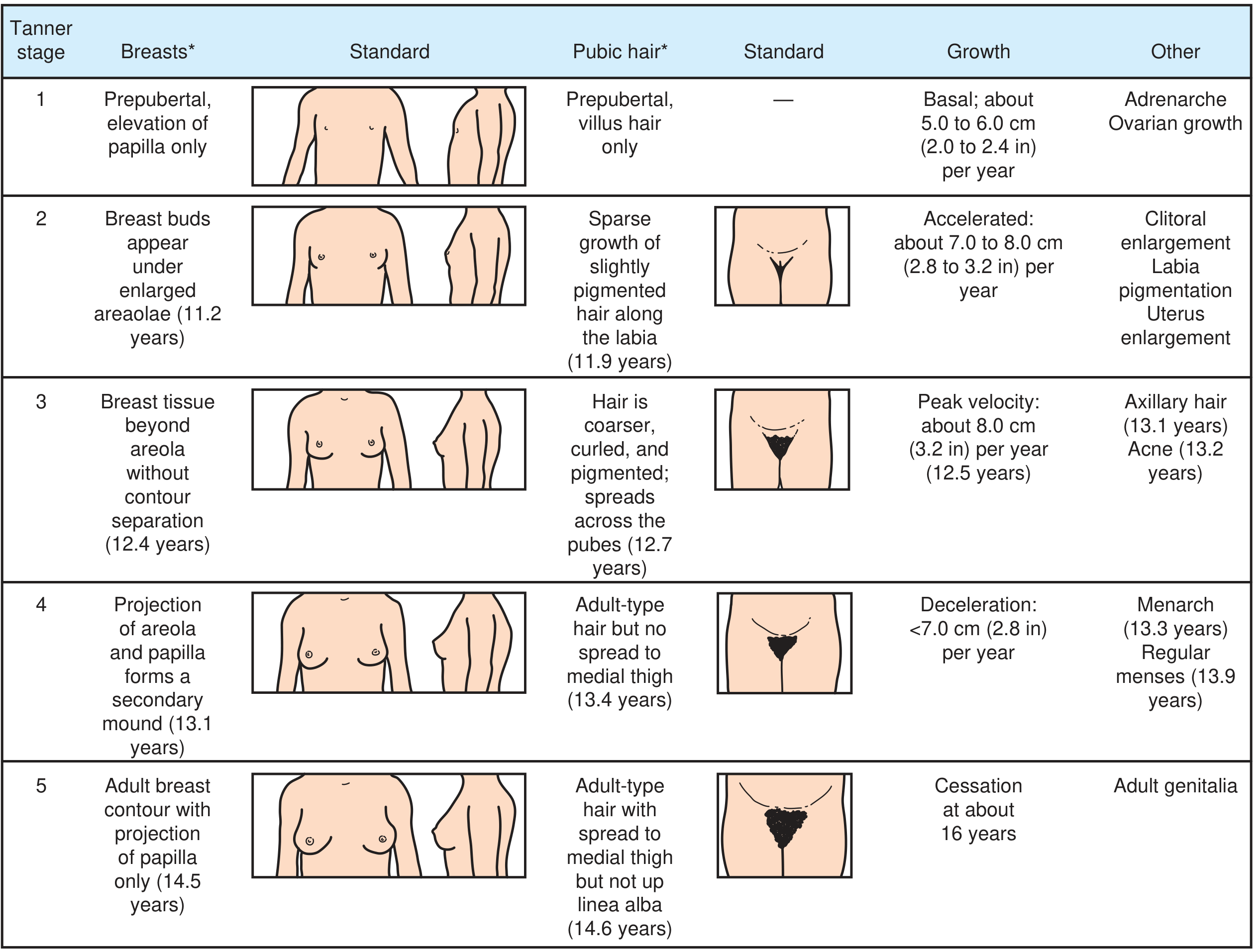
| Stage | Breasts | Pubic Hair | Growth | Other |
|---|---|---|---|---|
| 1 | Prepubertal, papilla elevation only | Prepubertal (villus hair only) | Basal: 5-6 cm/yr | Adrenarche, ovarian growth |
| 2 | Breast buds under enlarged areolae (11.2 yr) | Sparse, slightly pigmented hair along labia (11.9 yr) | Accelerated: 7-8 cm/yr | Clitoral enlargement, labia pigmentation, uterus enlargement |
| 3 | Breast tissue beyond areola, no contour separation (12.4 yr) | Coarser, curled, pigmented hair spreading across pubes (12.7 yr) | Peak velocity: ~8 cm/yr (12.5 yr) | Axillary hair (13.1 yr), acne (13.2 yr) |
| 4 | Areola and papilla project as secondary mound (13.1 yr) | Adult-type hair, no spread to medial thigh (13.4 yr) | Decelerating: <7 cm/yr | Menarche (13.3 yr), regular menses (13.9 yr) |
| 5 | Adult breast contour, papilla only projects (14.5 yr) | Adult-type hair with spread to medial thigh (14.6 yr) | Cessation ~16 yr | Adult genitalia |
TANNER STAGES - BOYS (Genitalia + Pubic Hair)
| Stage | Genitalia | Pubic Hair | Growth | Other |
|---|---|---|---|---|
| 1 | Prepubertal testes <2.5 cm | Prepubertal (villus hair only) | Basal: 5-6 cm/yr | Adrenarche |
| 2 | Scrotal thinning and reddening; testes 2.5-3.2 cm (11.9 yr) | Sparse, slightly pigmented hair at base of penis (12.3 yr) | Basal: 5-6 cm/yr | Decrease in total body fat |
| 3 | Penis elongates; testes 3.3-4.0 cm (13.2 yr) | Thicker, curlier hair spreading to mons pubis (13.9 yr) | Accelerated: 7-8 cm/yr | Gynecomastia (13.2 yr), voice breaks (13.5 yr), muscle mass increases |
| 4 | Penis and glans grow, scrotum darkens; testes 4.1-4.5 cm (14.3 yr) | Adult-type hair, no spread to medial thigh (14.7 yr) | Peak velocity: ~10 cm/yr (13.8 yr) | Axillary hair (14.0 yr), voice change (14.1 yr), acne (14.3 yr) |
| 5 | Adult genitalia; testes >4.5 cm (15.1 yr) | Adult-type hair with medial thigh spread (15.3 yr) | Deceleration and cessation (~17 yr) | Facial hair (14.9 yr), muscle mass continues increasing |
Key note: Testicular enlargement >2.5 cm generally indicates puberty has begun in boys.
1.6 Sequence of Pubertal Events
Girls:
- Adrenarche / pubarche (age 6-8)
- Thelarche - breast bud development (first sign of gonadarche, ~age 10-11)
- Pubic and axillary hair
- Growth spurt (peak at Tanner 3, ~12.5 yr)
- Menarche (Tanner 4, ~13.3 yr) - initial cycles typically anovulatory
- Regular ovulatory cycles (~1 year after menarche)
Boys:
- Adrenarche / pubarche (age 8-10)
- Testicular enlargement (first sign, ~age 11-12)
- Penile growth
- Pubic, axillary, facial hair
- Voice change and gynecomastia (Tanner 3)
- Growth spurt (peak at Tanner 4, ~13.8 yr - later than girls)
- Spermarche
PART 2: ABNORMAL PUBERTY
2.1 Overview - Evaluation Triggers
Evaluation should begin if:
- Signs of puberty in girls younger than 8 years (White) or younger than 6 years (Black)
- Signs of puberty in boys younger than 9 years
- Absence of thelarche by age 12 years in girls
- Absence of testicular enlargement by age 14 years in boys
- Duration between thelarche and menarche >5 years
Initial evaluation includes:
- Detailed history (growth/developmental milestones, medications, diet, family history, ethnicity)
- Physical examination with Tanner staging
- Growth chart from birth to present
- Left wrist X-ray for bone age
- If true precocious puberty suspected: cranial CT or MRI to rule out CNS lesions
PART 3: PRECOCIOUS PUBERTY
3.1 Definition
Precocious puberty = appearance of secondary sexual maturation at an early age:
- Girls: before age 8 (White), before age 6 (Black)
- Boys: before age 9 (all races)
- Boys: progressive testicular enlargement >4 mL before 9 years with linear growth acceleration and advanced bone age
Note: >75% of children investigated for precocious puberty have benign diagnoses (normal variations) requiring no treatment.
3.2 Classification
A. By Terminology:
- Isosexual precocity: Signs consistent with the child's own gender (e.g., feminization of a girl, virilization of a boy)
- Heterosexual (contrasexual) precocity: Signs consistent with the opposite gender (e.g., virilization of a girl, breast development in a boy)
- Progressive: Advances one Tanner stage every 3-6 months
- Nonprogressive: No progression of pubertal signs over time
B. By Mechanism - the main classification:
| Type | Mechanism | Also Called |
|---|---|---|
| Central (True) | GnRH-dependent; early HPG axis activation | Gonadotropin-dependent |
| Peripheral (Pseudo) | GnRH-independent; autonomous sex steroid production | Gonadotropin-independent |
| Incomplete / Benign Variants | Partial, isolated development | - |
3.3 Central (GnRH-Dependent) Precocious Puberty
Caused by early activation of hypothalamic GnRH secretion → increased FSH, LH → gonadal stimulation.
Causes:
- Idiopathic (most common, especially in girls) - no identifiable cause
- CNS lesions:
- Hypothalamic hamartoma (most common organic cause)
- Optic glioma, astrocytoma, ependymoma
- Arachnoid cysts
- Tuberous sclerosis
- Inflammatory/infectious lesions
- Genetic mutations: KISS1 (kisspeptin), KISS1R, MKRN3 gain/loss-of-function
- Primary hypothyroidism (severe, prolonged - can trigger central precocity)
- After androgen exposure
- Post-cranial irradiation
Investigations:
- FSH, LH, prolactin, sex steroids, TSH
- Morning testosterone (boys)
- GnRH-agonist stimulation test (females)
- MRI brain - mandatory to rule out CNS pathology, especially in boys
Treatment:
- GnRH agonists (e.g., leuprolide): reversibly inhibit gonadotropin secretion
- Prevent further secondary sexual development
- Prevent early epiphyseal fusion (preserves final adult height)
- Optimal age to discontinue: 11 years; puberty resumes normally after
- Treat underlying CNS lesion if present
- Slowly progressive cases may be managed with observation only
3.4 Peripheral (GnRH-Independent) Precocious Puberty
Sex steroids produced independently of the HPG axis.
Causes in both sexes:
- McCune-Albright syndrome (activating GNAS1 mutation → autonomous gonadal steroidogenesis)
- Adrenal disorders:
- Congenital adrenal hyperplasia (CAH) - most common in girls presenting with virilization
- Adrenal tumors (androgen or estrogen producing)
- Exogenous sex steroid exposure (estrogen creams, medications)
- hCG-secreting tumors (germ cell tumors)
Causes in boys specifically:
- Activating LH receptor mutations - familial male-limited precocious puberty (testotoxicosis)
- Testicular tumors (Leydig cell, Sertoli cell)
McCune-Albright Syndrome (important triad):
- Café-au-lait spots (irregular "coast of Maine" borders)
- Polyostotic fibrous dysplasia
- Peripheral precocious puberty (autonomous gonadal activation)
3.5 Benign Variants / Incomplete Precocious Puberty
These are nonprogressive isolated findings, usually not requiring treatment:
| Condition | Features | Management |
|---|---|---|
| Isolated precocious thelarche | Breast development (unilateral or bilateral) without other pubertal signs; most common in girls <2 years | Usually spontaneously resolves; observe; no treatment |
| Isolated precocious pubarche (adrenarche) | Pubic hair only; due to early adrenarche | DHEAS may be mildly elevated; ACTH stimulation test to exclude late-onset CAH; self-limited |
| Isolated menarche | Isolated vaginal bleeding without other signs | Exclude foreign body, tumor, trauma |
| Adolescent gynecomastia (boys) | Breast tissue enlargement in pubertal boys (Tanner 3) due to estrogen/androgen imbalance | Self-limited; mostly social concern; reassurance |
3.6 Long-Term Consequences of Precocious Puberty
- Shorter final adult height (early epiphyseal fusion)
- Increased risk of breast and endometrial cancer (earlier estrogen exposure)
- Cardiovascular disease, hypertension, type 2 diabetes
- Psychosocial issues (early physical maturity in young children)
- Shorter lifespan
PART 4: DELAYED PUBERTY
4.1 Definition
- Boys: No testicular enlargement by age 14 years OR more than 5 years between initial and complete genital development (up to age 19)
- Girls: No thelarche by age 12 years OR more than 5 years between thelarche and menarche (by age 17)
- Represents 2-2.5 standard deviations above the mean onset age
Delayed puberty is more common in boys than in girls.
Long-term risks: Lower peak bone mass, higher cardiovascular and metabolic risk. Conversely, lower risk of breast/endometrial cancer in women with late puberty.
4.2 Classification and Causes
There are 4 main categories (Harrison's 22E):
| Category | Proportion | Key Features |
|---|---|---|
| 1. Self-limited (constitutional) delay | ~60% of cases | Most common; familial; delayed but spontaneous onset |
| 2. Functional hypogonadotropic hypogonadism | ~20% of cases | Systemic illness, malnutrition, eating disorders |
| 3. Permanent hypogonadotropic hypogonadism (HH) | ~10% of cases | Congenital or acquired HPG axis defects |
| 4. Primary gonadal failure (hypergonadotropic hypogonadism) | ~15% of cases | Gonadal failure; high gonadotropins, low sex steroids |
4.3 Self-Limited (Constitutional) Delay
- Most common cause (~60% of boys, ~30% of girls with delayed puberty)
- Diagnosis of exclusion
- Mechanism: delayed GnRH pulse generation → low gonadotropins
- Height and weight below 5th percentile but catch up during adolescence
- Normal adult height and weight typically achieved
- Family history of delayed puberty in one or both parents (autosomal dominant in some families; X-linked or bilineal in others)
- Lab values remain prepubertal until puberty eventually begins
- FSH, LH, DHEA-S, prolactin, testosterone, estradiol: all prepubertal
4.4 Functional Hypogonadotropic Hypogonadism
Low FSH and LH due to suppression of GnRH pulsatility by systemic factors.
Causes:
- Anorexia nervosa / eating disorders
- Excessive weight loss or low body fat
- Extreme exercise (e.g., competitive female athletes, long-distance runners)
- Chronic disease (inflammatory bowel disease, celiac disease, renal failure, etc.)
- Malnutrition
- Head trauma
- CNS tumors and treatment (radiotherapy, surgery)
- Infiltrative diseases (hemochromatosis, sarcoidosis, histiocytosis)
- Infections
Note: Functional HH is more common in girls than boys.
4.5 Permanent Hypogonadotropic Hypogonadism
Congenital causes (genetic):
| Gene/Syndrome | Inheritance | Associated Features |
|---|---|---|
| ANOS1 (KAL1) - Kallmann syndrome | X-linked | Anosmia, renal agenesis, synkinesia, cleft palate |
| NELF | AR | Anosmia |
| FGF8 / FGFR1 | AR | Anosmia (some normosmic) |
| PROK2 / PROK2R | AR | Hypogonadism + anosmia |
| CHD7 | AD | CHARGE syndrome (coloboma, heart defect, choanal atresia, growth retardation, genital abnormalities, ear anomalies) |
| KISS1 / KISS1R | AR | Normosmic IHH |
| TAC3 / TACR3 | AR | Normosmic IHH |
| GNRH1 / GNRHR | AR | Isolated GnRH deficiency |
- Kallmann syndrome = congenital HH + anosmia (failure of GnRH neuron migration from olfactory placode)
- 10-20% of those with congenital HH may experience spontaneous restoration of GnRH secretion in adulthood
Acquired causes:
- Pituitary tumors (craniopharyngioma, prolactinoma)
- Post-irradiation
- Trauma, surgery
- Panhypopituitarism - presents with delayed puberty + growth failure + hypothyroidism + adrenal insufficiency
4.6 Primary Gonadal Failure (Hypergonadotropic Hypogonadism)
High FSH and LH (pituitary trying to compensate) + low sex steroids.
Causes in girls:
- Turner syndrome (45,X) - most common cause of hypergonadotropic hypogonadism in girls
- Autoimmune oophoritis
- Chemotherapy/irradiation
- Gonadal dysgenesis
Causes in boys:
- Klinefelter syndrome (47,XXY) - most common
- Bilateral cryptorchidism (untreated)
- Orchitis (viral - mumps)
- Chemotherapy/irradiation
- Anorchia
4.7 Evaluation of Delayed Puberty
History:
- Growth patterns since birth
- Presence of any secondary sexual development
- Diet and exercise habits
- Systemic illnesses
- Neurologic symptoms (headaches, visual changes)
- Family history of delayed puberty
- Psychosocial history
Physical Examination:
- Height, weight, arm span (arm span >5 cm above height suggests eunuchoid configuration - delayed epiphyseal closure from hypogonadism)
- Visual fields
- Hair growth pattern, testicular volume, phallic size, scrotal reddening
- Tanner staging
Investigations:
- Bone age (left wrist X-ray) - delayed in constitutional delay
- CBC, ESR, liver function tests
- FSH, LH, testosterone/estradiol, DHEA-S, prolactin
| Pattern | Interpretation |
|---|---|
| Low FSH, LH + Low sex steroids | Hypogonadotropic hypogonadism (constitutional, functional, or permanent) |
| High FSH, LH + Low sex steroids | Hypergonadotropic hypogonadism (primary gonadal failure) |
| Normal prepubertal levels | Constitutional delay (most likely if family history positive) |
- MRI pituitary/hypothalamus if hypogonadotropic HH suspected
- Karyotype if Turner or Klinefelter suspected
- GnRH stimulation test to differentiate constitutional delay from permanent HH (though not perfectly discriminatory)
4.8 Treatment of Delayed Puberty
Constitutional delay (self-limited):
- Reassurance is appropriate for many - puberty will occur eventually
- Consider impact on social relationships and school performance
- Boys: If treatment desired:
- Testosterone enanthate or cypionate 25-50 mg IM every 2-4 weeks
- OR testosterone patch 2.5 mg / testosterone gel 25 mg
- Interrupt after 6 months to check if endogenous puberty has started
- Consider aromatase inhibitors co-administration to improve final height (testosterone aromatizes to estrogen which drives epiphyseal closure)
- Girls: Low-dose estrogen to initiate puberty
Permanent hypogonadotropic HH:
- Earlier hormone treatment required
- Boys: hCG therapy to induce testicular development and spermatogenesis
- Long-term testosterone replacement
- For fertility: pulsatile GnRH therapy or gonadotropin therapy (FSH + hCG)
Primary gonadal failure:
- Long-term sex hormone replacement
- Turner syndrome: estrogen replacement + GH therapy
- Klinefelter: testosterone replacement
PART 5: SUMMARY TABLE - ABNORMAL PUBERTY AT A GLANCE
| Condition | Timing | Gonadotropins | Sex Steroids | Bone Age | Key Cause |
|---|---|---|---|---|---|
| Central precocious puberty | Early (<8F/<9M) | Elevated (LH, FSH) | Elevated | Advanced | Idiopathic, CNS lesion |
| Peripheral precocious puberty | Early | Low/suppressed | Elevated | Advanced | CAH, McCune-Albright, tumor |
| Constitutional delay | Late | Low (prepubertal) | Low (prepubertal) | Delayed | Familial; GnRH delay |
| Functional HH | Late | Low | Low | Delayed | Anorexia, chronic disease |
| Permanent HH (Kallmann etc.) | Late | Low | Low | Delayed | GnRH neuron defect |
| Primary gonadal failure | Late | Elevated | Low | Delayed | Turner, Klinefelter, gonadal injury |
PART 6: CLINICAL PEARLS
- First sign of puberty in girls: Breast bud development (thelarche) - Tanner stage 2
- First sign of puberty in boys: Testicular enlargement >2.5 cm - Tanner stage 2
- Girls reach peak growth velocity at Tanner stage 3 (~8 cm/yr); boys at Tanner stage 4 (~10 cm/yr)
- Gonadotropin pattern distinguishes primary from secondary gonadal failure - high gonadotropins = primary gonadal failure
- Kallmann syndrome = HH + anosmia (smell should always be tested in delayed puberty)
- GnRH agonists paradoxically suppress puberty because continuous (non-pulsatile) GnRH downregulates pituitary receptors
- Children with developmental disabilities have higher incidence of precocious puberty
- McCune-Albright = café-au-lait + polyostotic fibrous dysplasia + peripheral precocious puberty
- Bone age interpretation: advanced in precocious puberty (risk of short adult stature), delayed in constitutional delay (good prognosis for final height)
- Self-limited delayed puberty and congenital HH can look identical early on - longitudinal follow-up is often required to distinguish them
Sources:
- Medical Physiology (Boron & Boulpaep), pp. 1587-1590
- Ganong's Review of Medical Physiology 26th Ed., pp. 401-404
- Harrison's Principles of Internal Medicine 22E (2025), pp. 3152-3154
- Textbook of Family Medicine 9e, pp. 1038-1042
- Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.