Falx cerebri
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete anatomical overview of the falx cerebri, sourced from Gray's Anatomy for Students and the Color Atlas of Human Anatomy Vol. 2.
Falx Cerebri
Definition and Shape
The falx cerebri is a crescent-shaped (sickle-shaped) downward projection of the meningeal layer of dura mater from the dura lining the calvaria. It passes vertically in the longitudinal (interhemispheric) fissure between the two cerebral hemispheres, partially subdividing the cranial cavity.
It is one of four dural partitions:
- Falx cerebri - between the cerebral hemispheres
- Tentorium cerebelli - separates cerebrum from cerebellum
- Falx cerebelli - between the cerebellar hemispheres
- Diaphragma sellae - covers the hypophyseal fossa
Attachments
| Point | Structure |
|---|---|
| Anteriorly | Crista galli of ethmoid bone + frontal crest of frontal bone |
| Posteriorly | Blends with and attaches to the tentorium cerebelli |
| Superiorly | Inner surface of the calvaria (midline, from frontal to occipital bone) |
| Inferior border | Free edge (concave), arches over the corpus callosum |
Associated Dural Venous Sinuses
The falx cerebri houses two major dural venous sinuses:
| Sinus | Location | Drains Into |
|---|---|---|
| Superior sagittal sinus | Superior (convex) border of falx cerebri | Confluence of sinuses |
| Inferior sagittal sinus | Inferior (free/concave) border of falx cerebri | Straight sinus |
| Straight sinus | Junction of falx cerebri and tentorium cerebelli | Confluence of sinuses |
The straight sinus also receives the great cerebral vein (of Galen) and veins from the falx cerebri itself.
Diagrams
Dural partitions (diagram + cadaveric dissection):
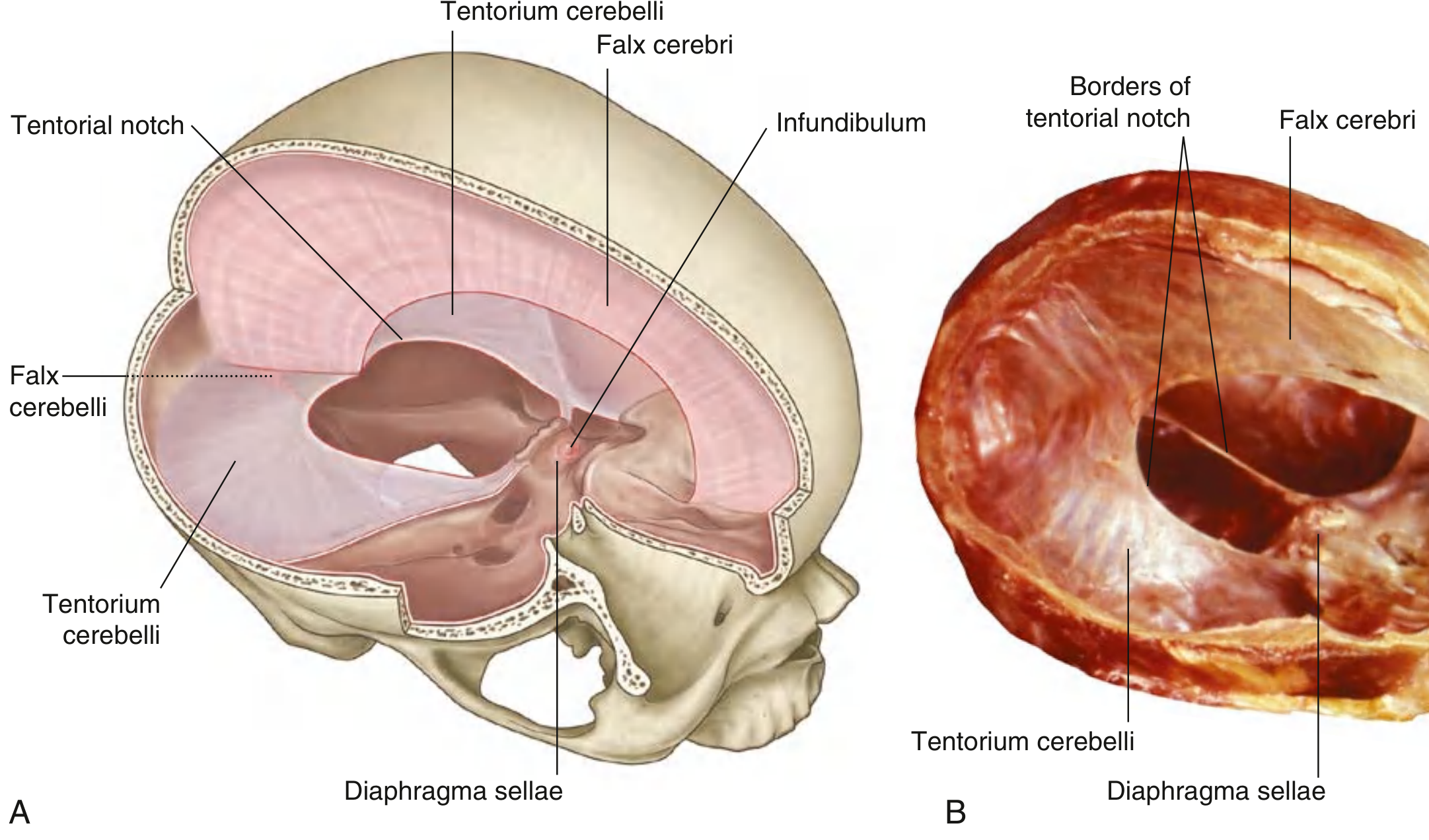
Gray's Anatomy for Students, Fig. 8.32 - Dural Partitions
Dural venous sinuses:
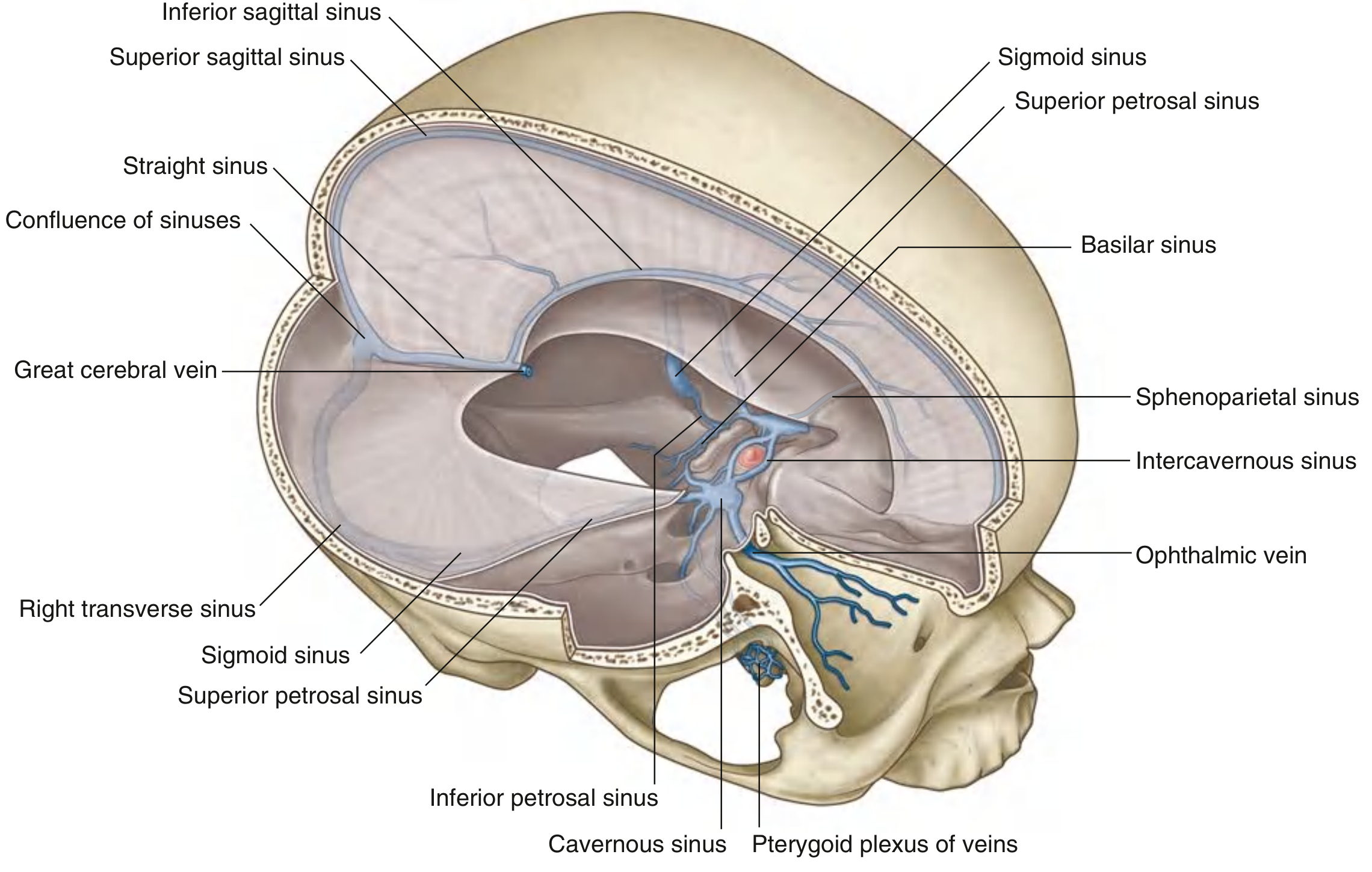
Gray's Anatomy for Students, Fig. 8.46 - Veins, Meninges, and Dural Venous Sinuses
Clinical Relevance
-
Subfalcine herniation - The cingulate gyrus is forced under the inferior free edge of the falx cerebri when a unilateral supratentorial mass displaces the hemisphere medially. This can compress the anterior cerebral artery, causing contralateral leg weakness.
-
Subdural abscess - An abscess can be confined to one side of the falx cerebri (the falx acts as a barrier), distinguishing it from epidural or subarachnoid spread.
-
Falcine meningioma - Meningiomas arising from the falx cerebri grow between the hemispheres and can compress the medial frontal lobes bilaterally, causing lower limb weakness.
-
Calcification of the falx - A normal age-related finding on CT; however, abnormal patterns can be seen in conditions like Gorlin syndrome (basal cell nevus syndrome), where extensive falx calcification is one of the major diagnostic criteria.
-
Skull base surgery - During anterior skull base approaches, the attachment of the falx cerebri to the crista galli must be divided with scissors before the anterior cranial base can be mobilized (as noted in K.J. Lee's Essential Otolaryngology).
Sources: Gray's Anatomy for Students (9780323934237); Color Atlas of Human Anatomy Vol. 2, Internal Organs (9783132424487); Neuroanatomy through Clinical Cases 3rd Edition (9781605359625); K.J. Lee's Essential Otolaryngology (9781260122237)
What is... Oculogeric muscles.
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a complete overview of the extraocular (oculogeric) muscles, sourced from Neuroanatomy through Clinical Cases, 3rd Edition.
Extraocular (Oculomotor) Muscles
These are the six striated muscles that move each eyeball within the orbit. They also include the levator palpebrae superioris (not strictly an extraocular muscle but closely associated).
All six muscles originate from the common tendinous ring (annulus of Zinn) at the orbital apex, except:
- The inferior oblique - originates from the anterior medial orbital wall
- The superior oblique - originates from the sphenoid bone in the posterior medial orbit
The Six Extraocular Muscles
| Muscle | Primary Action | Secondary Action | Innervation |
|---|---|---|---|
| Lateral rectus | Abduction (temporal gaze) | - | CN VI (Abducens) |
| Medial rectus | Adduction (nasal gaze) | - | CN III (Oculomotor) |
| Superior rectus | Elevation | Intorsion | CN III (Oculomotor) |
| Inferior rectus | Depression | Extorsion | CN III (Oculomotor) |
| Superior oblique | Depression + Intorsion | (depression increases with adduction) | CN IV (Trochlear) |
| Inferior oblique | Elevation + Extorsion | (elevation increases with adduction) | CN III (Oculomotor) |
Mnemonic - LR6SO4 (rest CN3): Lateral Rectus = CN VI, Superior Oblique = CN IV, all others = CN III.
Diagram - Rectus Muscles and Their Actions
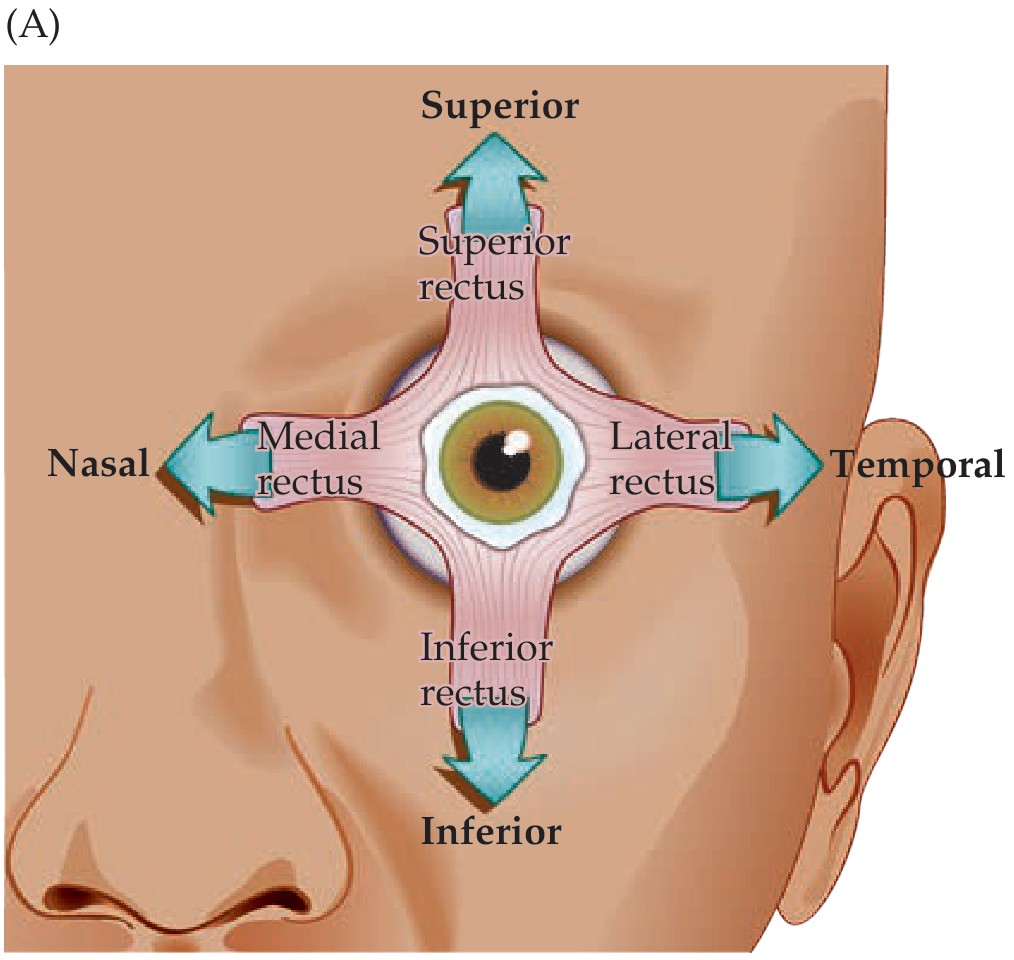
Neuroanatomy through Clinical Cases, Fig. 13.1A - Rectus muscles
Oblique Muscles - Special Features
The obliques produce torsional movements (rotation of the eye about its axis):
- Superior oblique passes through the trochlea (a fibrous pulley on the medial superior orbital rim), then curves back to insert on the superior surface of the globe. It produces intorsion (upper pole of eye rotates inward/nasally).
- Inferior oblique has no trochlea. It inserts on the inferior surface of the globe and produces extorsion (upper pole of eye rotates outward/temporally).
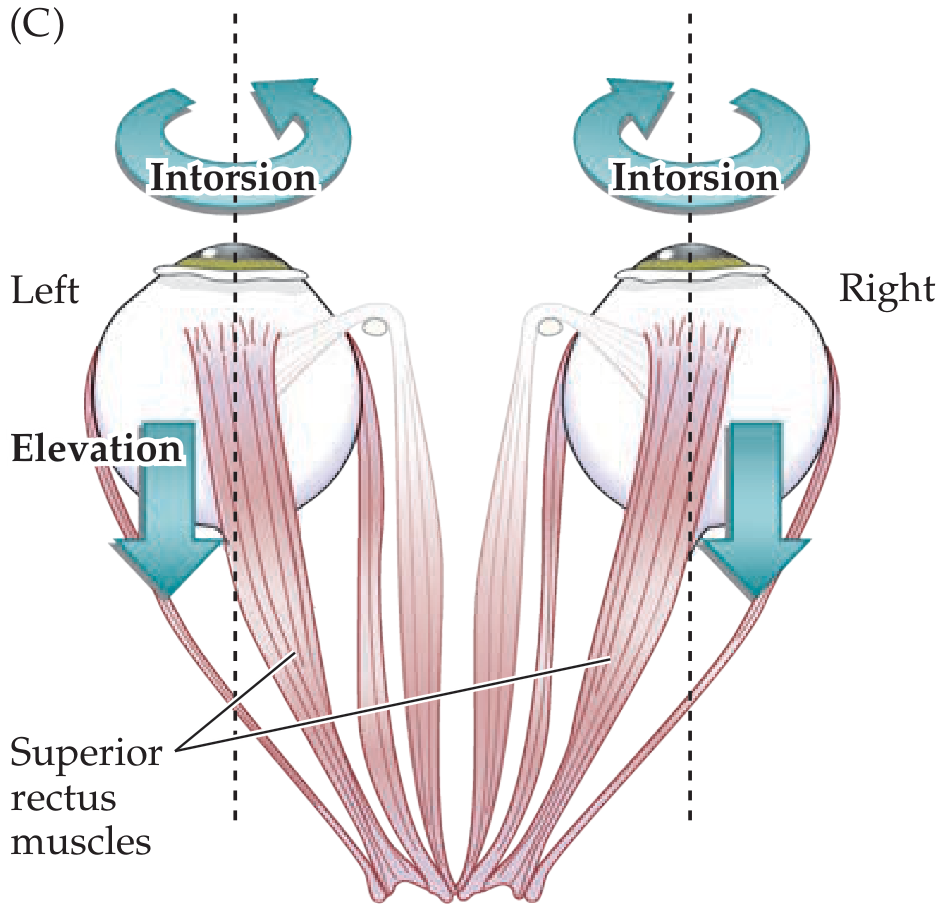
Neuroanatomy through Clinical Cases, Fig. 13.1C - Dual actions of superior rectus
Innervating Nerves and Their Paths
All three cranial nerves (CN III, IV, VI) travel through the cavernous sinus and enter the orbit via the superior orbital fissure.
CN III (Oculomotor) splits into two divisions in the orbit:
- Superior division - superior rectus + levator palpebrae superioris
- Inferior division - medial rectus, inferior rectus, inferior oblique + preganglionic parasympathetic fibers to the pupillary constrictor and ciliary muscle
CN IV (Trochlear) - exits the brainstem dorsally (unique among cranial nerves), crosses the midline, and innervates the contralateral superior oblique.
CN VI (Abducens) - long intracranial course; innervates the lateral rectus.
Brainstem Nuclei
| Nerve | Nucleus Location |
|---|---|
| CN III | Upper midbrain, level of superior colliculi, ventral to periaqueductal gray |
| CN IV | Lower midbrain, level of inferior colliculi |
| CN VI | Pons (near the floor of the 4th ventricle) |
The Edinger-Westphal nucleus sits dorsal to the CN III nucleus and carries preganglionic parasympathetics for pupil constriction and lens accommodation.
Additional Eye Muscles (Not Strictly Extraocular)
| Muscle | Action | Innervation |
|---|---|---|
| Levator palpebrae superioris | Elevates upper eyelid | CN III (superior division) |
| Pupillary constrictor | Miosis | CN III (parasympathetic via ciliary ganglion) |
| Pupillary dilator | Mydriasis | Sympathetic (superior cervical ganglion) |
| Ciliary muscle | Lens accommodation (thickens lens) | CN III (parasympathetic) |
Clinical Pearls
| CN | Palsy Findings |
|---|---|
| CN III palsy | "Down and out" eye (unopposed lateral rectus + superior oblique), ptosis, fixed dilated pupil (if nerve compressed - e.g., PCA aneurysm) |
| CN IV palsy | Vertical diplopia, eye excyclotorted; patient tilts head to compensate; causes difficulty descending stairs |
| CN VI palsy | Medial deviation of eye (esotropia), inability to abduct; most common CN palsy; can be a false localizing sign in raised ICP |
Sources: Neuroanatomy through Clinical Cases, 3rd Edition (9781605359625)
Uh, names of the sutures present on the skull.
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete overview of the sutures of the skull, sourced from Gray's Anatomy for Students and the Color Atlas of Human Anatomy Vol. 1.
Skull Sutures
Sutures are fibrous joints (synarthroses) between the flat bones of the skull. They allow slight movement in infancy and fetal life, then ossify progressively with age.
Superior View - The Three Major Sutures
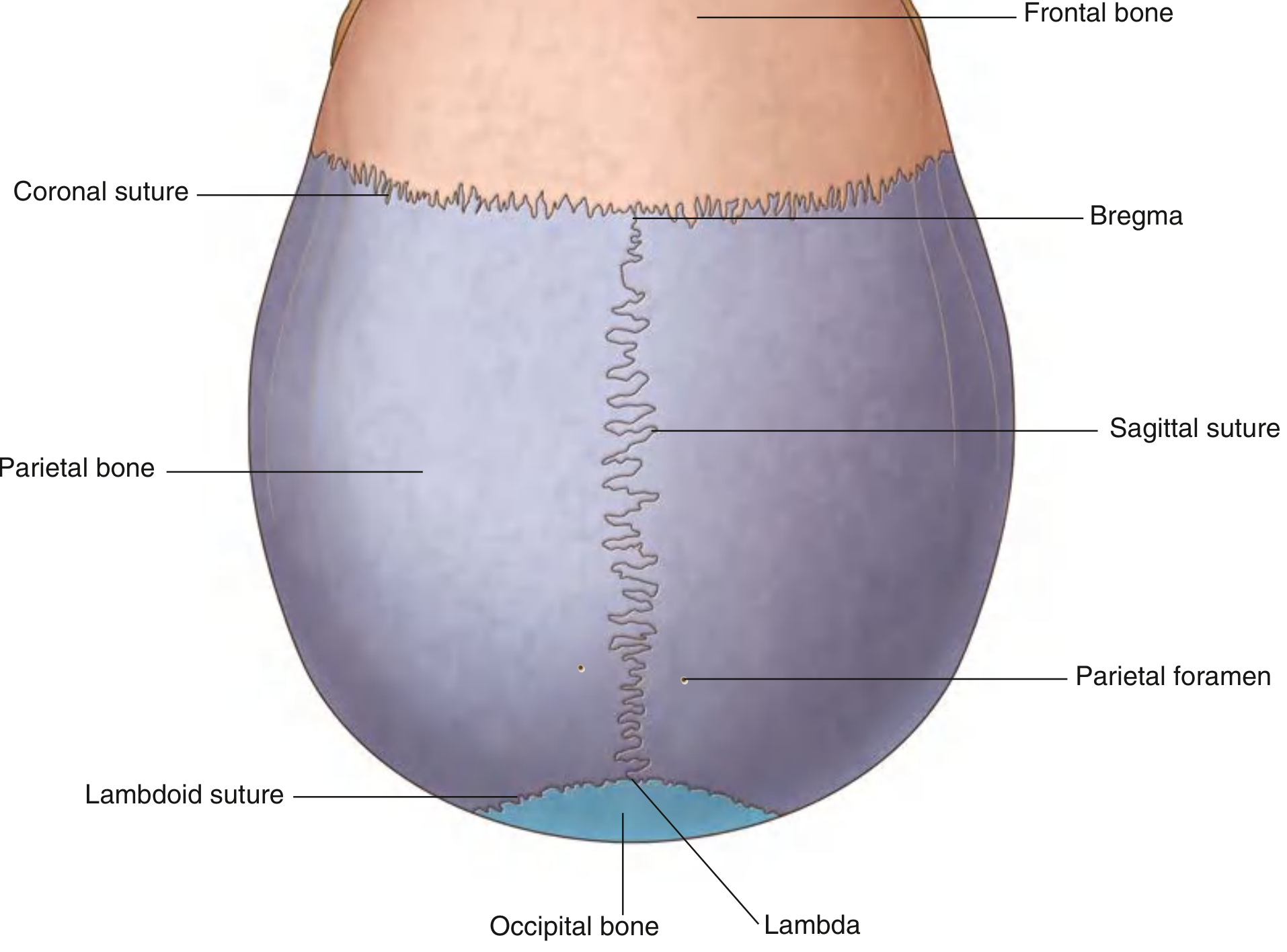
Gray's Anatomy for Students, Fig. 8.21 - Superior View of the Skull
| Suture | Bones Joined | Orientation |
|---|---|---|
| Coronal suture | Frontal + two parietal bones | Transverse (coronal plane) |
| Sagittal suture | Right parietal + left parietal bone | Midline anteroposterior |
| Lambdoid suture | Two parietal bones + occipital bone | Posterior, shaped like the Greek letter lambda (Λ) |
Lateral View - Additional Sutures
| Suture | Bones Joined | Notes |
|---|---|---|
| Squamous suture | Parietal + temporal bone | Curved, on the lateral skull |
| Sphenofrontal suture | Sphenoid (greater wing) + frontal bone | Anterior cranial fossa region |
| Sphenosquamosal suture | Sphenoid (greater wing) + temporal bone (squamous part) | Lateral skull |
| Sphenoparietal suture | Sphenoid (greater wing) + parietal bone | - |
| Parietomastoid suture | Parietal + mastoid part of temporal bone | Posterior lateral skull |
| Occipitomastoid suture | Occipital + mastoid part of temporal bone | Posterior lateral skull |
| Metopic suture | Right frontal + left frontal bone | Midline of frontal bone; normally fuses by age 2 |
Key Junctions (Landmarks)
| Junction | Sutures Meeting | Significance |
|---|---|---|
| Bregma | Coronal + sagittal sutures | Site of the anterior fontanelle in infants |
| Lambda | Sagittal + lambdoid sutures | Site of the posterior fontanelle in infants |
| Pterion | Frontal + parietal + greater wing of sphenoid + temporal bones | Thinnest part of skull; deep to it lies the middle meningeal artery - fracture here causes extradural hematoma |
| Asterion | Lambdoid + occipitomastoid + parietomastoid sutures | Overlies junction of transverse and sigmoid sinuses on inner surface; key landmark for posterior fossa surgery |
Fontanelles (in Newborns)
Before the sutures fuse, the gaps between bones are covered by fibrous membrane - these are the fontanelles:
| Fontanelle | Location | Closure |
|---|---|---|
| Anterior (bregmatic) | At bregma | Closes ~18 months after birth |
| Posterior (lambdoid) | At lambda | Closes ~2-3 months after birth |
| Anterolateral (sphenoidal) | At pterion region | Closes ~3 months |
| Posterolateral (mastoid) | At asterion region | Closes ~1 year |
The anterior fontanelle can be palpated in infants - it bulges with raised intracranial pressure and is sunken in dehydration.
Clinical Relevance - Craniosynostosis
Premature fusion of individual sutures produces characteristic skull deformities:
| Suture Fused Early | Deformity | Shape |
|---|---|---|
| Sagittal | Scaphocephaly | Narrow, boat-shaped (most common) |
| Coronal | Brachycephaly | Short, broad forehead |
| Metopic | Trigonocephaly | Triangular forehead ("bird's eye" view) |
| Lambdoid | Posterior plagiocephaly | Asymmetric flattening of posterior skull |
Sources: Gray's Anatomy for Students (9780323934237); Color Atlas of Human Anatomy Vol. 1 (9783132424432); Bailey and Love's Short Practice of Surgery 28th Ed. (9780367548117)
Name the cranium bones
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a complete overview of the bones of the cranium, sourced from Forensic Anthropology: A Comprehensive Introduction and Rosen's Emergency Medicine.
Bones of the Cranium
The cranium = the skull minus the mandible. It has 8 bones total (the neurocranium), divided into the cranial vault and cranial base.
"Bones of the calvaria are 8 in number: parietal 2, frontal 1, temporal 2, occipital 1, sphenoid 1, and ethmoid 1."
- The Essentials of Forensic Medicine and Toxicology, 36th Edition
Color-coded Lateral View
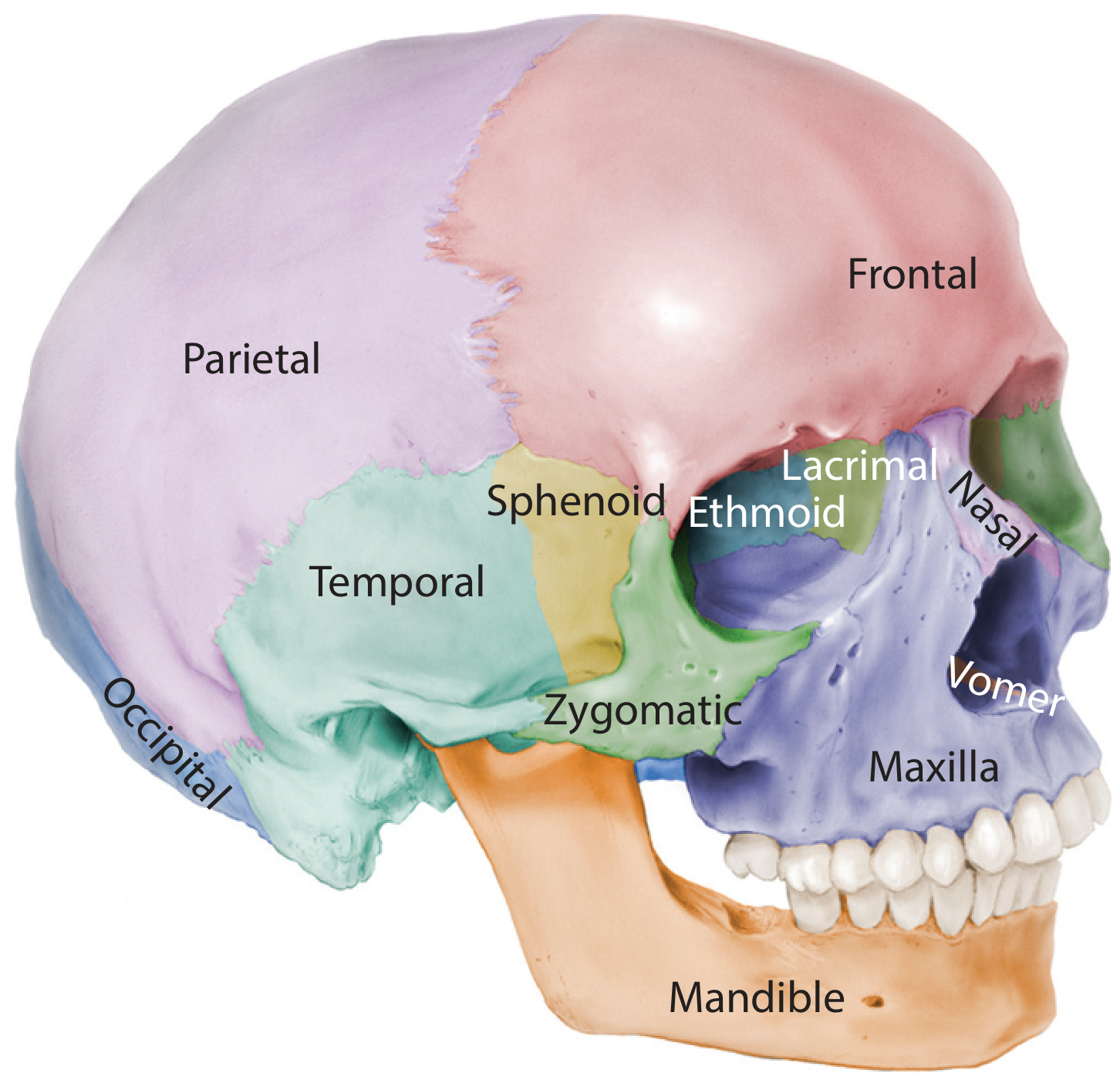
Forensic Anthropology: A Comprehensive Introduction, Fig. 5.9b - Bones of the Skull
The 8 Cranial Bones
| # | Bone | Count | Location | Key Features |
|---|---|---|---|---|
| 1 | Frontal | 1 (unpaired) | Anterior cranium; forehead + roof of orbits | Supraorbital margins, frontal sinuses, frontal crest (attachment of falx cerebri) |
| 2 | Parietal | 2 (paired) | Superior and lateral walls of the skull vault | Temporal lines, parietal foramina; articulate at sagittal suture |
| 3 | Temporal | 2 (paired) | Inferolateral skull | Contains the petrous part (houses inner ear - incus, malleus, stapes), mastoid process, styloid process, external acoustic meatus, TMJ |
| 4 | Occipital | 1 (unpaired) | Posterior and base of skull | Foramen magnum, occipital condyles (articulate with C1 atlas), external occipital protuberance, internal occipital crest |
| 5 | Sphenoid | 1 (unpaired) | Central skull base; "keystone bone" | Greater and lesser wings, sella turcica (houses pituitary), pterygoid processes, optic canals, foramen rotundum, foramen ovale |
| 6 | Ethmoid | 1 (unpaired) | Anterior cranial base; between orbits | Cribriform plate (CN I passes through), crista galli (attachment of falx cerebri), perpendicular plate (nasal septum), ethmoid air cells |
How to Remember Them
Mnemonic - "Pretty Fancy Old Skull, Expect To Find":
Parietal, Frontal, Occipital, Sphenoid, Ethmoid, Temporal, Frontal
Simpler: "PEST OF" - Parietal (×2), Ethmoid, Sphenoid, Temporal (×2), Occipital, Frontal
How They Fit Together
FRONTAL
_____|_____|_____
| Coronal suture |
| PARIETAL | PARIETAL| ← Sagittal suture runs between them
|__________|_________|
Lambdoid suture
OCCIPITAL
Laterally: TEMPORAL (with squamosal suture)
Base: SPHENOID + ETHMOID (anterior base)
Key Clinical Notes
- The temporal bone is the thinnest bone of the skull; the petrous part is the densest bone in the body
- The sphenoid is called the "keystone" of the cranial base - it articulates with all other cranial bones
- The ethmoid's cribriform plate is very fragile - fractures here cause CSF rhinorrhoea (cerebrospinal fluid leaking from the nose)
- The occipital condyles articulate with the atlas (C1) at the atlanto-occipital joint, allowing nodding movements
Sources: Forensic Anthropology: A Comprehensive Introduction, 2nd Ed. (9781498736121); Rosen's Emergency Medicine (9780323757898); The Essentials of Forensic Medicine and Toxicology, 36th Ed. (9789366165257)
This is a shared conversation. Sign in to Orris to start your own chat.