Why big placenta in rh negative pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
Rh isoimmunization placenta hydrops fetalis pathophysiology
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Now I have everything needed for a complete answer. Let me compile it.
Why the Placenta is Large in Rh-Negative Pregnancy (with Rh Sensitization)
The enlarged placenta in an Rh-negative mother sensitized to an Rh-positive fetus is a direct result of placental hydrops - fluid accumulation and edema within the placental villi, driven by the cascade below.
Step-by-Step Pathogenesis
1. Sensitization of the Rh-negative mother
In a prior pregnancy or transfusion, fetal Rh+ red cells entered the maternal circulation, triggering antibody production. The first response is IgM (does not cross the placenta). Subsequent exposure produces IgG antibodies, which cross the placenta freely.
2. Fetal red cell destruction (hemolysis)
Maternal IgG anti-D antibodies coat the fetal Rh+ red cells. Phagocytes destroy these antibody-coated cells, causing progressive fetal hemolytic anemia.
3. Fetal anemia leads to two major problems:
| Pathway | Consequences |
|---|---|
| Severe anemia | Hypoxic injury to liver and heart |
| Liver injury | Reduced plasma protein synthesis (albumin drops to ~2-2.5 g/dL) |
| Cardiac hypoxia | Cardiac decompensation and heart failure |
| Low oncotic pressure + high hydrostatic pressure (heart failure) | Generalized edema, anasarca, hydrops fetalis |
4. The placenta becomes large and edematous
The same forces that cause generalized fetal edema - reduced plasma oncotic pressure and elevated hydrostatic pressure from heart failure - cause fluid to accumulate in the placental tissue. The villi become edematous and hydropic, making the placenta:
- Large (increased weight and volume)
- Pale (diluted by edema fluid)
- Bulky and waterlogged
This appearance is described as hydrops of the placenta, and it mirrors the hydrops fetalis seen in the fetus.
The Pathogenesis Diagram
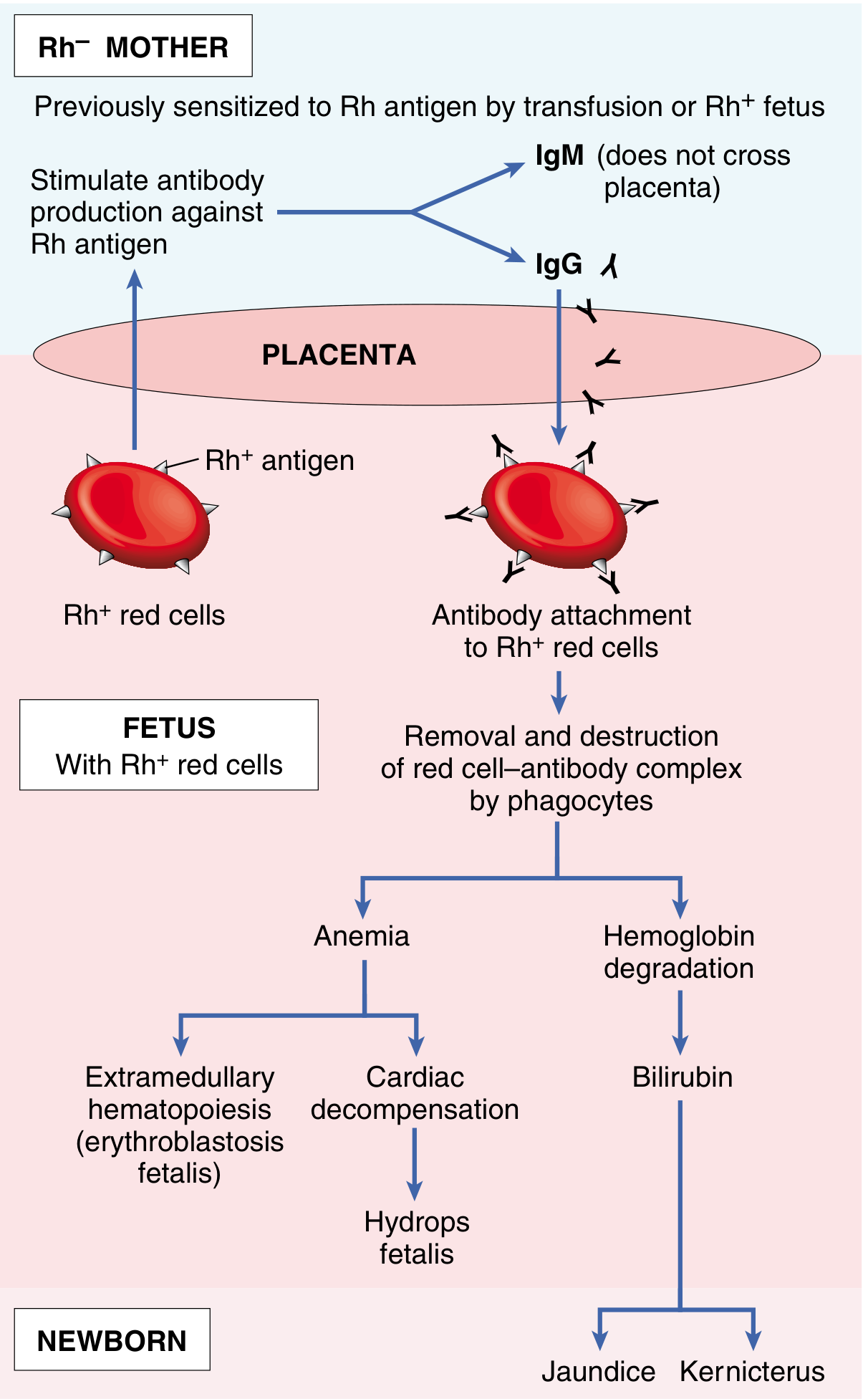
Fig. 10.10 - Pathogenesis of immune hydrops fetalis (Robbins Pathologic Basis of Disease)
Summary
Rh sensitization → maternal IgG crosses placenta → fetal hemolysis → fetal anemia → cardiac failure + hypoalbuminemia → ↑ hydrostatic pressure + ↓ oncotic pressure → fluid extravasation into placenta and fetus → large, pale, edematous (hydropic) placenta
The enlarged placenta is therefore not a primary event - it is a secondary consequence of severe fetal anemia and the resulting hemodynamic failure (hydrops fetalis).
Additional Notes
- This was the most common cause of immune hydrops historically; anti-D (RhIG) prophylaxis at 28 weeks gestation and within 72 hours of delivery has dramatically reduced its incidence.
- The fetus also shows hepatosplenomegaly (from extramedullary hematopoiesis as the marrow tries to compensate), circulating erythroblasts (erythroblastosis fetalis), and jaundice/kernicterus from bilirubin accumulation.
- Today, non-immune hydrops (chromosomal anomalies, structural cardiac defects, parvovirus B19, α-thalassemia) is more common than immune hydrops.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 436-437
This is a shared conversation. Sign in to Orris to start your own chat.