Turners syndrome
Reading File
Finding Sources
Searching PubMed
"Turner syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Robbins & Kumar. Let me compile the full answer.
Turner Syndrome
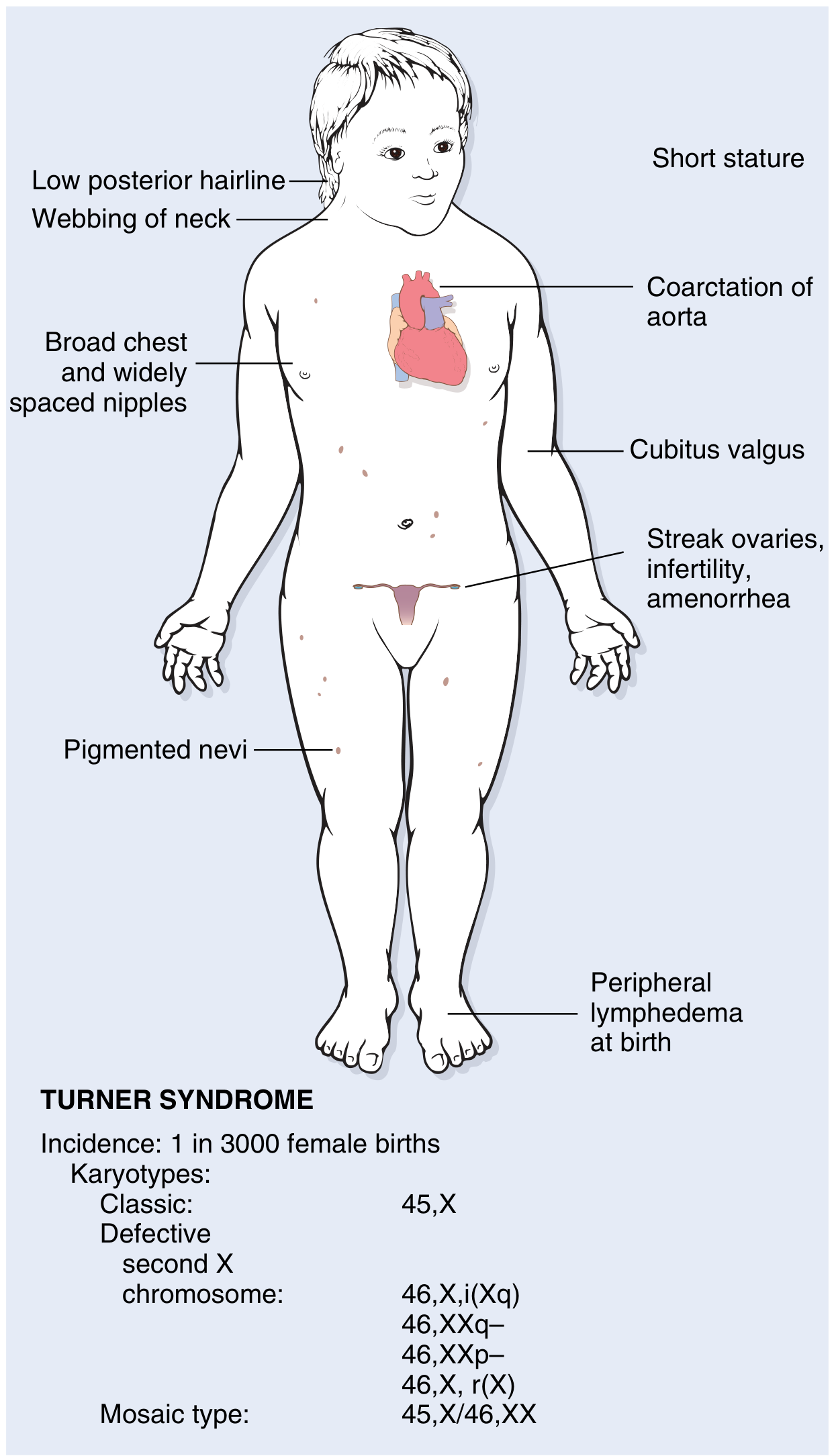
Fig. 4.20 - Clinical features and karyotypes of Turner syndrome (Robbins & Kumar Basic Pathology)
Definition
Turner syndrome is characterized by primary hypogonadism in phenotypic females, resulting from complete or partial monosomy of the X chromosome. It is the most common sex chromosome abnormality in females.
- Incidence: approximately 1 in 2,000-3,000 live-born females
- Only ~1% of monosomy X embryos survive to birth; the 45,X karyotype accounts for ~18% of all chromosomally abnormal spontaneous abortions
Karyotypes
| Type | Karyotype | Frequency |
|---|---|---|
| Classic | 45,X | ~57% |
| Isochromosome of long arm | 46,X,i(Xq10) - loss of short arm | Most common structural variant |
| Ring chromosome | 46,X,r(X) - deletion of both long and short arm portions | Less common |
| Short/long arm deletion | 46,X,del(Xp) or 46,X,del(Xq) | Less common |
| Mosaic | 45,X/46,XX; 45,X/46,XY; 45,X/47,XXX | ~29% |
Key point: 5-10% of patients have Y chromosome sequences (e.g., 45,X/46,XY). These patients carry a significantly elevated risk of gonadoblastoma and require prophylactic gonadectomy.
The true prevalence of mosaicism may be as high as 75% when more sensitive techniques are used. Patients with a higher proportion of 45,X cells have a more severe phenotype; those with detectable 45,X/46,XX mosaicism may appear nearly normal and present only with primary amenorrhea.
Pathogenesis
- In ~80% of cases, the X chromosome retained is maternal in origin, implying an error in paternal gametogenesis (absent or defective sperm contributes most errors).
- The fetal ovaries develop normally up to ~18 weeks of gestation, but the absence of the second X leads to accelerated oocyte attrition, complete by age 2 years - effectively "menopause before menarche."
- SHOX gene (at Xp22.33, pseudoautosomal region, escapes X inactivation): haploinsufficiency of SHOX is responsible for short stature. Normally, both males and females have two copies. SHOX is expressed in the growth plates of long bones (radius, ulna, tibia, fibula).
- Genes on the short arm largely determine somatic features; genes on the long arm influence fertility and menstruation.
Clinical Features
At Birth / Infancy
- Peripheral lymphedema of dorsum of hands and feet (due to lymph stasis)
- Cystic hygroma - markedly distended lymphatic channels at the nape of neck, later manifests as neck webbing
- Congenital heart disease in 25-50% of patients
Somatic Features (Childhood onward)
- Short stature (below 3rd percentile) - most consistent feature
- Webbed neck (pterygium colli) with low posterior hairline
- Shield chest with broad thorax and widely spaced nipples
- Cubitus valgus (increased carrying angle of the arms)
- High-arched palate
- Pigmented nevi
- Horseshoe kidney
Cardiovascular (most common cause of death in childhood)
- Preductal coarctation of the aorta (most common cardiac lesion)
- Bicuspid aortic valve
- Aortic root dilation in ~30% of cases
- 100-fold increased risk of aortic dissection
- ~5% of young females initially diagnosed with coarctation of the aorta have Turner syndrome
Reproductive / Endocrine (Adolescence/Adulthood)
- Primary amenorrhea (most common presenting complaint in adults)
- Failure to develop secondary sexual characteristics at puberty
- Infantile external genitalia, minimal breast development, sparse pubic hair
- Streak ovaries - bilateral fibrous white strands devoid of follicles and ova (result of oocyte attrition)
- Infertility (a very small number of mosaic patients can conceive)
Other Systemic Associations
- Autoimmune hypothyroidism - antithyroid autoantibodies are common; up to 50% of patients (especially those with isochromosome Xp) develop clinical hypothyroidism
- Glucose intolerance, insulin resistance, obesity, non-alcoholic fatty liver disease - a subset develops full metabolic syndrome
- Subtle deficits in visuospatial information processing - overall intellect is generally within normal limits
- Sensorineural hearing loss (noted in ENT literature)
Diagnosis
- Short stature + primary amenorrhea in an adolescent/adult female - strong clinical suspicion
- Karyotype (peripheral blood lymphocytes) - confirmatory
- Prenatal: detected on maternal serum screening (elevated hCG, low estriol) or fetal ultrasound (cystic hygroma, nuchal translucency, hydrops, cardiac defects)
- FISH or array CGH for detecting mosaicism or structural rearrangements with Y material
Management
| Problem | Treatment |
|---|---|
| Short stature | Recombinant growth hormone (GH) therapy (started early in childhood); note: GH worsens insulin resistance |
| Hypogonadism / puberty induction | Estrogen replacement (low-dose estrogen at ~12-13 years, then cyclical estrogen/progesterone) |
| Fertility | Not typically achievable without donor oocytes + IVF |
| Cardiovascular | Echocardiography screening; surgical correction of coarctation; aortic surveillance (MRI) |
| Hypothyroidism | Levothyroxine supplementation |
| Y-chromosome material | Prophylactic gonadectomy to prevent gonadoblastoma |
| Psychological | Support for identity, peer relationships, and body image issues |
Recent Evidence (2025)
Recent systematic reviews add important updates:
- A 2025 meta-analysis (PMID 40557696) confirms the impact of karyotype on congenital heart disease risk in Turner syndrome - structural variants carry different CHD profiles than classic 45,X.
- A 2025 meta-analysis (PMID 41243107) quantifies the global prevalence of autoimmune diseases in Turner syndrome, underscoring the need for systematic autoimmune surveillance.
- A 2025 systematic review (PMID 39743222) on karyotype-phenotype associations in non-mosaic X chromosome structural rearrangements helps predict clinical severity.
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; The Developing Human - Clinically Oriented Embryology
This is a shared conversation. Sign in to Orris to start your own chat.