Side swipe injury etiology mechanism of injury associated injury signs and symptoms and investigations and evaluation treatment explain in detail with appropriate illustrative diagrams and images
sideswipe injury elbow mechanism associated injuries treatment orthopedics
"sideswipe injury" elbow
PMID: 34858714
PMID: 33487856
sideswipe injury elbow "traffic elbow" fracture dislocation classification injuries vascular nerve
https://e-century.us/files/ijbt/11/5/ijbt0135626.pdf
Medical diagram showing sideswipe injury mechanism: a car with a passenger's elbow protruding out of the window being struck by a passing vehicle, with arrows showing direction of impact forces on the elbow and forearm. The diagram shows the arm anatomy including humerus, radius, ulna, and elbow joint with force vectors labeled. Include a second panel showing the resulting injury pattern with fracture-dislocation of the elbow.
Sideswipe Injury (Traffic Elbow / Baby Car Injury)
Definition
Etiology
| Setting | Mechanism |
|---|---|
| Car/bus passenger | Elbow resting on or protruding through an open window, struck by a passing vehicle |
| Driver | Arm resting on the window sill during a side-impact collision |
| Train passenger | Window seat with elbow outside, struck by a fixed object or passing vehicle at a rail crossing (reported by Pandey et al., 2021, PMID 34858714) |
| Tricycle passenger | Limb protrusion struck by a fixed or moving object (can involve the knee rather than the elbow) |
| Mountain/narrow road collisions | Vehicle squeezing through a narrow gap, arm struck against a rock face or another vehicle |
Mechanism of Injury
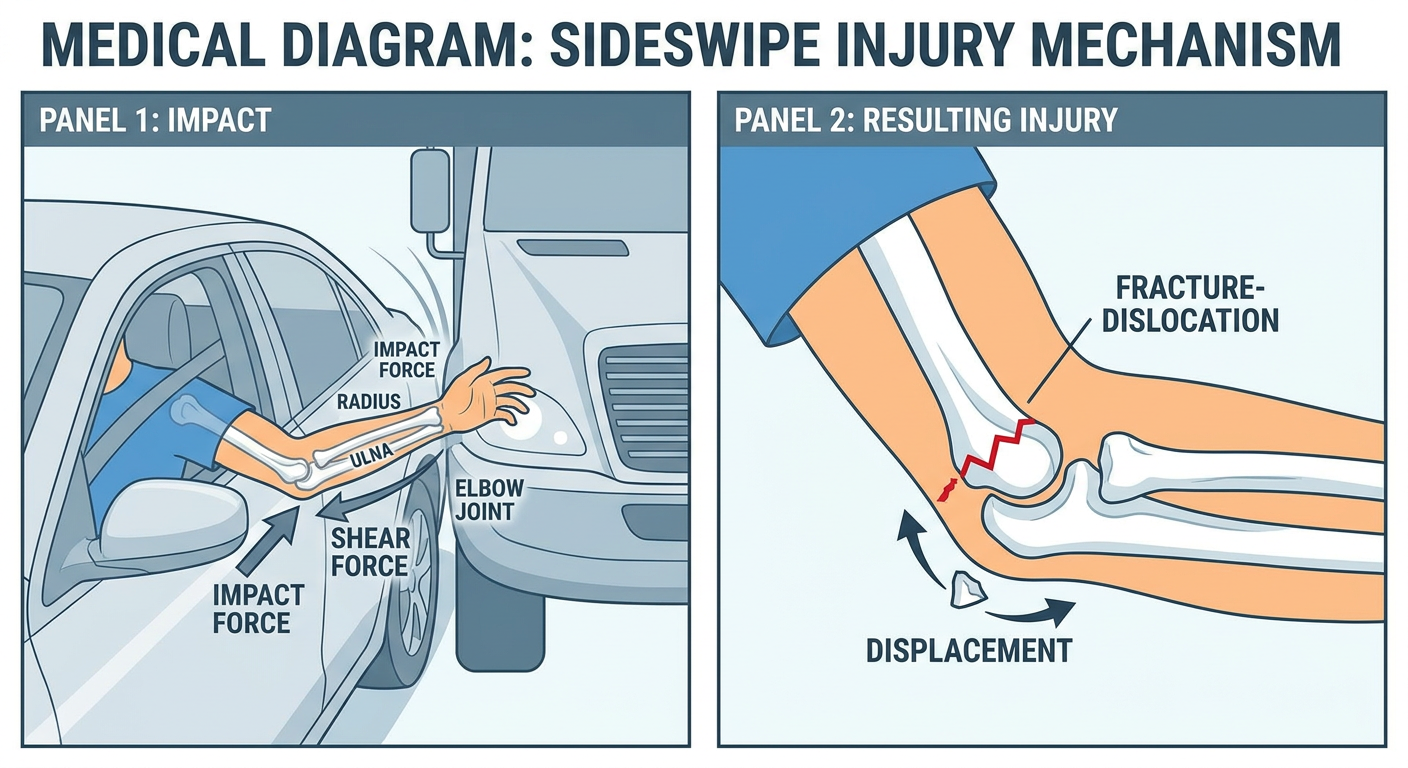
- Direct impact force - a lateral or posterolateral crushing force directed at the elbow region from the striking object
- Shear force - tangential scraping/grinding forces that produce extensive soft tissue stripping and degloving
- Compressive-torsional force - the combination of compression along the forearm axis with a rotational component, accounting for Monteggia-pattern and forearm fractures
- Avulsion force - the momentum of the vehicle can pull tissues off the bone (periosteal stripping, tendon avulsion)
- Open wounds with bone exposure
- Comminuted multi-bone fractures
- Joint dislocation
- Neurovascular injury
- Soft tissue degloving/loss
Elbow Anatomy Relevant to Sideswipe Injury
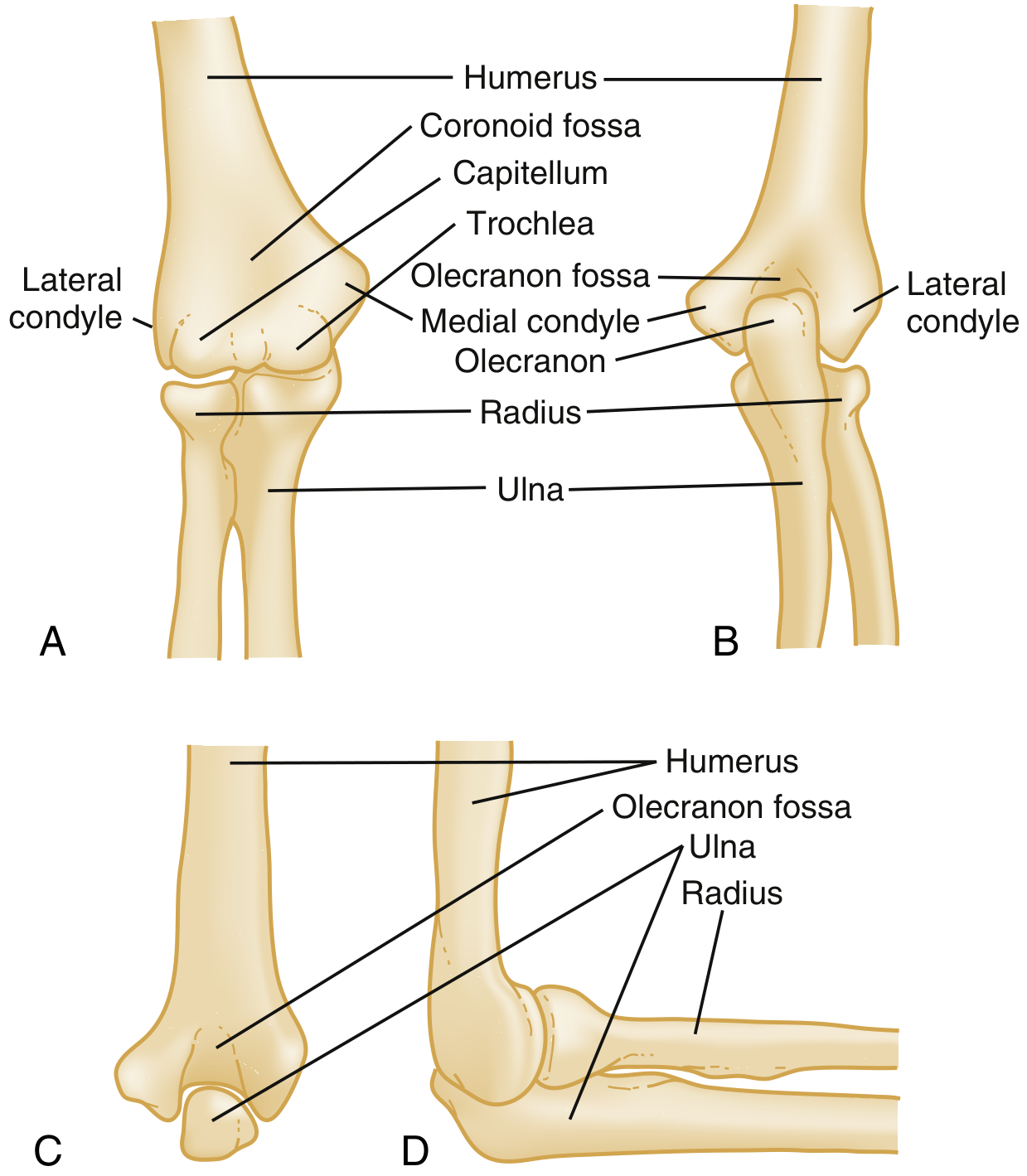
- Distal humerus (condyles, epicondyles, supracondylar region)
- Olecranon and coronoid process of the ulna
- Radial head and neck
- Brachial artery - passes anterior to the elbow joint and is vulnerable to laceration or transection
- Median nerve - runs medial to the brachial artery anteriorly
- Radial nerve / posterior interosseous nerve - passes around the radial neck laterally
- Ulnar nerve - passes posterior to the medial epicondyle in the cubital tunnel
- Brachial plexus - can be injured in very high-energy mechanisms
Associated Injuries
Osseous (Bone) Injuries
| Bone Structure | Injury |
|---|---|
| Distal humerus | Comminuted distal humeral fracture (most common bony injury) |
| Proximal ulna | Olecranon fracture, coronoid fracture, Monteggia fracture-dislocation |
| Radial head/neck | Radial head fracture (part of "terrible triad") |
| Humeral shaft | Shaft fracture (especially at junction of middle and distal thirds) |
| Both forearm bones | Radius + ulna shaft fractures ("both bones forearm") |
Monteggia Fracture-Dislocation
Soft Tissue Injuries
- Degloving injuries of the forearm and elbow (skin stripped off while underlying structures remain)
- Open wounds with exposed bone - Gustilo-Anderson Grade I to Grade III
- Laceration/rupture of the triceps tendon
- Rupture of collateral ligaments (lateral collateral ligament, ulnar collateral ligament)
- Elbow joint capsule disruption
- Compartment syndrome of the forearm
Neurovascular Injuries
| Structure | Injury | Clinical Effect |
|---|---|---|
| Brachial artery | Laceration, transection, intimal tear | Absent radial/ulnar pulse, ischemia, compartment syndrome |
| Radial nerve / PIN | Contusion, laceration, avulsion | Wrist drop, inability to extend fingers/thumb, patchy dorsal hand sensory loss |
| Ulnar nerve | Contusion, laceration | Loss of intrinsic muscle function, small finger sensory loss |
| Median nerve | Contusion, laceration | Thenar wasting, "OK sign" weakness, lateral thumb sensation loss |
| Brachial plexus | Traction avulsion (high energy) | Complete upper limb paralysis (rare) |
Associated Lower Limb Injuries
Signs and Symptoms
Local Examination (Elbow and Upper Limb)
- Open wound with active bleeding
- Exposed bone fragments (open fracture)
- Visible degloving with skin loss
- Deformity of the elbow (may show posterolateral displacement as in fracture-dislocation)
- Swelling and hematoma
- Inability to use the upper limb
- Severe localized pain
- Crepitus over fracture sites
- Loss of normal bony landmarks (in elbow dislocation, the equilateral triangle formed by the two epicondyles and olecranon tip is disrupted)
- Tenderness over the radial head, medial/lateral epicondyles, olecranon
- Inability to flex/extend the elbow
- Inability to pronate/supinate the forearm
- Wrist drop (radial nerve injury)
- Inability to extend MCP joints/thumb (posterior interosseous nerve)
- Patchy sensory changes over the hand
Neurovascular Status (Critical Assessment)
| Nerve | Motor Test | Sensory Test |
|---|---|---|
| Radial nerve | Wrist extension, finger/thumb MCP extension | Dorsum of hand (first web space) |
| Median nerve | "OK sign" (thumb-index pinch), thumb opposition | Lateral palm, thumb, index, middle fingers |
| Ulnar nerve | Finger abduction (small finger), intrinsic grip | Medial palm, ring and small fingers |
- Radial and ulnar pulse palpation (but note: absence may not be apparent if collaterals are maintaining perfusion)
- Capillary refill time
- Hand color and temperature
- Sensation (as paresthesia may indicate ischemia)
Systemic Assessment
- Hemorrhagic shock (open wounds with major vessel involvement)
- Associated thoracic, abdominal injuries (if vehicle occupant in multi-trauma)
Investigations and Evaluation
Imaging
- AP and lateral views of the elbow (mandatory)
- AP lateral view of the entire forearm including wrist (to exclude Monteggia, Galeazzi variants)
- Lateral view of the humerus if shaft fracture suspected
- Findings: fracture lines, dislocation, intra-articular fragments, degree of comminution
- Posterior fat pad sign - indicates hemarthrosis even with subtle fractures
- Anterior fat pad ("sail sign") - also indicates joint effusion
- Disruption of the radiocapitellar line
- CT with 3D reconstruction is essential for:
- Defining fracture pattern precisely
- Identifying coronoid fractures (often missed on plain films)
- Assessing degree of comminution
- Guiding surgical approach and fixation strategy
- Classifying with the Wrightington or OTA/AO classification
- Duplex Doppler ultrasound - non-invasive first-line
- CT Angiography (CTA) - preferred when vascular injury is suspected clinically
- Formal angiography - reserved for cases requiring interventional planning
- Not typically used in the acute setting
- Useful for ligamentous injury assessment if stability is uncertain after initial treatment
Laboratory Investigations
- Full blood count, urea/electrolytes, group and crossmatch
- Coagulation profile
- Injury Severity Score (ISS) documentation
Treatment
Phase 1 - Emergency Resuscitation (On Arrival)
- ATLS protocol - Airway, Breathing, Circulation
- IV antibiotics - Immediate broad-spectrum cover (e.g., cefazolin + metronidazole + aminoglycoside for open fractures)
- Tetanus prophylaxis
- Wound lavage - Copious irrigation of open wounds with normal saline
- Hemorrhage control - Pressure dressings, tourniquet if exsanguinating hemorrhage
- Temporary splintage - Above-elbow posterior splint to immobilize and reduce pain
Phase 2 - Wound Debridement and Fracture Stabilization (Urgent Surgery)
- The priorities are: wound irrigation and debridement, IV antibiotics, tetanus coverage, fracture stabilization, and appropriate soft tissue management (Rockwood and Green's, 10th ed.)
- Contaminated/devascularized bone is excised - EXCEPT when dealing with articular surface fragments, where preservation is preferred to avoid posttraumatic arthritis
| Method | Indication |
|---|---|
| External fixation | Initial stabilization of unstable open fractures, spanning fixator across elbow, allows soft tissue management |
| ORIF with plate and screws | Definitive fixation after soft tissue recovery; distal humerus bicolumnar plating |
| Intramedullary nailing | Humeral shaft fractures |
| Tension band wiring | Olecranon fractures (comminuted = plate preferred) |
| Radial head ORIF or replacement | Radial head fractures depending on fragment size |
| External fixator (hinged) | Complex instability; allows early motion |
- ORIF of the ulna fracture with anatomic restoration of ulnar bow
- Radial head will usually reduce after ulnar fixation; if not, open reduction of radial head required
Phase 3 - Vascular Repair
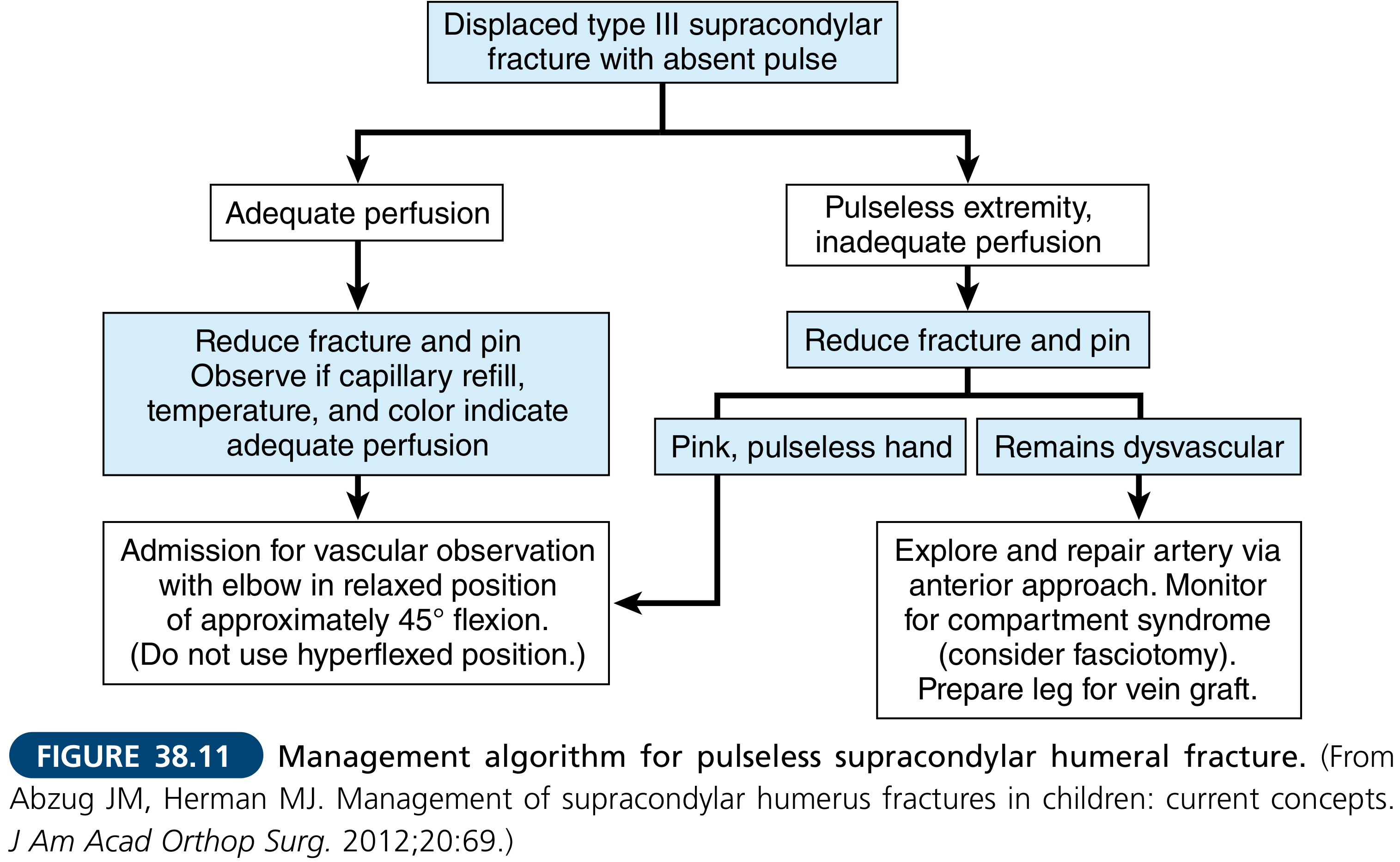
- Brachial artery injury requires urgent vascular surgery consultation
- If hand is pulseless and ischemic after fracture reduction: explore and repair brachial artery via anterior approach with vein graft from the leg
- Collateral circulation may maintain a pink, pulseless hand - this warrants close observation
- Compartment syndrome must be monitored; fasciotomy is performed at low threshold
Phase 4 - Nerve Exploration
- Radial nerve: exploration is performed for established motor deficit (wrist drop, PIN palsy); nerve is explored through posterior or lateral approach
- In Pandey et al.'s series, all four patients underwent radial nerve exploration as part of the staged protocol
- Ulnar and median nerve injuries: primary repair where technically feasible; nerve grafting for segmental loss
- Outcome note: Nerve injury is the most important factor for dismal functional outcomes; only ~25% of ulnar nerve injuries fully recover (Campbell's, 15th ed.)
Phase 5 - Soft Tissue Reconstruction
- Wound closure should not be performed primarily in contaminated injuries
- After debridement, wounds are left open and covered with moist dressings or negative pressure wound therapy (NPWT/VAC)
- Secondary closure at 48-72 hours if wound is clean
- Skin grafting for degloving injuries
- Flap reconstruction (local or free) for exposed bone/hardware where direct closure is not possible
Phase 6 - Rehabilitation
- Early range of motion exercises (30-120 degrees active) once stability achieved - critical to prevent stiffness
- Physiotherapy initiated within first 3 weeks
- Splinting in functional position between exercises
- Stiffness is the most common long-term outcome even in successfully managed cases (Pye's)
- Heterotopic ossification prophylaxis (indomethacin or single-dose radiation) considered for high-energy injuries
Complications
| Complication | Comment |
|---|---|
| Elbow stiffness and contracture | Most common; often permanent |
| Nonunion | Especially with bone loss; may require bone grafting |
| Infection / osteomyelitis | Risk increases with open/contaminated wounds (11% deep infection in some series) |
| Nerve palsy (permanent) | Radial nerve most common; brachial plexus injury rare but devastating |
| Vascular compromise / limb loss | Amputation required if vascular repair fails or delayed |
| Compartment syndrome | Forearm; urgent fasciotomy required |
| Heterotopic ossification | Leads to additional stiffness |
| Hardware failure | Especially in comminuted fractures with osteopenic bone |
| Post-traumatic arthritis | Especially with articular surface comminution |
Key Points Summary
- Sideswipe injury = violent lateral blow to the elbow protruding from a vehicle window - a high-energy, complex, open injury
- The classic triad is: open fracture + soft tissue loss + neurovascular injury
- Most common fracture pattern: distal humerus + proximal ulna (Monteggia type) + radial head fractures
- Brachial artery injury in 10-20% of severe cases; a warm pink pulseless hand does not exclude arterial injury
- Radial nerve palsy is the most common nerve injury and the main determinant of poor outcome
- Management is staged: debridement first, then fixation, then soft tissue reconstruction
- Prognosis is guarded; stiffness, contracture, and nerve deficits are common
- 22nd Edition Pye's Surgical Handicraft, p. 187 - Fracture-dislocation of the elbow / sideswipe injury
- Rosen's Emergency Medicine, 9th ed. - Elbow trauma, neurovascular assessment
- Campbell's Operative Orthopaedics, 15th ed. 2026 - Vascular injury in elbow fractures
- Rockwood and Green's Fractures in Adults, 10th ed. 2025 - Open distal humerus fractures
- Pandey R et al. "An unusual mechanism of sideswipe injury in passengers traveling in a train and review of literature." Int J Burns Trauma 2021 [PMID: 34858714]
- Oyewole OA et al. "Sideswipe Injury of the Knee." Niger Med J 2020 [PMID: 33487856]