What is clubbing in medical terms
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough explanation of digital clubbing in medical terms, sourced from authoritative textbooks:
Finger/Digital Clubbing
Clubbing (also called "digital clubbing" or "Hippocratic fingers") is the selective bulbous enlargement of the distal segments of the digits due to an increase in soft tissue beneath the nail bed. It affects both fingers and toes.
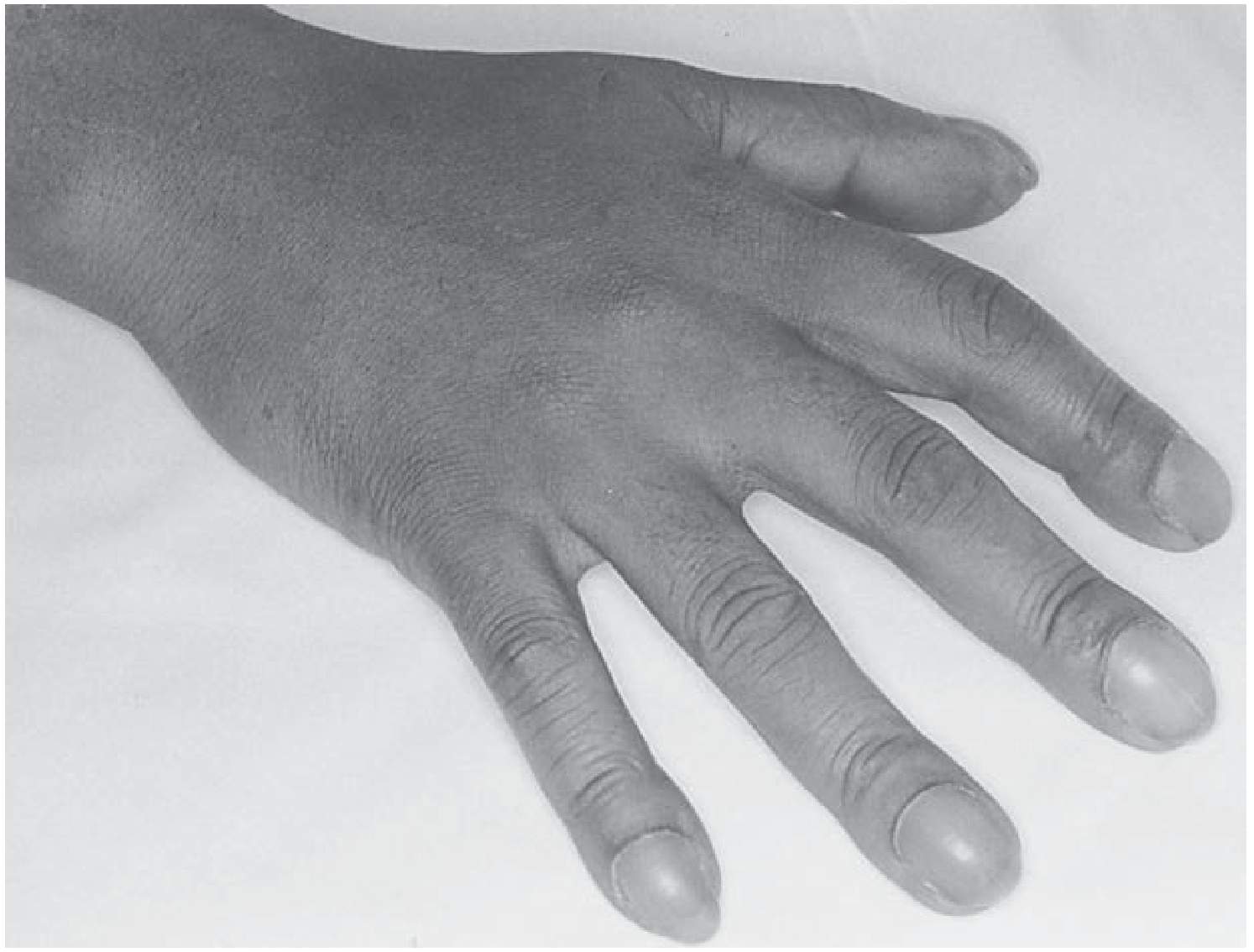
Clubbing of all fingers. - Fishman's Pulmonary Diseases and Disorders

Clubbed fingers showing rounded, bulbous tips - Andrews' Diseases of the Skin
Clinical Features (How to Recognize It)
When fully established, clubbing shows four hallmarks:
- Loss of nail-cuticle angle - The normal 160-165° angle between the nail and the cuticle (Lovibond angle) becomes obliterated and increases to 180° or greater. This is the most sensitive sign.
- Softening and sponginess of the nail base - The nail appears to "float" on a soft, spongy bed; perilingual erythema is often present.
- Enlargement of the distal phalanx - The fingertip becomes bulbous, warm, and possibly erythematous.
- Curved nails - The nails curve in both the longitudinal and coronal (transverse) planes.
Schamroth sign: When the dorsal surfaces of opposing fingers from each hand are placed together, the normal small diamond-shaped window at the nail base disappears in clubbing.
Pathophysiology (Why It Happens)
The main mechanism involves:
- Increased capillary density stimulated by chronic hypoxia, which drives vascular growth factor production.
- Elevated levels of VEGF (vascular endothelial growth factor), PDGF (platelet-derived growth factor), HIF-1α, and HIF-2α have been demonstrated histochemically in clubbed digits.
- Shunting of blood past the capillary bed of the lung or liver - this means angiogenic factors are not metabolized in a critical organ, and they accumulate to stimulate tissue proliferation.
Clubbing can develop rapidly (as quickly as 2 weeks in new-onset empyema) and can also reverse within 2 weeks (e.g., after corrective cardiac surgery).
- Murray & Nadel's Textbook of Respiratory Medicine, p. 3782-3788
Causes
Clubbing is divided into idiopathic/hereditary and acquired/secondary forms:
Not associated with overt disease:
- Hereditary (familial) clubbing - caused by mutations in the HPGD gene (encoding 15-hydroxyprostaglandin dehydrogenase) or the SLCO2A1 prostaglandin transporter gene
- Sporadic clubbing
- Pachydermoperiostosis (primary hypertrophic osteoarthropathy)
Thoracic / Pulmonary (most common group):
- Lung cancer - the single most common cause of acquired clubbing
- Bronchiectasis, lung abscess, empyema
- Cystic fibrosis
- Benign and malignant pleural tumors
- Esophageal cancer, lymphoma
Cardiac and vascular:
- Cyanotic congenital heart disease
- Subacute bacterial endocarditis
- Infected aortic graft
- Takayasu's arteritis, Behçet syndrome
Liver and GI disease:
- Liver cirrhosis / hepatopulmonary syndrome
- Inflammatory bowel disease (Crohn's, ulcerative colitis)
- Cirrhosis with arteriovenous shunting
Infections / other:
- HIV infection (~36% of HIV-positive patients have clubbed nails)
- Benign asbestos pleural disease
Unilateral or asymmetric clubbing can occur in Takayasu arteritis, sarcoidosis, or local causes (injury to a finger or the median nerve).
- Andrews' Diseases of the Skin, p. 898
- Murray & Nadel's Textbook of Respiratory Medicine (eTable 18.1)
Associated Condition: Hypertrophic Osteoarthropathy (HOA)
Clubbing can progress to or be associated with hypertrophic osteoarthropathy (HOA), which involves:
- Subperiosteal new bone formation at the distal ends of long bones (especially the radius, ulna, tibia, and fibula)
- Painful swelling of joints (e.g., knees, wrists)
- HOA is most common in patients with bronchogenic carcinoma and cystic fibrosis
- It can also be idiopathic, familial, or drug-induced (e.g., voriconazole)
Clinical Significance
Clubbing was found in about 1% of all admissions to an internal medicine ward, and was associated with "serious disease" in 40% of affected patients. New-onset clubbing therefore always warrants:
-
A chest X-ray as the first step
-
A CT scan if the X-ray is unrevealing, to rule out pulmonary neoplasm or other occult lesion
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 3784
-
Fishman's Pulmonary Diseases and Disorders, p. 447
Summary Table
| Feature | Detail |
|---|---|
| Definition | Bulbous enlargement of distal digits due to soft tissue increase |
| Key sign | Lovibond angle ≥ 180°; loss of Schamroth window |
| Most common cause | Lung cancer (acquired); hereditary HPGD mutation (familial) |
| Mechanism | Hypoxia → VEGF/PDGF → increased capillary density + angiogenic shunting |
| Associated syndrome | Hypertrophic osteoarthropathy (HOA) |
| Reversibility | Can reverse in ~2 weeks after correction of underlying cause |
This is a shared conversation. Sign in to Orris to start your own chat.