How to do continuous bladder irrigation
Reading File
Finding Sources
Finding Sources
Searching the Web
continuous bladder irrigation procedure nursing technique 2024
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer.
Continuous Bladder Irrigation (CBI)
Continuous bladder irrigation is a procedure that flushes the bladder with sterile saline via a three-way Foley catheter to prevent or dissolve blood clots - most commonly after transurethral resection of the prostate (TURP) or other bladder/prostatic surgery.
Indications
- Post-TURP or post-prostatectomy hematuria with clot risk
- Gross hematuria with clot retention
- Hemorrhagic cystitis (radiation-induced, cyclophosphamide-related)
- Post-bladder tumor resection
Equipment Needed
- Three-way (triple-lumen) Foley catheter - 22F to 26F (larger bore accommodates clot passage)
- Port 1: irrigation inflow
- Port 2: drainage outflow
- Port 3: balloon inflation
- Sterile normal saline in 2-L or 4-L bags
- IV administration/irrigation tubing set
- Large-volume drainage collection bag
- IV pole
Step-by-Step Procedure
The 10-step photo guide below comes from Roberts and Hedges' Clinical Procedures in Emergency Medicine:
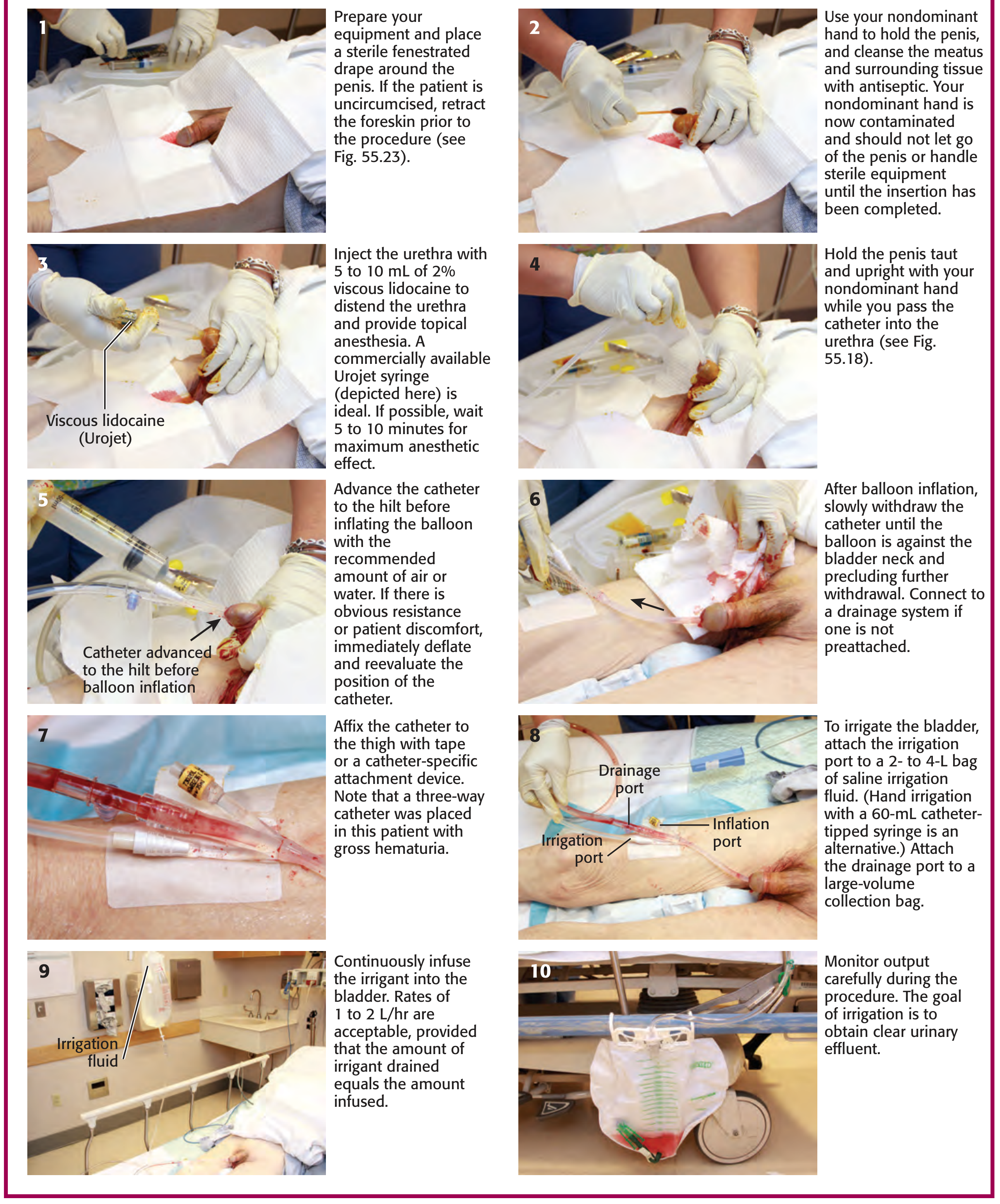
Steps 1-7: Catheter insertion (if not already in place)
- Prepare equipment; place a sterile fenestrated drape. Retract foreskin if uncircumcised.
- Hold the penis with the non-dominant hand; cleanse the meatus and surrounding tissue with antiseptic (hand is now contaminated - do not release grip).
- Inject 5-10 mL of 2% viscous lidocaine into the urethra for topical anesthesia and urethral distention. Wait 5-10 minutes for maximum effect.
- Hold the penis taut and upright; pass the catheter gently into the urethra.
- Advance the catheter fully to the hilt before inflating the balloon. If resistance or patient discomfort occurs, deflate immediately and reposition.
- After balloon inflation, slowly withdraw the catheter until the balloon seats against the bladder neck. Connect to the drainage system.
- Affix the catheter to the thigh with tape or a catheter-specific attachment device.
Steps 8-10: Setting up irrigation
- Attach the irrigation port to a 2-4 L bag of sterile saline irrigation fluid hung on an IV pole. Attach the drainage port to a large-volume collection bag at the bedside.
- Begin continuous infusion by gravity. Rates of 1 to 2 L/hr are acceptable, provided the volume drained equals the volume infused.
- Monitor output closely - adjust the flow rate based on urine color. The goal is clear urinary effluent.
Flow Rate Titration
| Urine color | Action |
|---|---|
| Bright red / frank blood | Increase flow rate; consider manual syringe flush to break up clots |
| Dark pink/rose | Maintain current rate |
| Light pink/straw | Can cautiously decrease rate |
| Clear | Consider stopping CBI if sustained |
The rate can be brisk - 1 to 2 L/hr or more - as long as output volume equals input volume. Use 60-mL aliquots with a catheter-tipped syringe for manual irrigation if gravity is insufficient to clear a clot.
Calculating Urine Output During CBI
Because saline is continuously entering the drainage bag, you cannot read urine output directly. Use this formula:
True urine output = Total drainage bag volume - Total irrigation saline infused
Track saline infused carefully on a running worksheet. Document at regular intervals (every 1-4 hours depending on clinical need).
Monitoring and Nursing Care
- Check urine color every 15-30 minutes initially; adjust flow accordingly
- Ensure the catheter and tubing are free of kinks at all times
- If drainage stops suddenly, suspect clot obstruction - perform a manual bladder irrigation with a 60-mL catheter-tipped syringe
- Ensure output volume equals input volume; if less is draining than going in, the catheter may be blocked
- Monitor for bladder distension - patient reports suprapubic pressure, urge to void around the catheter, or leakage around the catheter
Complications to Watch For
| Complication | Signs | Action |
|---|---|---|
| Catheter obstruction by clot | Reduced/absent drainage, suprapubic pain | Manual flush with 60-mL syringe |
| Bladder distension | Suprapubic fullness, leakage around catheter | Check tubing for kinks; manual flush |
| Fluid overload (over-irrigation) | Edema, electrolyte imbalance | Ensure in = out; slow rate |
| Infection (CAUTI) | Fever, foul-smelling urine | Routine antibiotic prophylaxis is NOT recommended; treat if symptomatic |
| Bladder spasm | Cramping, urge around catheter | Antispasmodics (e.g., oxybutynin) may help |
Routine antimicrobial prophylaxis should not be used during catheterization to avoid promoting antimicrobial resistance. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
When to Stop CBI
- Urine remains consistently clear for several hours
- Physician orders discontinuation based on clinical assessment
- Typically 12-24 hours post-operatively after TURP, though this varies by case
Key Points Summary
-
Always use a three-way (22-26F) Foley - a standard two-way catheter cannot handle simultaneous inflow and outflow
-
Gravity drive at 1-2 L/hr is sufficient; titrate to urine color
-
Always verify drainage = infusion to avoid bladder over-distension
-
Calculate true urine output by subtracting total irrigant infused from total drainage
-
A manual syringe flush with 60 mL saline is the first response to catheter obstruction
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine, Fig. 55.21 and Bladder Irrigation section
-
Bailey and Love's Short Practice of Surgery 28th Ed., Urology chapter (post-TURP CBI context)
This is a shared conversation. Sign in to Orris to start your own chat.