Twisty questions and answers for viva of panophthalmitis
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed. Here is a comprehensive set of twisty viva questions and answers on panophthalmitis:
Twisty Viva Q&A: Panophthalmitis
Definitions & Distinctions
Q1. You see a patient with severe intraocular inflammation. The examiner asks: "Is this endophthalmitis or panophthalmitis?" What is the key distinguishing anatomical criterion?
Endophthalmitis = inflammation of the interior of the eye confined to the vitreous humor and internal ocular structures. Panophthalmitis = the same process that has extended outward into the uvea (choroid + ciliary body + iris), sclera, and ultimately the orbit. The boundary-crossing from intraocular to trans-scleral/orbital is the critical distinction.
- Robbins, Cotran & Kumar, p. 1216
Q2. A surgeon says "I'll treat this panophthalmitis the same way I treat endophthalmitis." What trap has he fallen into?
Panophthalmitis with orbital involvement is a different beast. Because inflammation has breached the sclera into the orbit, you get proptosis, restricted ocular motility, chemosis, eyelid oedema on top of the intraocular signs. It can masquerade as or co-exist with orbital cellulitis. Treating it only as endophthalmitis (intravitreal antibiotics alone) without addressing systemic sepsis and orbital spread is dangerously inadequate.
- Wills Eye Manual (signs section)
Q3. "Endophthalmitis and panophthalmitis are both intraocular infections." Agree or disagree?
Disagree - at the point of panophthalmitis, the infection is no longer purely intraocular. It has extended into the uvea, sclera and orbit. The term "intraocular" correctly applies to endophthalmitis, not panophthalmitis.
Classification Traps
Q4. A patient develops panophthalmitis after a neighbour's Diwali firecracker hits their eye. Another patient develops it after lung sepsis. How do you classify these two cases - and why does the classification matter for management?
- Exogenous panophthalmitis: Pathogen enters from the environment through a wound (penetrating trauma, post-surgical). The firecracker case fits here.
- Endogenous panophthalmitis: Pathogen is delivered hematogenously from a distant focus (e.g., pulmonary infection, IV drug use, systemic candidemia). The lung sepsis case fits here.
Classification matters because:
-
Exogenous: needs wound management, intravitreal antibiotics, possibly vitrectomy
-
Endogenous: systemic antibiotics to eliminate the source are key - without them you are treating the eye but leaving the bacteraemia/fungaemia untreated. You must also search for the septic focus (echocardiogram, blood cultures, etc.)
-
Robbins, Cotran & Kumar, p. 1216; Kanski's
Q5. The examiner shows you a slide of a patient with endogenous endophthalmitis and asks: "What populations should make you immediately think of this diagnosis?"
- IV drug users (Candida, S. aureus bacteraemia)
- Immunocompromised patients / AIDS (Candida, CMV retinitis can progress)
- Patients with known systemic candidemia from any source
- Patients with pulmonary infections or infective endocarditis
The classic trick: CMV retinitis in AIDS is an important cause of infectious retinitis/visual morbidity - don't confuse the retinitis picture with bacterial endophthalmitis in an immunocompromised patient.
- Robbins, Cotran & Kumar, p. 1216
Organisms & Microbiology Traps
Q6. "In a garden injury with a piece of metal entering the eye, the most likely pathogen is Staphylococcus." Do you agree?
No - the most notorious organism in soil-associated / vegetable garden penetrating eye injuries is Bacillus cereus. This is a gram-positive, spore-forming rod that is:
- Notoriously aggressive and rapid
- Carries genes for resistance to penicillins and cephalosporins (so don't use amoxicillin or cefazolin)
- Treated with vancomycin, clindamycin, ciprofloxacin, or gentamicin
The clinical course is fulminant - despite prompt surgical and intravitreal antibiotic therapy (vancomycin + ceftazidime + dexamethasone + ciprofloxacin), evisceration may still be required. This is the classic teaching case in every microbiology textbook.
- Medical Microbiology 9e, Clinical Case 20.2
Q7. Pseudomonas aeruginosa causes panophthalmitis - what is the context, and why is it called "devastating"?
P. aeruginosa endophthalmitis occurs secondary to bacteraemia (rarely, as a complication of cataract surgery). It is described as "the most devastating of P. aeruginosa eye infections" because it presents with:
- Severe pain
- Chemosis
- Decreased visual acuity
- Anterior uveitis
- Vitreous involvement progressing rapidly to panophthalmitis
The fulminant course means vision loss is common even with treatment.
- Harrison's Principles of Internal Medicine 22E
Q8. Why are penicillins and cephalosporins NOT appropriate monotherapy for traumatic panophthalmitis from soil/garden injuries?
Because the key culprit - Bacillus cereus - harbours genes encoding resistance to both beta-lactam classes. Using amoxicillin or a cephalosporin would leave the dominant organism untreated while the eye is rapidly destroyed (B. cereus produces cytotoxins including haemolysins and proteases). Empirical therapy must cover gram-positive organisms with vancomycin plus gram-negative coverage with ceftazidime (intravitreally).
Clinical Signs Traps
Q9. A registrar says "The red reflex is intact, so this can't be endophthalmitis progressing to panophthalmitis." Is this reasoning safe?
No. Loss of the red reflex is a sign of significant vitreous involvement/opacity, but early endophthalmitis may still have a partially present red reflex. The sequence is: corneal haze → hypopyon → vitritis → loss of red reflex → orbital signs. Absence of red reflex loss does not exclude the diagnosis. If there is any clinical doubt, treat empirically as endophthalmitis - early treatment is the only thing that saves vision.
- Kanski's Clinical Ophthalmology 10th
Q10. What distinguishes the signs of panophthalmitis from orbital cellulitis on examination?
Both share: proptosis, periorbital oedema, restricted ocular motility, chemosis. The distinguishing features of panophthalmitis are the intraocular signs: hypopyon, vitritis, absent red reflex, and evidence of an intraocular source (penetrating wound, recent surgery, or known sepsis). Orbital cellulitis is primarily a periorbital/sinogenic process without these intraocular findings.
The complication chart is also important: panophthalmitis is itself a complication of orbital cellulitis (from ethmoiditis, dacryocystitis, infected hordeolum, dental abscess - especially via direct extension). So panophthalmitis can be an endpoint of either intraocular or extra-orbital disease.
- Wills Eye Manual; Tintinalli's Emergency Medicine
Q11. In endophthalmitis/panophthalmitis secondary to orbital cellulitis, what is the most feared systemic complication and what pathogens should you suspect?
Cavernous sinus thrombosis is the most feared intracranial complication. Responsible pathogens in orbital cellulitis (which can progress to panophthalmitis) include: S. pneumoniae, M. catarrhalis, S. aureus, S. pyogenes, and anaerobic upper respiratory flora (Bacteroides, Fusobacterium).
- Tintinalli's Emergency Medicine
Treatment Traps
Q12. The EVS (Endophthalmitis Vitrectomy Study) concluded that systemic antibiotics do not improve outcomes in postoperative endophthalmitis. Can you apply this to panophthalmitis?
No - and this is a classic viva trap. The EVS findings are specific to post-cataract surgery endophthalmitis. In panophthalmitis, particularly endogenous disease and traumatic disease, systemic antibiotics are important because:
- In endogenous disease: they are key to eliminating the haematogenous source
- In traumatic/exogenous disease: systemic antibiotics reduce the risk of progression and treat any systemic seeding
The EVS conclusions cannot be extrapolated beyond their study population.
- Kanski's Clinical Ophthalmology 10th
Q13. You are about to give intravitreal vancomycin as prophylaxis at the end of cataract surgery in a patient who doesn't have established endophthalmitis. Is this safe?
No. Intravitreal vancomycin used as routine prophylaxis has been reported to cause haemorrhagic occlusive retinal vasculitis in some patients and should be avoided as prophylactic use. The recommended intracameral prophylaxis is cefuroxime 1 mg in 0.1 ml injected into the anterior chamber at the end of surgery (alternative: moxifloxacin 0.5 mg in 0.1 ml if cefuroxime unavailable).
- Kanski's Clinical Ophthalmology 10th
Q14. Intravitreal ceftazidime dose is 2 mg in 0.1 ml. Intravitreal amikacin dose is also 0.1 ml - but what hidden danger must you know about amikacin vs ceftazidime?
The dose of intravitreal amikacin is 0.4 mg (much lower than 2 mg ceftazidime) - note the different dilution procedure. More critically, amikacin carries a higher risk of retinal infarction compared to ceftazidime. Therefore, amikacin should only be used when there is a well-defined penicillin or cephalosporin allergy preventing use of ceftazidime. It is not a routine first choice.
- Kanski's Clinical Ophthalmology 10th
Q15. "Systemic antibiotics are not effective in endophthalmitis, so I won't prescribe them." This statement appears in a textbook. Under what specific circumstance is this correct, and when is it dangerously wrong?
Correct: in post-cataract surgery endophthalmitis, systemic antibiotics add no benefit (per EVS data). The mainstay is intravitreal antibiotics ± pars plana vitrectomy.
Dangerously wrong in:
- Endogenous endophthalmitis/panophthalmitis - systemic antibiotics are key to eliminating the haematogenous focus (bacteraemia, fungaemia, infective endocarditis). Without them, the eye is re-seeded.
- Traumatic panophthalmitis - systemic antibiotics reduce risk and treat systemic extension.
- Orbital cellulitis complicated by panophthalmitis - IV antibiotics are the primary treatment.
- Kanski's Clinical Ophthalmology; Rosen's Emergency Medicine
Q16. When should you perform vitrectomy in endophthalmitis, and what was the EVS finding about visual acuity thresholds?
Per EVS, pars plana vitrectomy (PPV) improved outcomes in patients with light perception only vision - in this group, vitrectomy led to significantly better visual acuity outcomes. Patients with hand motion or better vision did not show significant benefit from immediate vitrectomy (tap and inject was adequate).
In endophthalmitis / panophthalmitis not covered by the EVS (traumatic, endogenous), PPV may improve prognosis and should be considered on its merits. If vitrectomy is not immediately available, intravitreal antibiotics should be given as a temporizing measure rather than waiting.
- Kanski's Clinical Ophthalmology 10th
Q17. A patient with panophthalmitis requires vitreous sampling. The surgeon says "aqueous tap and vitreous tap are equally good for culture." Agree?
Disagree. Vitreous sampling is more likely to yield a positive culture than aqueous. The ideal method is a disposable vitrector (manual vitreous tap with 23-gauge needle also acceptable). Aqueous sampling yields 0.1-0.2 ml via limbal paracentesis and has lower sensitivity. A negative culture from aqueous does not rule out infection - treatment should always be continued regardless of culture result.
- Kanski's Clinical Ophthalmology 10th
Steroids - The Double-Edged Sword
Q18. An examiner asks: "Should you give steroids in panophthalmitis?" This is a trick - walk them through your reasoning.
The rationale for steroids is to limit the inflammatory destruction that, even when the organism is killed, continues to damage the retina. However:
- Never give steroids before excluding fungal infection (steroids worsen fungal disease catastrophically)
- Oral prednisolone (1 mg/kg/day) may be considered in severe bacterial cases after 12-24 hours of antibiotics, once fungal aetiology is excluded from smear examination
- Periocular steroids (dexamethasone or triamcinolone) are an alternative when systemic therapy is contraindicated
- The place of systemic steroids remains undefined - no strong RCT evidence
The trap is either reflexively giving steroids (dangerous if fungal) or reflexively withholding them (losing the anti-inflammatory benefit in severe bacterial disease).
- Kanski's Clinical Ophthalmology 10th
Surgical Endpoints
Q19. What is the difference between evisceration and enucleation, and which is preferred in panophthalmitis?
- Evisceration: Removal of the intraocular contents while leaving the scleral shell (and extraocular muscles) intact. Gives a better cosmetic result and faster rehabilitation with a prosthesis.
- Enucleation: Removal of the entire eyeball including sclera (with ligation of the optic nerve).
In panophthalmitis: evisceration is generally preferred (better cosmesis, preserves the orbital socket). However, if there is concern for sympathetic ophthalmia or orbital/intracranial spread, enucleation is safer. The B. cereus case above illustrates that even aggressive treatment may culminate in evisceration.
- Kanski's Clinical Ophthalmology 10th; Tietz Textbook
Q20. "If the eye is lost to panophthalmitis, the job is done." What serious risk does the fellow eye now face?
Sympathetic ophthalmia - a bilateral granulomatous uveitis where the healthy (sympathizing) eye mounts a T-cell mediated autoimmune attack against uveal antigens released by the injured (exciting) eye. It can occur weeks to decades after the inciting injury. This is why timely enucleation of a blind, painful eye (within 2 weeks of injury, before sympathetic ophthalmia develops) may be recommended - though evisceration is usually preferred cosmetically once the risk window has passed.
Pathology Viva Hook
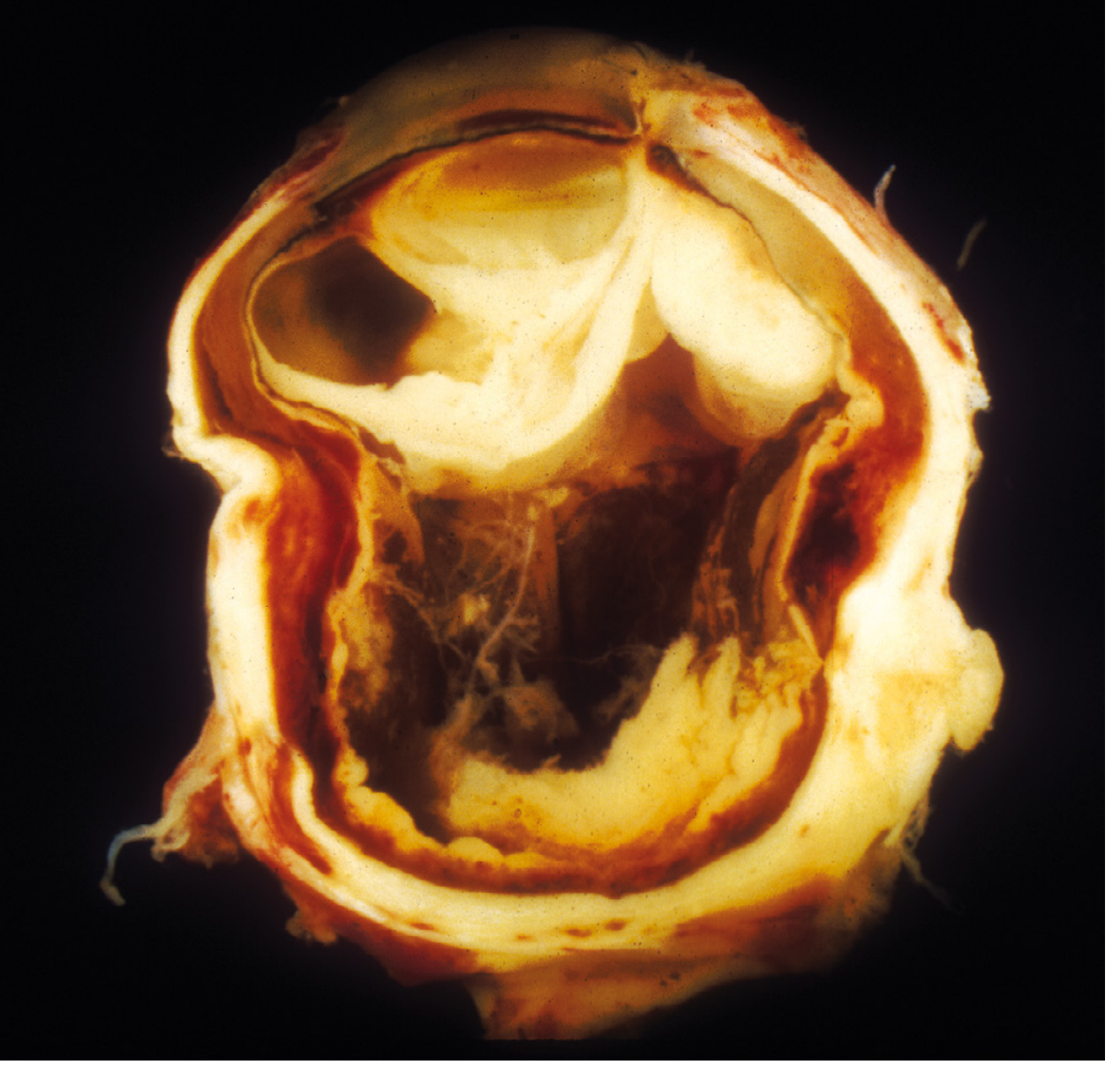
Q21. The examiner shows you the gross specimen photograph (above). Describe what you see and what caused it.
The cross-section shows a globe with completely distorted architecture - the normal layered structure (sclera, choroid, retina) is lost, replaced by diffuse suppurative inflammation throughout. The internal cavity shows purulent/exudative material and the scleral coat is thickened and inflamed, with suppuration extending outward. This is exogenous panophthalmitis following penetrating foreign body injury - suppurative inflammation of the entire orbit has effaced normal ocular anatomy. The specimen was removed (enucleation) because the eye was unsalvageable.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 29.16
Quick Reference Summary Table
| Feature | Endophthalmitis | Panophthalmitis |
|---|---|---|
| Extent | Vitreous + intraocular | Uvea + sclera + orbit |
| Proptosis/restricted motility | No | Yes |
| Red reflex | Lost (late) | Lost |
| Hypopyon | Yes | Yes |
| Systemic antibiotics | Not in post-op (EVS) | Yes (especially endogenous) |
| Surgery | Vitrectomy + intravitreal | Vitrectomy ± evisceration/enucleation |
| Sympathetic ophthalmia risk | Lower | Higher (open globe) |
Top organisms to know by context:
| Context | Key Organism | Trap |
|---|---|---|
| Post-cataract surgery | CoNS (S. epidermidis) | Most common; usually indolent |
| Penetrating garden/soil injury | Bacillus cereus | Penicillin/cephalosporin-RESISTANT |
| IV drug use / candidaemia | Candida spp. | Endogenous; treat systemically |
| Orbital cellulitis | S. pneumoniae, S. aureus, anaerobes | Risk of cavernous sinus thrombosis |
| P. aeruginosa bacteraemia | Pseudomonas aeruginosa | "Most devastating" eye infection |
This is a shared conversation. Sign in to Orris to start your own chat.