hypertension for pathology 2 nd year BDS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive, textbook-sourced content with images. Here is the complete, well-organized answer for 2nd year BDS pathology:
Hypertension - Pathology (2nd Year BDS)
Based on Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
1. Definition and Classification
Hypertension is defined as sustained diastolic pressure >80 mm Hg or sustained systolic pressure >120 mm Hg. It affects approximately 40-50% of the general population and is a major risk factor for atherosclerosis, congestive heart failure, stroke, and renal failure.
Types:
| Type | Frequency | Key Feature |
|---|---|---|
| Primary (Essential/Idiopathic) | 90-95% of cases | No identifiable cause; multifactorial |
| Secondary | 5-10% of cases | Identifiable underlying disease |
Synonyms for primary hypertension: Essential, idiopathic, benign hypertension (though "benign" is a misnomer - it is neither benign nor essential).
2. Blood Pressure Regulation (Physiology Review)
Understanding the regulation is key to understanding why hypertension occurs:
- Blood pressure = Cardiac output × Peripheral vascular resistance
- Cardiac output is determined by heart rate and stroke volume (influenced by blood volume)
- Blood volume is regulated mainly by renal sodium excretion/reabsorption
- The Renin-Angiotensin-Aldosterone System (RAAS) is the central regulator
RAAS pathway:
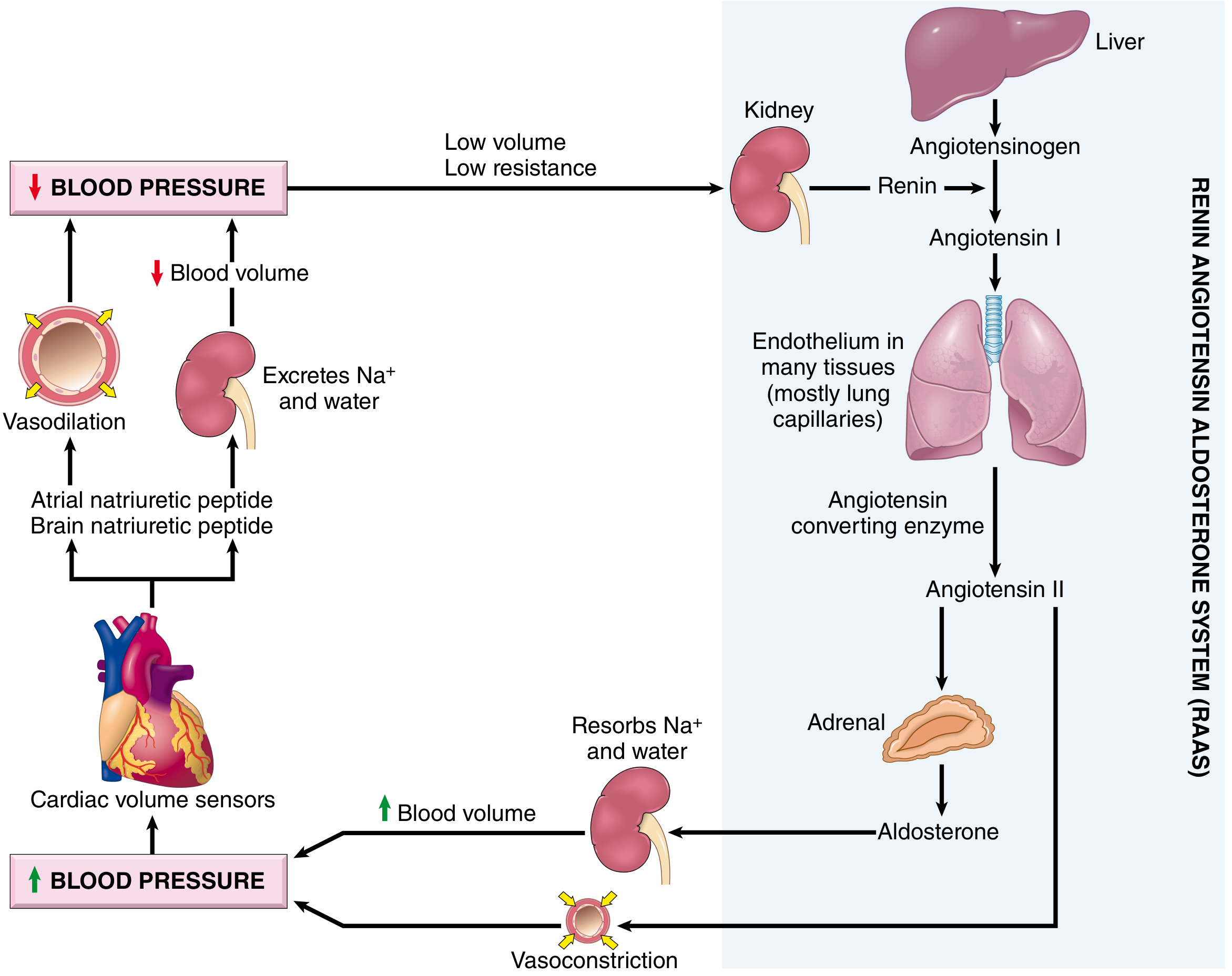
Low BP → Kidney secretes Renin → Renin cleaves Angiotensinogen (liver) → Angiotensin I → ACE in lung endothelium → Angiotensin II → (a) Vasoconstriction + (b) Aldosterone release from adrenal → Na⁺ and water reabsorption → increased blood volume → increased BP
Counterbalancing this are natriuretic peptides (ANP from atria, BNP from brain/ventricles) which promote vasodilation and Na⁺ excretion.
3. Causes of Secondary Hypertension
| System | Causes |
|---|---|
| Renal | Acute/chronic glomerulonephritis, polycystic kidney disease, renal artery stenosis (renovascular HTN), renin-secreting tumors |
| Endocrine | Cushing syndrome, primary aldosteronism, pheochromocytoma, acromegaly, hypothyroidism, hyperthyroidism, oral contraceptives |
| Cardiovascular | Coarctation of the aorta, polyarteritis nodosa |
| Neurologic | Increased intracranial pressure, obstructive sleep apnea |
Renovascular hypertension mechanism: Renal artery stenosis → decreased glomerular flow → RAAS activation → increased vasoconstriction + blood volume.
Primary hyperaldosteronism (idiopathic or adrenal adenoma) is one of the most frequent causes of secondary hypertension.
Rare single-gene disorders:
- Defects in aldosterone metabolism enzymes (aldosterone synthase, 11β-hydroxylase, 17α-hydroxylase) → excess aldosterone → salt/water retention
- Liddle syndrome - mutation in epithelial Na⁺ channel (ENaC-γ) → exaggerated distal tubular Na⁺ reabsorption
4. Pathogenesis of Primary (Essential) Hypertension
Primary hypertension is a complex, multifactorial disorder involving both genetic and environmental factors. The final common pathway is:
Increased blood volume + Increased peripheral vascular resistance (both often linked to increased Na⁺ reabsorption by the kidney)
Genetic Factors:
- Twin studies and genome-wide association studies (GWAS) confirm strong genetic contribution
- 500+ genetic variants are identified, each with small individual effects
- Polymorphisms affecting sodium resorption, the RAAS, aldosterone pathways, and the adrenergic nervous system all play roles
Environmental Factors:
- Dietary sodium - excess Na⁺ increases blood volume
- Obesity - promotes insulin resistance, activates the sympathetic nervous system, and stimulates Na⁺ reabsorption
- Stress - adrenergic system activation increases cardiac output and vascular resistance
Key pathophysiologic mechanisms:
- Reduced renal Na⁺ excretion at any given blood pressure level ("resetting of the pressure-natriuresis curve") - central mechanism
- RAAS dysregulation - inappropriately elevated renin/angiotensin II activity
- Increased sympathetic nervous system activity
- Defects in natriuretic peptide signaling
- Endothelial dysfunction - reduced nitric oxide (vasodilator) production
5. Vascular Pathology in Hypertension
Hypertension causes two main types of vascular injury. Both are visible histologically and are exam-important.
A. Hyaline Arteriolosclerosis (Benign HTN)
- Seen in primary hypertension (also in diabetes and normal aging, but more generalized/severe in HTN)
- Arteriolar walls show homogeneous, pink (eosinophilic), hyaline thickening with luminal narrowing
- Caused by:
- Plasma protein leakage across injured endothelial cells
- Increased ECM production by smooth muscle cells (SMCs) in response to chronic hemodynamic stress
- In the kidney → nephrosclerosis (diffuse vascular compromise + glomerular scarring)
B. Hyperplastic Arteriolosclerosis (Malignant/Severe HTN)
- Seen in severe/malignant hypertension
- Vessels show concentric, laminated "onion-skin" thickening with luminal narrowing
- Laminations consist of SMCs + thickened, reduplicated basement membrane
- In malignant hypertension: accompanied by fibrinoid deposits and vessel wall necrosis (necrotizing arteriolitis), especially prominent in the kidney
Histology (Robbins Fig. 8.4):
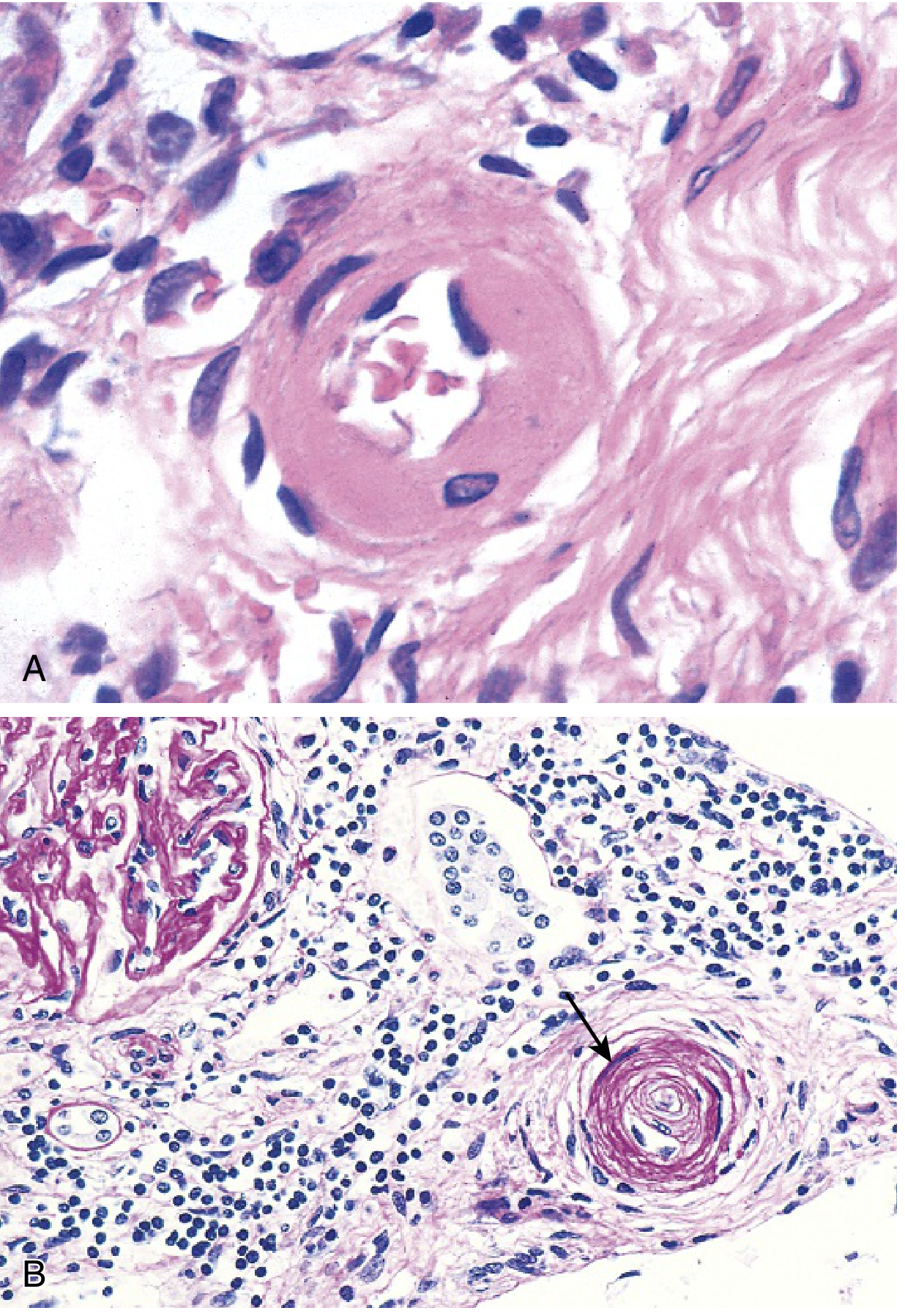
Fig. A: Hyaline arteriolosclerosis - arteriolar wall thickened with amorphous proteinaceous material, markedly narrowed lumen. Fig. B: Hyperplastic arteriolosclerosis ("onion-skinning", arrow) causing luminal obliteration (PAS stain)
6. Consequences / End-Organ Damage
A. Heart - Hypertensive Heart Disease
Left-sided (Systemic) Hypertensive Heart Disease:
Diagnostic criteria:
- Left ventricular hypertrophy (LVH) in the absence of other cardiovascular pathology
- History or evidence of hypertension in other organs
Gross morphology:
- Heart weight >500 g (normal 320-360 g in a 60-70 kg individual)
- LV wall thickness >2.0 cm (normal 1.2-1.4 cm)
- Concentric hypertrophy (pressure overload, NO early dilation)
- Late stage: LV dilation when heart fails
Microscopy:
- Increased transverse diameter of myocytes
- "Boxcar nuclei" (prominent nuclear enlargement and hyperchromasia)
- Intercellular fibrosis
Clinical features:
- Usually asymptomatic initially (detected by BP measurement, ECG/echo)
- Later: atrial fibrillation (from left atrial dilation), congestive heart failure (CHF)
- Increased risk of ventricular arrhythmias, sudden cardiac death, MI, and stroke
- HTN control can cause regression of hypertrophy
Right-sided (Cor Pulmonale): Right ventricular hypertrophy/dilation from pulmonary hypertension (due to lung disorders, not directly systemic HTN)
B. Kidney - Nephrosclerosis
- Hyaline arteriolosclerosis in renal arterioles → reduced blood flow → ischemic glomerular damage and tubular atrophy
- Gross: bilaterally contracted, granular kidneys
- Result: chronic renal failure
C. Brain
- Stroke (cerebral hemorrhage or infarction)
- Hypertension is the single most important risk factor for hemorrhagic stroke
- Can also cause lacunar infarcts and multi-infarct dementia
D. Blood Vessels (Large arteries)
- Accelerates atherosclerosis
- Promotes aortic dissection and aortic aneurysm
- Cerebrovascular hemorrhage
7. Malignant Hypertension
- Rapidly progressive, severe form
- BP typically >180/120 mm Hg
- Characterized by:
- Hyperplastic arteriolosclerosis with fibrinoid necrosis
- Necrotizing arteriolitis (especially kidney)
- Papilledema
- Acute renal failure
- Encephalopathy
- Medical emergency
8. Summary - Key Concepts Table
| Feature | Detail |
|---|---|
| Definition | Sustained BP >120/80 mm Hg |
| Most common type | Primary/Essential (90-95%) |
| Pathogenesis | Increased Na⁺ reabsorption → RAAS activation → ↑BP |
| Benign HTN vascular lesion | Hyaline arteriolosclerosis ("pink, glassy" wall thickening) |
| Malignant HTN vascular lesion | Hyperplastic arteriolosclerosis ("onion-skin") + fibrinoid necrosis |
| Cardiac effect | LV concentric hypertrophy → "Boxcar nuclei" on microscopy |
| Renal effect | Nephrosclerosis (arteriolar narrowing + glomerular scarring) |
| Major risk for | Atherosclerosis, stroke, heart failure, renal failure |
Oral Pathology Relevance (BDS Specific)
Hypertension is relevant to dental practice:
- Many antihypertensive drugs (Ca-channel blockers like nifedipine, amlodipine) cause gingival enlargement (drug-induced gingival overgrowth)
- Patients on antihypertensives need BP monitoring before dental procedures
- Hypertension promotes periodontal disease (shared risk factors - inflammation, endothelial dysfunction)
- Stress of dental procedures can acutely elevate blood pressure
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 311-315, 362-363 | Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 445-448, 463
This is a shared conversation. Sign in to Orris to start your own chat.