Management of hypotension
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypotension" AND "management"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent — I now have all the key content and images needed for a comprehensive answer.
Management of Hypotension
Hypotension (SBP < 90 mmHg or MAP < 65 mmHg, or a ≥40 mmHg drop from baseline) can reflect shock — a state of inadequate oxygen delivery to tissues. Management is guided by the underlying type of shock, and the goal is always restoration of tissue perfusion, not merely a blood pressure number.
Step 1: Classify the Type of Shock
Understanding the hemodynamic profile determines the correct treatment.
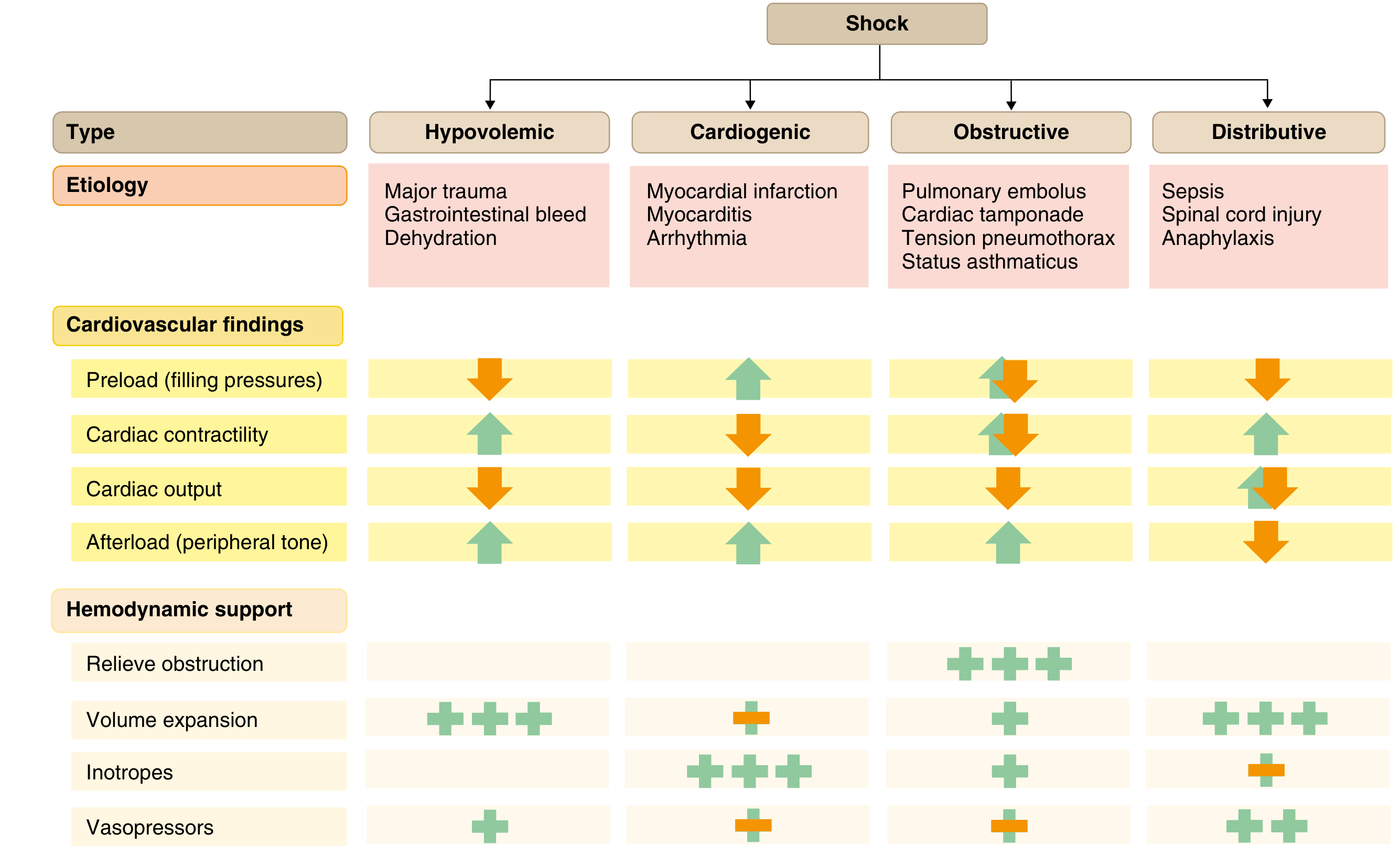
Goldman-Cecil Medicine — Causes, cardiovascular findings, and hemodynamic support for different shock types.
| Type | Examples | Preload | Contractility | Afterload |
|---|---|---|---|---|
| Hypovolemic | Hemorrhage, GI bleed, dehydration | ↓ | ↑ (compensatory) | ↑ |
| Cardiogenic | MI, myocarditis, arrhythmia | ↑ | ↓ | ↑ |
| Obstructive | PE, tamponade, tension pneumothorax | ↓ | ↓ | ↑ |
| Distributive | Sepsis, anaphylaxis, neurogenic | ↓ | ↑/variable | ↓ |
General Principles (All Shock Types)
- Airway & Oxygenation: Supplemental O₂ for all patients. Intubate early for severe hypotension, acidosis, or respiratory distress — do not delay for a trial of non-invasive ventilation.
- IV access: Large-bore peripheral or central access.
- Monitor: Arterial line for continuous BP; consider right heart catheterization when starting vasoactive agents in cardiogenic shock.
- Treat the cause: The definitive intervention is always etiology-specific (e.g., PCI for cardiogenic shock from MI, decompression for tension pneumothorax, source control for sepsis).
1. Hypovolemic Shock
Cornerstone: fluid resuscitation
- Isotonic crystalloids (normal saline or Ringer's lactate) — at least 30 mL/kg IV in sepsis-induced hypoperfusion; guided by hemodynamic response in hemorrhagic shock.
- Blood products for hemorrhage: packed RBCs; balanced transfusion (1:1:1 ratio of RBC:FFP:platelets) in massive hemorrhage.
- Vasopressors may be needed transiently while resuscitation proceeds but carry caution (increase afterload, risk of ischemia if underfilled).
- Control the source of bleeding.
2. Cardiogenic Shock
Cornerstone: restore myocardial perfusion + pharmacological support
- Small fluid bolus may be tried cautiously — but aggressive fluids worsen pulmonary edema.
- Vasopressors & Inotropes (titrated to BP and mixed venous O₂ saturation):
| Agent | Dose | Mechanism | Role |
|---|---|---|---|
| Norepinephrine | 0.02–1.0 µg/kg/min | α1 + mild β1 | Preferred vasopressor for cardiogenic shock; increases coronary flow |
| Dopamine | 3–10 µg/kg/min (inotrope); 10–20 µg/kg/min (vasopressor) | DA/β1/α1 | Second-line; more arrhythmias than NE |
| Dobutamine | 2.5–20 µg/kg/min | β1 selective | Inotrope of choice when SBP >90 mmHg; may worsen hypotension |
| Milrinone | 0.125–0.75 µg/kg/min (no load) | PDE inhibitor | Equivalent to dobutamine; long half-life, risk of hypotension |
| Epinephrine | 0.05–2 µg/kg/min | α + β | Reserve for refractory hypotension; more metabolic derangement |
| Vasopressin | 0.02–0.04 U/min | V1 receptor | Catecholamine-refractory cases |
- Revascularization (PCI) is the only intervention that consistently reduces mortality in cardiogenic shock from acute MI — outcomes are best within 6 hours of onset.
- Intra-aortic balloon pump (IABP): reduces systolic afterload, augments diastolic perfusion pressure — randomized trials show no mortality benefit with routine use; reserved for bridging to definitive therapy.
- Mechanical circulatory support (e.g., LVAD) if IABP fails.
3. Obstructive Shock
Cornerstone: relieve the obstruction
- Tension pneumothorax: immediate needle decompression → chest tube.
- Cardiac tamponade: pericardiocentesis.
- Massive PE: thrombolysis or catheter-directed therapy (systemic tPA if no contraindications); anticoagulation.
- Vasopressors and volume expansion are temporizing measures only.
4. Distributive Shock (Septic/Neurogenic/Anaphylactic)
Septic Shock
Surviving Sepsis Campaign (2016 guidelines, still in wide use):
| Priority | Intervention |
|---|---|
| 1st | IV crystalloid ≥30 mL/kg + norepinephrine as first vasopressor |
| 2nd | Add vasopressin (0.03 U/min) when NE dose escalates (0.25–0.5 µg/kg/min) |
| 3rd | Epinephrine as third agent |
| Adjunct | Hydrocortisone 200 mg/day if ongoing vasopressor requirement |
| Low CO component | Add dobutamine to NE, or switch to epinephrine |
- Norepinephrine is preferred over dopamine — the SOAP II trial (1679 patients) showed similar mortality but significantly more arrhythmias with dopamine; subgroup analysis showed improved survival with NE in cardiogenic shock.
- In vasodilatory shock, a target MAP of 65 mmHg is standard; lowering the target to 60–65 mmHg by reducing vasopressors is not clearly superior to standard care.
- Permissive hypotension strategies should be applied cautiously.
Anaphylactic Shock
- Epinephrine IM (0.3–0.5 mg, 1:1000) into the lateral thigh — first-line.
- IV fluids for volume depletion.
- Antihistamines (H1 + H2), corticosteroids as adjuncts.
- Second dose of epinephrine if no response within 5–15 min.
Neurogenic Shock (spinal cord injury)
- IV fluids first.
- Vasopressors (norepinephrine or phenylephrine) to restore vascular tone.
- Target MAP 85–90 mmHg for the first 7 days in acute spinal cord injury.
5. Orthostatic Hypotension (Chronic / Non-Shock)
The goal is symptom control, not a BP target.
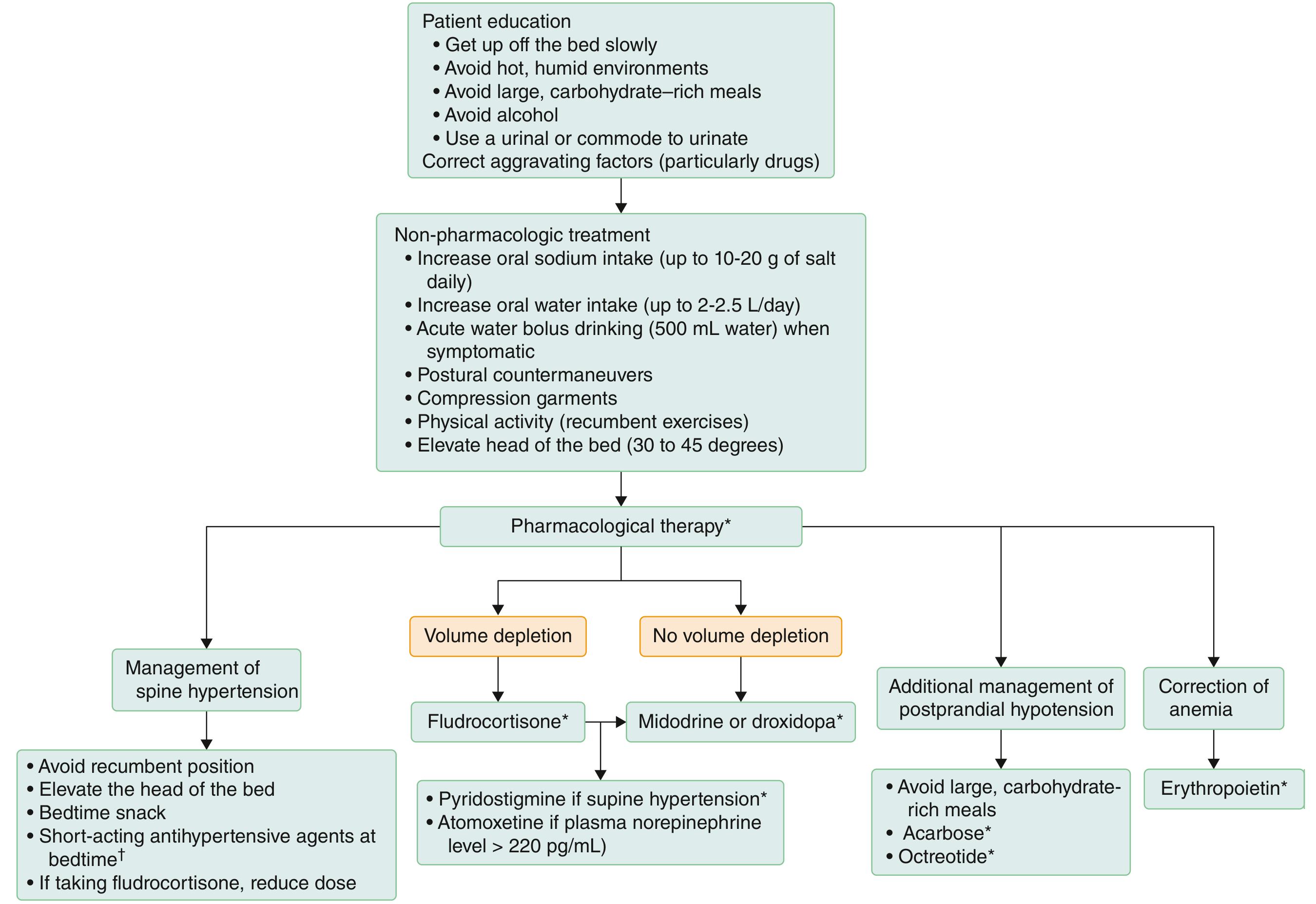
Goldman-Cecil Medicine — Stepwise approach to orthostatic hypotension.
Non-pharmacologic (first-line):
- Change positions gradually; sit briefly before standing.
- Increase fluid intake (2–2.5 L water/day) and salt (1–2 tsp daily or salt tablets 0.5–1.0 g).
- Avoid hot environments, alcohol, large carbohydrate-rich meals.
- Physical countermaneuvers: leg crossing, squatting, calf raises.
- Compression stockings (≥15–20 mmHg) or abdominal binder.
- Bolus water drinking (500 mL) for acute rescue — pressor effect within 5–10 min.
- Elevate head of bed 30–45°.
Pharmacologic:
| Drug | Dose | Mechanism | Notes |
|---|---|---|---|
| Fludrocortisone | 0.1–0.2 mg/day PO | Mineralocorticoid — expands volume | First-line with volume depletion; takes ≥7 days to work; watch for supine hypertension, hypokalemia |
| Midodrine | 5–10 mg TID PO | α1 agonist — arteriolar/venous constriction | Take before rising, before lunch, ≥3–4h before bedtime |
| Droxidopa | 100–600 mg TID PO | Converted to NE peripherally | Same timing as midodrine; for neurogenic OH |
| Pyridostigmine | 30–60 mg TID PO | AChE inhibitor — enhances ganglionic transmission | Increases standing BP without causing supine HTN |
| Atomoxetine | 10–18 mg BID PO | NE reuptake inhibitor | Best when sympathetic terminals preserved (MSA) |
| Acarbose | 50–100 mg before meals | Delays carbohydrate absorption | Adjuvant for postprandial hypotension |
| Octreotide | 0.2–0.4 µg/kg SQ | Splanchnic vasoconstriction | Adjuvant for postprandial hypotension |
| Erythropoietin | 25–75 U/kg SQ 3×/week | Increases RBC mass | When anemia contributes |
Key Vasopressor Drug Comparison Summary
| Drug | Receptor | Primary Effect | Best Use |
|---|---|---|---|
| Norepinephrine | α1 > β1 | Vasoconstriction + mild inotropy | First-line for distributive & cardiogenic shock |
| Vasopressin | V1 | Vasoconstriction | Second-line add-on to NE in septic shock |
| Dopamine | DA > β > α | Dose-dependent: inotrope/vasopressor | Second-line; avoid if arrhythmia risk |
| Dobutamine | β1 | Inotropy | Cardiogenic shock with adequate BP |
| Epinephrine | α + β | Vasoconstriction + inotropy | Anaphylaxis (1st line); refractory shock |
| Phenylephrine | α1 | Pure vasoconstriction | Neurogenic shock; avoid in low CO states |
| Milrinone | PDE inhibitor | Inotropy + vasodilation | Cardiogenic shock; beware of hypotension |
Sources: Goldman-Cecil Medicine (9780323930345) | Fuster & Hurst's The Heart, 15th Ed. (9781264257560) | Harrison's Principles of Internal Medicine 22E (9781265977061) | Washington Manual of Medical Therapeutics (9781975190620)
Non pharmacological managt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have rich, detailed content from three authoritative sources. Here is a comprehensive answer.
Non-Pharmacological Management of Hypotension
Non-pharmacological measures are the foundation of management — especially in orthostatic hypotension (OH), where they are sufficient alone for functional class I (asymptomatic/mild) and essential adjuncts in all stages before or alongside pharmacotherapy. The goal is to improve symptoms and prevent falls, syncope, and end-organ damage — not to hit a specific BP number.
1. Patient Education & Aggravating Factor Removal
This is always the first step.
- Review and adjust medications that worsen hypotension: diuretics, antihypertensives, tricyclic antidepressants, antipsychotics, dopamine agonists, alpha-blockers, nitrates, sildenafil.
- Address correctable comorbidities: iron deficiency, vitamin B12/D deficiencies, anaemia, dehydration, frailty.
- Educate the patient about the mechanism — understanding triggers helps enormously with self-management.
2. Positional & Behavioural Measures
Postural Precautions
- Rise slowly: sit at the edge of the bed for 30–60 seconds before standing; dangle the legs first.
- Avoid Valsalva maneuvers (straining at stool, heavy lifting) — these transiently reduce venous return.
- Urinate sitting down or use a urinal — avoids the combination of straining and standing.
- Avoid prolonged standing: shift weight, move around rather than standing still.
Environmental Avoidance
- Avoid hot, humid environments (cause cutaneous vasodilation — the main exacerbating factor in warm weather).
- Avoid prolonged hot baths or showers — warm water causes vasodilation; consider cooler showers or bathing seated.
- Avoid alcohol (a powerful vasodilator) — if consumed, restrict to the evening before bedtime.
3. Physical Countermaneuvers
These maneuvers use muscle pump action or gravity reduction to acutely raise venous return and blood pressure. They are entirely under the patient's control and highly effective — many patients discover them on their own before diagnosis.
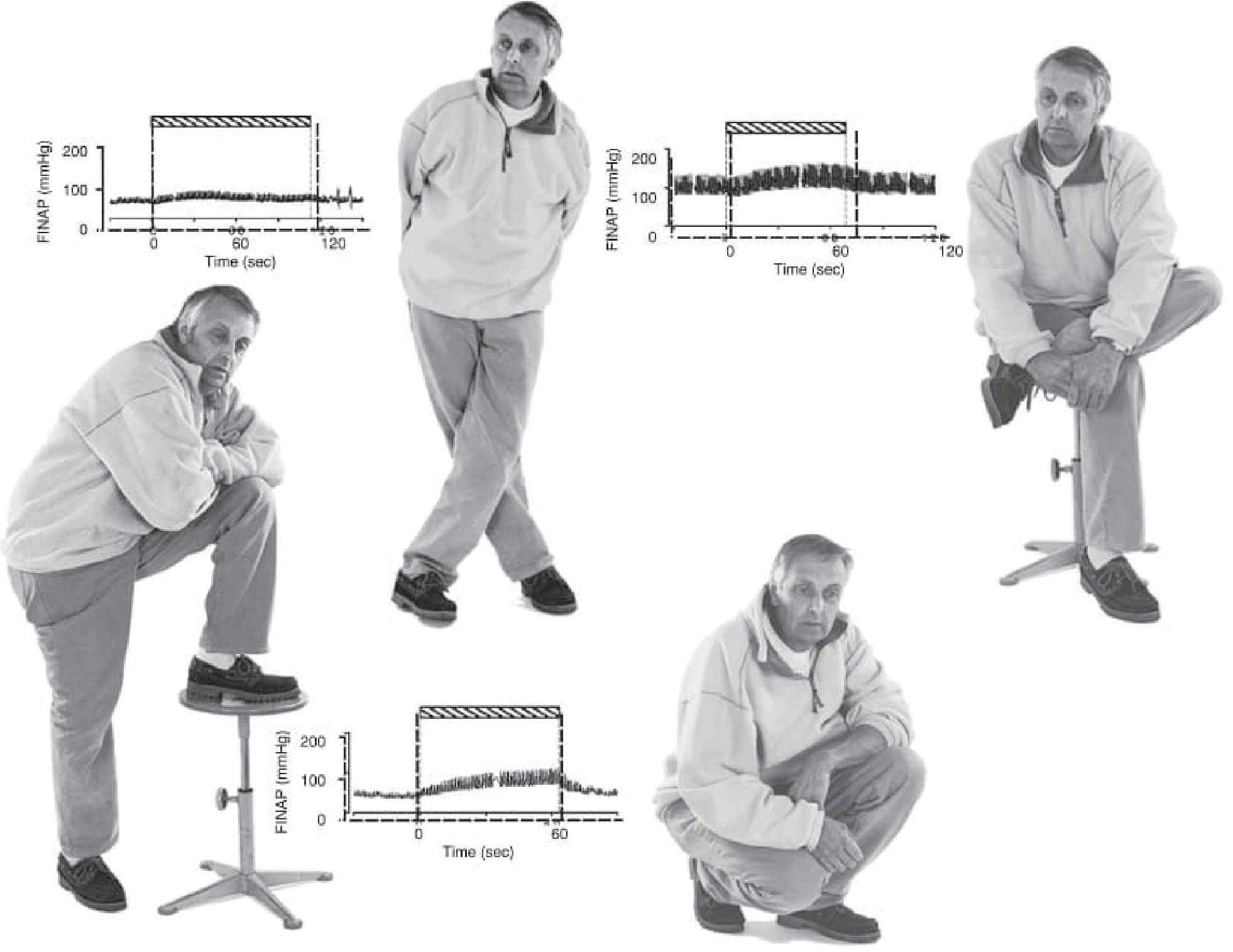
Bradley & Daroff's Neurology — Blood pressure (FINAP) response to physical countermaneuvers in a patient with pure autonomic failure: leg crossing, foot on chair, and squatting all produce prompt BP elevation.
| Maneuver | Mechanism | Notes |
|---|---|---|
| Leg crossing (standing) | Squeezes venous vessels in legs and abdomen → reduces venous pooling; lean forward slightly to enhance benefit | Most practical; can be sustained; caution in patients with balance problems (MSA) |
| Leg crossing (seated) | Similar mechanism; effective even seated | Most useful in severe OH where even sitting is challenging |
| Squatting | Reduces venous capacity in legs and splanchnic bed; creates mechanical impediment to leg arterial flow | Very powerful acute rescue maneuver; caution when rising from squat |
| Standing on tiptoes | Calf muscle pump activation | Simple; can be done anywhere |
| Buttock clenching | Isometric lower limb contraction | Easy to perform discreetly |
| Stooping / bending forward | Increases intra-abdominal pressure; reduces effective gravitational gradient | Useful when feeling faint |
4. Fluid & Salt Loading
Water (Bolus Drinking)
- 500 mL (16 oz) of plain water drunk rapidly is a potent acute pressor maneuver.
- BP rises by 30–40 mmHg on average (occasional patients see +80 mmHg or more).
- Onset: ~5 minutes; peak: 30–40 minutes; duration: ~90 minutes.
- Works via a spinal sympathoexcitatory reflex triggered by portal osmoreceptors — this effect is present only when baroreflex regulation is impaired (aging, neurodegenerative disorders).
- Hypotonic (plain) water works best — sugar or salt in beverages attenuates the pressor effect.
- Ideal timing:
- Immediately on waking (before standing)
- Before meals in postprandial hypotension
- Before activities requiring prolonged standing
Chronic Fluid Intake
- Target 2–3 L of water/day to maintain adequate plasma volume.
- Monitor weight and BP; check 24-hour urinary sodium before and after starting a salt load.
Dietary Sodium
- Target 6–10 g of sodium/day (approximately 2 g salt three times daily, or 1–2 teaspoons added to food).
- Raising 24-hour urinary sodium to ~185 mmol is a reasonable target.
- Works chronically by expanding extracellular fluid volume.
- Available as salt tablets (0.5–1.0 g); may cause abdominal discomfort.
- POTS patients typically need 2 g at 8 AM and 2 g at 2 PM (covers waking hours when upright; duration of action ~4–5 hours).
- Contraindicated in heart failure, severe hypertension, or renal failure.
5. Dietary Modifications
- Eat smaller, more frequent meals low in carbohydrates — postprandial hypotension (occurring within 2 hours of eating) is driven by insulin-triggered splanchnic vasodilation.
- Avoid large carbohydrate-rich or high-sugar meals — sweets and desserts are the most potent BP depressants.
- Avoid alcohol with meals — the combination of postprandial vasodilation and alcohol-induced vasodilation is especially dangerous.
- Plan activities before eating rather than after (e.g., shopping first, then eating).
- Caffeine (coffee/tea) in the morning can blunt postprandial hypotension — useful as an adjunct.
6. Compression Garments
- Graduated compression stockings: high-waist (thigh-high) stockings providing ≥15–20 mmHg compression reduce venous pooling in the legs, increase venous return, and raise BP.
- Must be applied before getting out of bed — put on while still lying down.
- Remove when lying down (to preserve effectiveness in the upright posture).
- Disadvantage: inconvenient; many patients find them uncomfortable, particularly in warm climates.
- Best reserved for special occasions (e.g., when prolonged standing is required) in patients who find daily use impractical.
- Abdominal binder: very effective at reducing splanchnic blood pooling (the largest venous reservoir).
- Often more practical than full-length stockings.
- Particularly useful in neurogenic OH.
7. Exercise & Physical Conditioning
- Deconditioning worsens OH — patients should not stop exercising.
- Preferred modes:
- Recumbent or seated exercise (recumbent cycling, rowing)
- Water aerobics / water jogging in shoulder-deep water — water reduces the gravitational pull on blood volume to ~¼ of its normal value, allowing exercise with minimal orthostatic stress.
- Swimming pool exercise preferred; cooler water temperatures are better (warm water → cutaneous vasodilation).
- Caution: great care when exiting the pool — full gravitational pull returns with a vasodilated muscular (and possibly cutaneous) system.
- Orthostatic (tilt) training for recurrent reflex syncope:
- Lean upright with back against a wall, feet ~30 cm from the wall (simulating ~70° head-up tilt).
- Duration: 10–20 minutes, once or twice daily.
- Performed on carpeted floor away from sharp furniture.
- Evidence: promising in open-label trials; worth attempting for OH and POTS as well.
8. Sleeping Position
- Elevate the head of bed by 30–45° (using bed risers, wedge pillow, or raising the headboard).
- Prevents nocturnal supine hypertension, which causes pressure diuresis and volume loss during sleep → worsened morning OH.
- Reduces overnight diuresis by maintaining mild head-up tilt, thereby preserving intravascular volume on waking.
- Also stimulates the renin-angiotensin-aldosterone system overnight, providing some volume protection.
Summary Framework
Step 1: Remove aggravating factors (drugs, comorbidities)
Step 2: Patient education (positional awareness, trigger avoidance)
Step 3: Fluid & salt loading (2–3 L water/day; 6–10 g Na/day)
Step 4: Dietary modification (small meals, low-carb, avoid alcohol)
Step 5: Compression garments (abdominal binder ± thigh-high stockings)
Step 6: Physical countermaneuvers (leg crossing, squatting, tiptoes)
Step 7: Exercise prescription (recumbent/pool-based)
Step 8: Head-of-bed elevation (30–45°)
Step 9: Orthostatic training (tilt training for reflex syncope/POTS)
↓ if still symptomatic
Pharmacological therapy
Sources: Goldman-Cecil Medicine (9780323930345) | Bradley & Daroff's Neurology in Clinical Practice (9780323642613) | Harrison's Principles of Internal Medicine 22E (9781265977061)
This is a shared conversation. Sign in to Orris to start your own chat.