Draw labeled diagram of layers of cornea. Clinical features, investigations management of corneal ulcer
Reading File
Finding Sources
Finding Sources
Generating Image
Labeled cross-section diagram of the layers of the cornea, showing from anterior to posterior: Epithelium (stratified squamous, 5 layers), Bowman's layer (anterior limiting membrane), Stroma (90% of corneal thickness, collagen lamellae), Descemet's membrane (posterior limiting membrane), Endothelium (single cell layer). Clean medical illustration style with clear labels and arrows, white background.
Searching PubMed
corneal ulcer management treatment
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compile the full answer.
Layers of the Cornea
Labeled Diagram
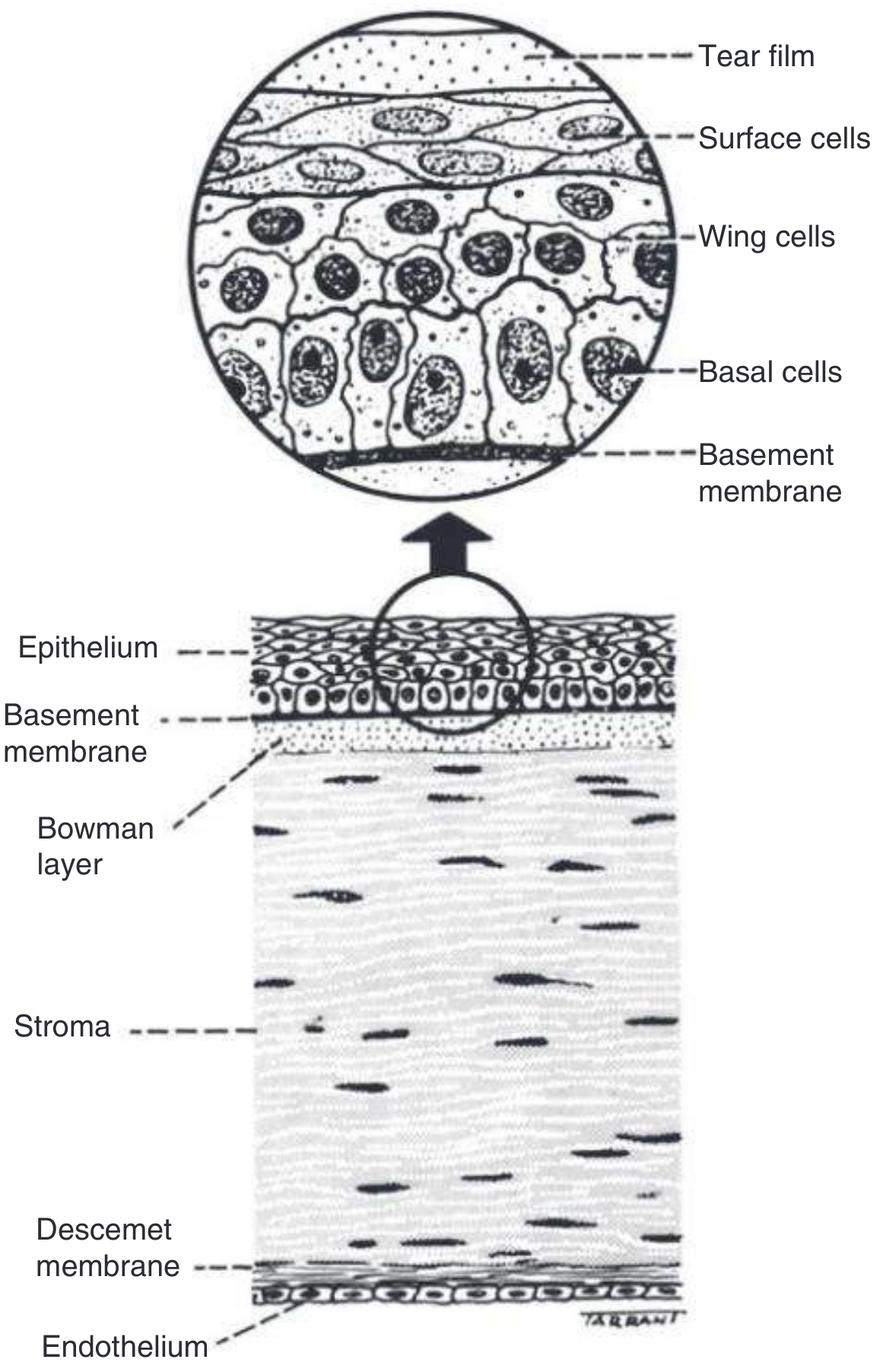
From Kanski's Clinical Ophthalmology (Fig. 7.1) — Anatomy of the Cornea:
Generated diagram for clarity:
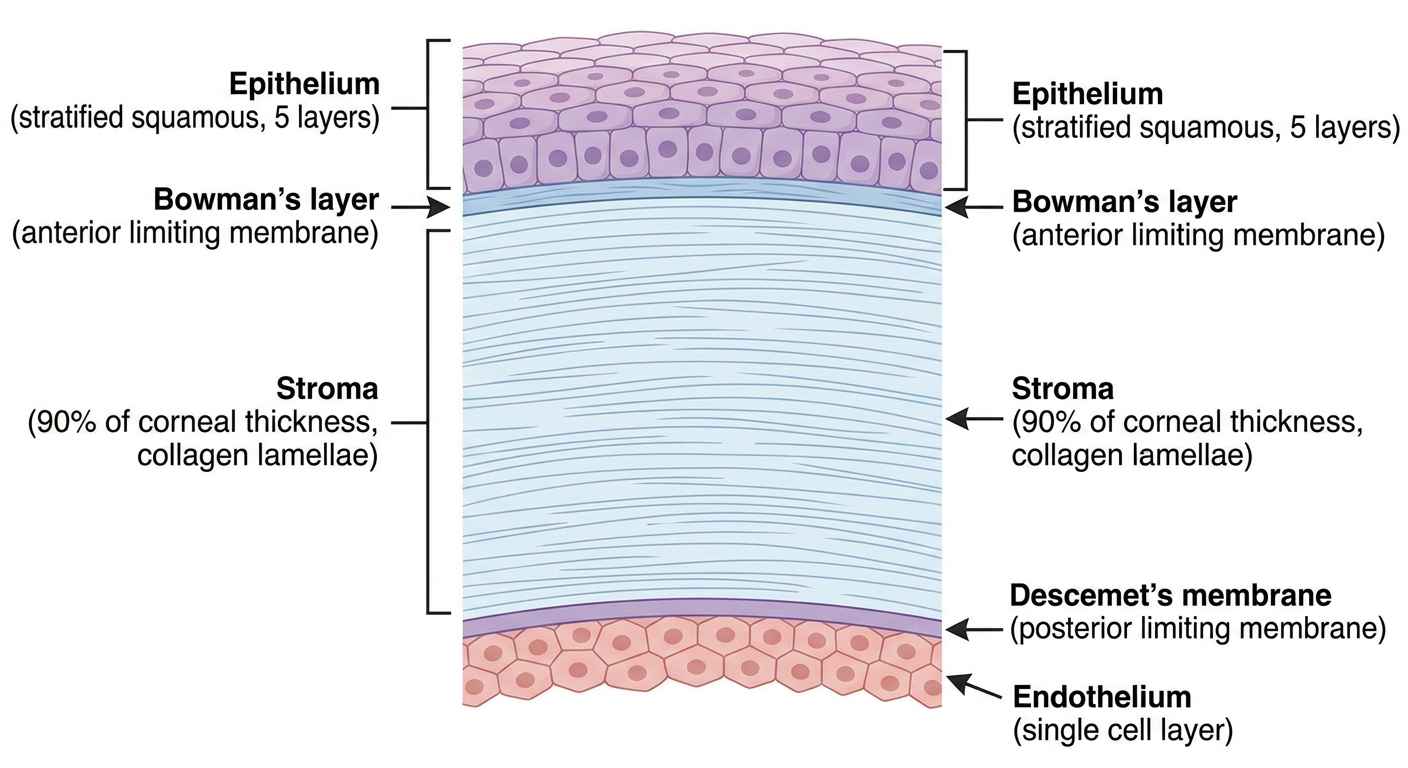
The Five Layers of the Cornea
The cornea is ~0.5 mm thick centrally and ~1 mm peripherally. It consists of three cellular layers separated by two acellular membranes:
| Layer | Key Features |
|---|---|
| 1. Epithelium | Non-keratinized stratified squamous epithelium, ~50 μm thick (~5 cell layers). Cells arranged as: surface squamous cells → wing cells → basal columnar cells resting on basement membrane. Remarkable regenerative capacity (turnover ~7 days). Stem cells reside at the corneoscleral limbus. |
| 2. Bowman's Layer (Anterior Limiting Membrane) | Acellular; superficial condensed layer of the stroma composed of collagen fibres. Cannot regenerate — scarring is permanent once damaged. |
| 3. Stroma | Constitutes ~90% of corneal thickness. Regularly arranged orthogonal collagen lamellae (types I & V) spaced by proteoglycan ground substance (keratan sulphate, chondroitin sulphate) with interspersed keratocytes. Regular spacing is critical for optical transparency. Can scar but cannot fully regenerate. |
| 4. Descemet's Membrane (Posterior Limiting Membrane) | Discrete sheet of collagen fibrils distinct from stromal collagen. Has an anterior banded zone (deposited in utero) and a posterior non-banded zone (laid down throughout life). Has regenerative potential. Serves as basement membrane for endothelium. |
| 5. Endothelium | Single monolayer of polygonal cells. Maintains corneal deturgescence by active fluid pumping. Young adult density ~3,000 cells/mm². Declines ~0.6%/year; at <500 cells/mm², corneal oedema develops. Cannot regenerate. |
Dua's Layer: A recently proposed 6th layer (15 μm thick, between stroma and Descemet's membrane), though its distinctness is still debated.
— Kanski's Clinical Ophthalmology, 10th ed.; Histology: A Text and Atlas (Wojciech Pawlina)
Corneal Ulcer
Definition
A corneal ulcer is a serious infection involving multiple layers of the cornea — it develops secondary to breaks in the epithelial barrier, allowing infectious agents to invade the underlying corneal stroma.
Aetiology / Causative Organisms
| Category | Organisms |
|---|---|
| Bacteria | Pseudomonas aeruginosa (contact lens wearers), S. pneumoniae, S. aureus, Moraxella spp., Streptococcus |
| Viruses | Herpes simplex virus (HSV), Varicella zoster virus |
| Fungi | Candida, Aspergillus, Penicillium, Cephalosporium (Acremonium) |
| Protozoa | Acanthamoeba (contact lens wearers, water exposure) |
Predisposing factors: contact lens wear (especially extended-wear/overnight), corneal trauma, previous ocular surgery, immunosuppression, Bell's palsy/exposure keratitis, topical steroid use.
Clinical Features
Symptoms
- Red eye with conjunctival/ciliary injection
- Moderate-to-severe ocular pain / foreign body sensation
- Photophobia (consensual photophobia due to ciliary spasm from associated iritis)
- Decreased visual acuity (if ulcer is in visual axis or significant uveal inflammation)
- Mucopurulent discharge
- Acute contact lens intolerance
Signs
| Feature | Description |
|---|---|
| Corneal infiltrate | Round/irregular white, hazy stromal opacity with heaped-up edges |
| Epithelial defect | Stains with fluorescein; loss of epithelium overlying infiltrate |
| Stromal thinning | Tissue loss in stroma; slit beam cannot see through infiltrate to iris |
| Anterior chamber reaction | Flare and cells; hypopyon (sterile or infected) in severe cases |
| Miotic pupil | Due to iritis/ciliary spasm |
| Lid/conjunctival changes | Erythema, oedema, mucopurulent discharge |
Organism-specific features:
- Staphylococcal: well-defined, grey-white stromal infiltrate → dense stromal abscess
- Streptococcal: fulminant with severe hypopyon, or crystalline (in chronic steroid users)
- Pseudomonas: rapidly progressive, suppurative, necrotic infiltrate + hypopyon + mucopurulent discharge; can cause corneal melting and perforation
- Moraxella: indolent, inferior cornea, full-thickness, immunocompromised host
- Fungal: feathery borders, satellite lesions; history of vegetable/plant trauma
- Acanthamoeba: extreme pain, perineural invasion, ring infiltrate in late stages; swimming/contact lens history
Investigations
-
History: Contact lens type and care, water exposure, trauma, prior surgery, systemic illness, steroid/immunosuppressant use
-
Slit lamp examination:
- Fluorescein staining to map epithelial defect
- Document size, depth, and location of infiltrate
- Assess anterior chamber reaction (flare, cells, hypopyon size)
- Measure IOP (Tono-Pen preferred)
-
Corneal scrapings (culture if infiltrate >1–2 mm, in visual axis, unresponsive to treatment, or unusual organism suspected):
- Gram stain — bacteria
- Giemsa stain — Acanthamoeba cysts, fungi
- KOH preparation / Calcofluor white — fungi, Acanthamoeba
- Culture media: Blood agar, chocolate agar, Sabouraud's (fungi), non-nutrient agar with E. coli lawn (Acanthamoeba), Löwenstein-Jensen (atypical mycobacteria — keep 8 weeks)
-
Contact lens and case cultures (in contact lens wearers)
-
Confocal microscopy: For detecting Acanthamoeba cysts in vivo
The diagnosis is primarily clinical; cultures confirm the organism and guide targeted therapy.
Management
General Principles
- Treat empirically as bacterial until proven otherwise
- Initial therapy must be broad-spectrum
- Do NOT patch the eye (increases risk of Pseudomonas infection → corneal melting and perforation)
- Refer to ophthalmologist within 12–24 hours
Step-by-Step Treatment
1. Cycloplegia
- Cyclopentolate 1% t.i.d. — relieves ciliary spasm, prevents posterior synechiae
- Atropine 1% b.i.d.–t.i.d. if hypopyon is present
2. Topical Antibiotics (risk-stratified)
| Risk Level | Criteria | Treatment |
|---|---|---|
| Low risk | Small peripheral infiltrate, no/minimal AC reaction | Fluoroquinolone (moxifloxacin, gatifloxacin, ciprofloxacin) q1–2h while awake; or polymyxin B/trimethoprim |
| Borderline risk | 1–1.5 mm peripheral, or any with epithelial defect/mild AC reaction | Fluoroquinolone q1h around the clock ± polymyxin B/trimethoprim q1h. Loading: 1 drop q5 min × 5 doses → q30 min → q1h |
| Vision-threatening | >1.5–2 mm, in visual axis, or unresponsive to initial Rx | Fortified antibiotics: Fortified tobramycin/gentamicin (15 mg/mL) q1h alternating with fortified cefazolin (50 mg/mL) q1h (drop every 30 min around the clock). If MRSA suspected: substitute vancomycin (25 mg/mL). If Pseudomonas suspected: add fortified ceftazidime q1h |
3. Specific Infections
- Fungal: Natamycin 5% (filamentous), amphotericin B (Candida), voriconazole; consider intrastromal antifungal injections (ophthalmologist)
- HSV: Topical acyclovir/ganciclovir; systemic acyclovir for stromal disease
- Acanthamoeba: PHMB (polyhexamethylene biguanide) + propamidine (Brolene) for several months
- Bacterial coinfection may complicate fungal/Acanthamoeba keratitis — broaden accordingly
4. Adjunctive Measures
- Topical steroids: Relatively contraindicated in viral infections; may reduce scarring/perforation risk in bacterial keratitis but only under ophthalmologist guidance; never initiate in the ED without ophthalmology advice
- Corneal thinning: Protect with a shield (no patch). Add doxycycline 100 mg p.o. b.i.d. (MMP inhibitor) + vitamin C (collagen synthesis promoter)
- IOP management: If raised, topical β-blocker or carbonic anhydrase inhibitor (avoid prostaglandins)
Surgical Management
| Indication | Procedure |
|---|---|
| Non-healing/refractory ulcer | Therapeutic penetrating keratoplasty (PKP) |
| Impending perforation | Tissue adhesive (cyanoacrylate), amniotic membrane graft, or emergency PKP |
| Corneal perforation | Emergency PKP or patch graft |
Complications
- Corneal scarring → permanent visual impairment
- Corneal perforation → endophthalmitis
- Anterior and posterior synechiae
- Secondary glaucoma
- Cataract
- Phthisis bulbi (end-stage)
Sources: Tintinalli's Emergency Medicine (9th ed.); The Wills Eye Manual (7th ed.); Kanski's Clinical Ophthalmology (10th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.