Severe headache which was triggered by going up a flight of stairs, which led to some calf muscle soreness in the moment and a pulsation or a pulsating sensation in the head, as if blood is being pumped harder into my head. The headache was gradually progressive, throbbing in nature. It's experienced on all the aspects of the head. It gets worse on suddenly changing the position of my head.
exertional headache diagnosis
Exertion-Triggered Headache - Clinical Analysis
Diagnostic Approach: New vs. Old Headache
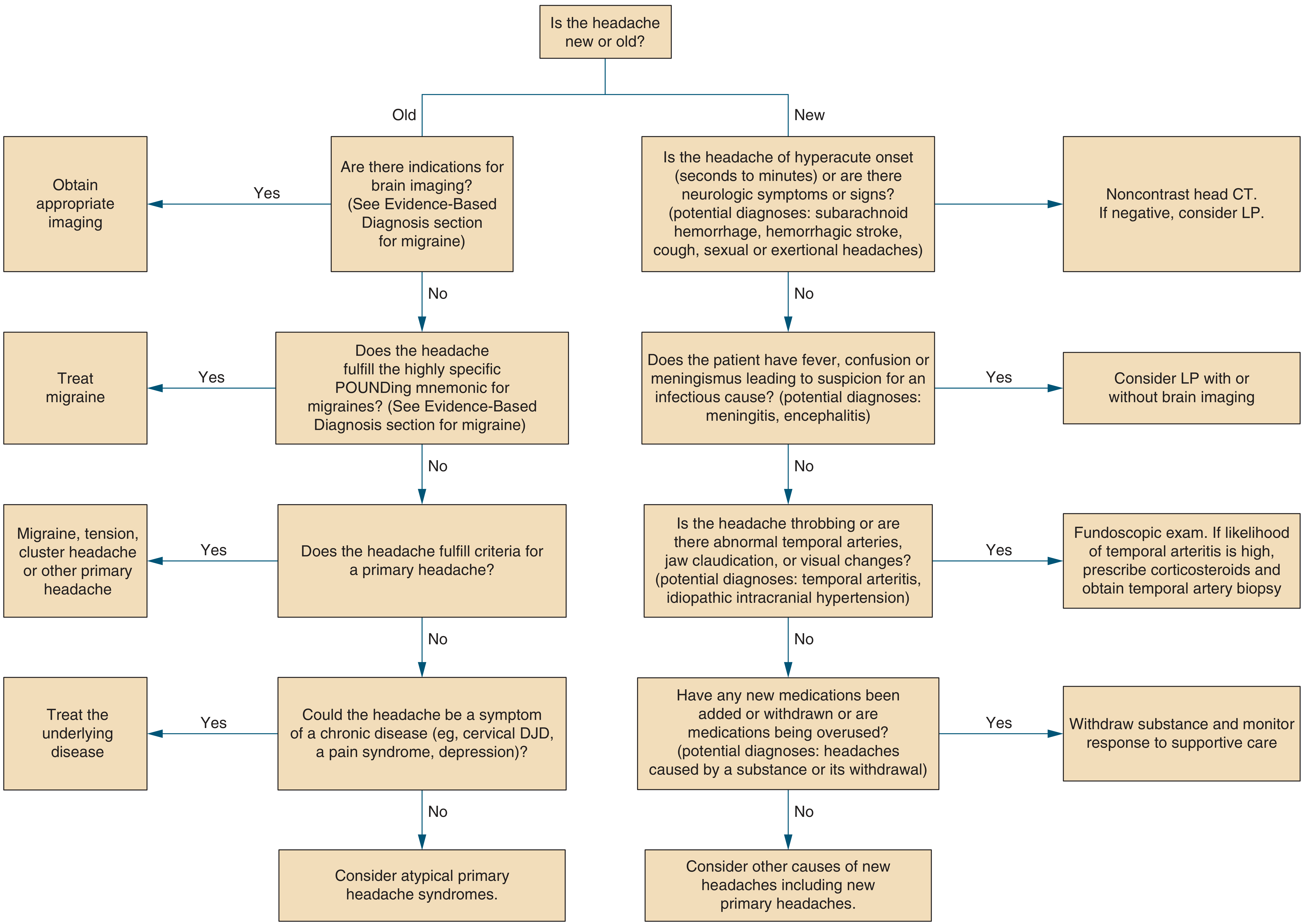
The "Must Not Miss" Diagnoses First
1. Subarachnoid Hemorrhage (SAH) - Highest Priority
"Onset of thunderclap headache during periods of exertion raises suspicion for subarachnoid hemorrhage or arterial dissection of the carotid or vertebrobasilar circulation."
- Age ≥40 years
- Neck pain or stiffness
- Witnessed loss of consciousness
- Onset during exertion ✓ (present in this case)
- Thunderclap headache (peak pain within 1 second)
- Limited neck flexion on examination
2. Reversible Cerebral Vasoconstriction Syndrome (RCVS)
3. Arterial Dissection
Primary (Benign) Diagnoses - After Excluding Dangerous Causes
4. Primary Exertional Headache (Benign Exertional Headache)
"A patient may complain of very severe, transient cranial pain on coughing, sneezing, laughing heartily, lifting heavy objects, stooping, and straining at stool... The pain is often described as having a bursting quality... Most often this syndrome is a benign idiopathic state that recurs over a period of several months to a year or two and then disappears."
5. Migraine Triggered by Exertion
The Position-Change Worsening - An Important Clue
- Raised intracranial pressure - from any space-occupying lesion, hemorrhage, or CSF outflow obstruction
- Colloid cyst of the third ventricle - classically causes positional headache and can present acutely
- Cerebral venous sinus thrombosis - another exertional/positional headache entity
Red Flag Summary ("SNOOP4" Features Present)
| Red Flag | Present? |
|---|---|
| Systemic symptoms or disease | Not mentioned |
| Neurologic symptoms/signs | Not mentioned |
| Onset sudden/thunderclap | Exertional onset - YES |
| Older age (>50 new headache) | Unknown |
| Progressive pattern | YES - gradually progressive |
| Postural aggravation | YES - worse with position change |
| Precipitated by exertion/Valsalva | YES |
| Papilledema | Not assessed |
Recommended Workup
- Noncontrast head CT - immediately, to exclude hemorrhage
- LP with xanthochromia assessment - if CT is negative but suspicion for SAH remains (CT misses ~2% of SAHs at 6 hours, more at later presentation)
- CT angiography or MR angiography - to evaluate for aneurysm, arterial dissection, RCVS, or venous sinus thrombosis
- Blood pressure measurement - malignant hypertension can also cause exertional pulsating headache
Important note: This analysis is for educational purposes. A new severe exertional headache with positional aggravation requires in-person medical evaluation - ideally in an emergency setting - to rule out hemorrhagic and vascular causes before any diagnosis of a benign primary headache disorder can be made.
If I try to press my hand or even touch it, slightly makes it worse.
Cutaneous Allodynia - What Your Symptom Means
"The allodynic migraineur experiences pain or discomfort with normally nonnoxious stimulation of the skin, such as occurs with light touch of the face or scalp, wearing eyeglasses, shaving the face, and wearing a tight collar or necklace."
Why This Happens - Central Sensitization
What This Tells Us Diagnostically
- Cutaneous allodynia develops in approximately two-thirds of migraineurs during an attack - it is one of the most characteristic features of migraine pathophysiology
- Combined with your earlier symptoms - throbbing/pulsating quality, gradually progressive intensity, holocephalic distribution, worsening with movement/position change, and exertional trigger - the allodynia rounds out a picture very consistent with migraine
- The scalp vessels themselves can become distended and tender during a migraine attack, which further explains the touch-sensitivity
-
Treatment timing is critical. The presence of allodynia during an attack predicts a less robust response to acute treatments (like triptans). Triptans work best when taken early in the attack - before central sensitization sets in. Once allodynia is present, the window for optimal acute treatment may have partially closed.
-
Risk of chronification. A history of allodynia increases the risk of migraine becoming chronic (more than 15 headache days per month). This is a flag to discuss with a neurologist.
-
Treatment implication. If attacks with allodynia become frequent, onabotulinumtoxinA (Botox) for chronic migraine has actually shown a more favorable response in allodynic migraineurs specifically.
Does This Change the "Must Not Miss" Picture?
| Feature | Migraine Allodynia | SAH Meningeal Irritation |
|---|---|---|
| Timing | During established headache | Often alongside worst-of-life onset |
| Neck stiffness | Usually absent | Classic finding |
| Touch sensitivity | Scalp, face, hair | Neck movement most prominent |
| Photophobia/nausea | Very common | Can occur |
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology, 12th Ed.
Let's assume that it is a migraine. How do we treat this episode and prevent further future episodes?
"migraine"[MeSH Terms] AND "treatment"[MeSH Terms]
Migraine Treatment: Acute Episode + Prevention
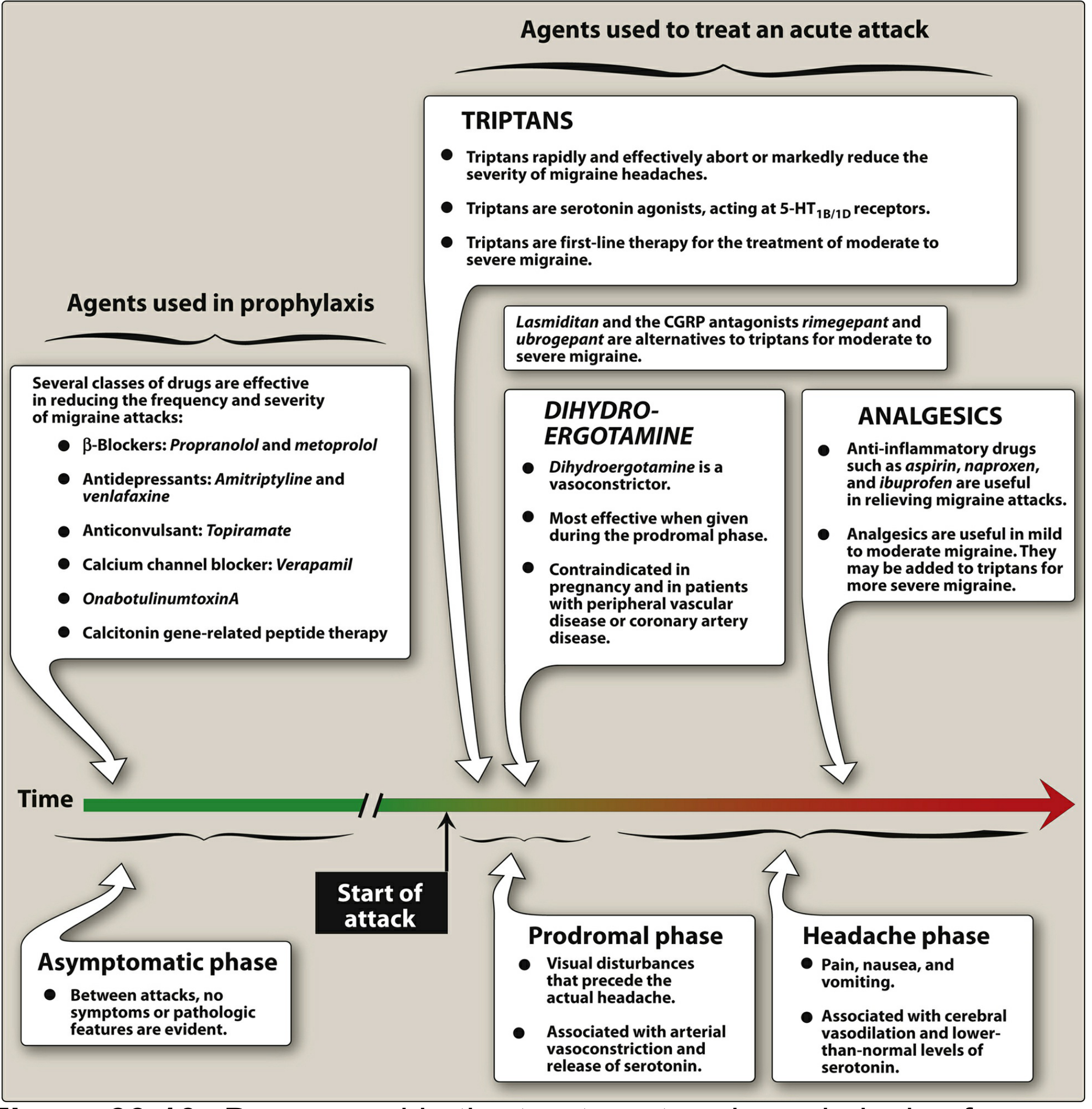
Part 1: Treating This Episode (Acute/Abortive Treatment)
Step-Up Strategy
Mild-to-Moderate Attack: Non-Specific Analgesics First
| Drug | Dose | Notes |
|---|---|---|
| Ibuprofen | 400 mg q3-4h | First choice NSAID |
| Naproxen | 220-550 mg twice daily | Longer-acting, also reduces recurrence |
| Aspirin + acetaminophen + caffeine | 2 tablets | (e.g., Excedrin Migraine) - caffeine enhances absorption |
Moderate-to-Severe Attack: Triptans (First-Line Specific Therapy)
| Triptan | Route | Dose | Notes |
|---|---|---|---|
| Sumatriptan | Oral | 50-100 mg at onset | Prototype; also SC (6 mg) and nasal (20 mg) |
| Rizatriptan | Oral | 5-10 mg at onset | Among the most efficacious |
| Eletriptan | Oral | 40 or 80 mg at onset | High efficacy on a population basis |
| Zolmitriptan | Oral/nasal | 2.5 mg at onset | Flexible formulations |
| Frovatriptan | Oral | 2.5 mg at onset | Longest half-life (>24h); fewer recurrences |
| Almotriptan | Oral | 12.5 mg at onset | Well tolerated |
| Naratriptan | Oral | 2.5 mg at onset | Slower onset, well tolerated |
- Rizatriptan and eletriptan are the most effective on a population basis
- Faster onset = better effect: sumatriptan SC (onset ~20 min) beats oral (1-2 hours); clinical efficacy relates more to time-to-peak plasma level than potency
- Adding naproxen 500 mg to sumatriptan both augments the initial effect AND significantly reduces headache recurrence - this combination is well-supported by RCT evidence
- Do not use triptans in patients with ischemic cardiac, cerebrovascular, or peripheral vascular disease (they are vasoconstrictors)
- If one triptan fails, try a different one - individual responses vary considerably
What About the Allodynia/Timing Problem?
- Subcutaneous sumatriptan (SC) is preferred - it bypasses gastric stasis (which also occurs during migraine) and achieves peak levels in ~12 minutes
- Nasal sumatriptan or zolmitriptan are the next-best non-oral options
If Triptans are Contraindicated or Unavailable: Alternatives
- Lasmiditan (ditan, 5-HT1F agonist) - does NOT cause vasoconstriction, so safe in cardiovascular disease; classified as a controlled substance; do not drive after taking it
- Gepants (CGRP receptor antagonists):
- Ubrogepant or Rimegepant - oral, for acute treatment; no vasoconstriction; safe with cardiovascular risk factors
- Rimegepant can also serve double-duty for prevention
Antiemetics
- Prochlorperazine - both controls nausea and has independent analgesic properties in migraine
- Metoclopramide - also helps with gastric stasis, improving absorption of oral medications
Ergot Alkaloids (Older Agents)
Non-Pharmacological Measures During an Attack
- Lie in a dark, quiet room (photophobia and phonophobia are expected)
- Cold or warm compress on the forehead/scalp (whichever is more comfortable)
- Hydration
- Sleep, if possible - migraine often resolves after sleep
Part 2: Preventing Future Episodes
Indications to Start Prevention
- ≥2 attacks/month that impair daily function
- Attacks lasting >48 hours
- Rescue medications needed >2 days/week (risk of medication-overuse headache)
- Presence of allodynia (risk of chronification)
- Attacks triggered predictably by exertion (as in this case - prophylaxis before exercise is a specific strategy)
First-Line Preventive Agents
1. Beta-Blockers (Drugs of Choice)
- Propranolol: 40-240 mg/day (divided doses)
- Especially relevant here: for exertional migraine, propranolol taken before exercise has direct clinical evidence of preventing attacks (as noted in Symptom to Diagnosis for the clinical case of exertional headache treated with pre-exercise propranolol)
- Avoid in asthma, severe bradycardia, or depression
2. Anticonvulsants
- Topiramate (25-200 mg/day) - Level A evidence; also causes weight loss (useful if weight is a trigger); can cause cognitive slowing ("dopamax" effect) and kidney stones
- Valproate/Divalproex (500-1500 mg/day) - effective; avoid in women of childbearing age (teratogenic); causes weight gain
3. Antidepressants
- Amitriptyline (10-150 mg nightly) - tricyclic; works independently of mood effect; sedating at night (beneficial for sleep disruption in migraine); also treats comorbid depression and tension-type headache
- Venlafaxine (SNRI) - evidence for migraine prevention, better tolerated than amitriptyline
4. Calcium Channel Blockers
- Verapamil - moderate evidence; useful if beta-blockers are contraindicated
Newer/Specialized Preventive Agents
5. CGRP Monoclonal Antibodies (Injectable, Monthly or Quarterly)
| Agent | Target | Dosing |
|---|---|---|
| Erenumab | CGRP receptor | 70-140 mg SC monthly |
| Galcanezumab | CGRP ligand | 120 mg SC monthly (240 mg loading) |
| Fremanezumab | CGRP ligand | 225 mg SC monthly or 675 mg quarterly |
| Eptinezumab | CGRP ligand | 100-300 mg IV quarterly |
6. OnabotulinumtoxinA (Botox)
- Approved specifically for chronic migraine (≥15 headache days/month)
- 155 units injected across 31 sites on the head and neck, every 12 weeks
- Particularly effective in patients with allodynia - which this patient has
- Not useful for episodic migraine (fewer than 15 days/month)
7. Oral CGRP Antagonists for Prevention
- Rimegepant (75 mg every other day) and atogepant - dual-use: acute treatment AND prevention
Lifestyle and Trigger Management (Non-Pharmacological Prevention)
| Strategy | Specifics |
|---|---|
| Regular sleep schedule | Irregular sleep is a major trigger |
| Consistent meal timing | Skipped meals = hypoglycemia trigger |
| Hydration | Dehydration is a common trigger |
| Exercise pacing | Warm up gradually before exercise; avoid sudden intense exertion |
| Stress management | CBT, biofeedback, and relaxation training have RCT support |
| Headache diary | Identify personal triggers (foods, hormones, weather, sleep) |
| Caffeine regulation | Both excess and withdrawal trigger migraine |
| Medication overuse awareness | Taking acute treatment >2 days/week leads to rebound headaches |
Summary Decision Framework
Acute attack:
Mild → NSAID (ibuprofen/naproxen ± caffeine)
Moderate → Triptan (rizatriptan or eletriptan oral) + naproxen
Severe → Sumatriptan SC or DHE nasal/injection
Allodynia present → prefer SC/nasal route; add antiemetic
CV contraindication → gepant (ubrogepant/rimegepant) or lasmiditan
Prevention:
First-line → Propranolol or topiramate or amitriptyline
Exertional → Pre-exercise propranolol specifically
Refractory → CGRP monoclonal antibody
Chronic (≥15d/mo) → OnabotulinumtoxinA ± CGRP mAb
Does whether the headache respond to paracetamol or not give us a clue as to the etiology?
Does Paracetamol Response Tell Us the Etiology?
"Improvement of the patient's pain with treatment does not predict benign cause of headache."
Why Response to Paracetamol is Misleading
1. Serious Causes Can Respond to Paracetamol
- Activating descending serotonergic pain-modulation pathways in the CNS
- Inhibiting prostaglandin synthesis centrally
2. Migraine Can Fail to Respond to Paracetamol
"Failed NSAIDs/analgesics → First tier: Sumatriptan 50-100 mg"
Where Analgesic Response Has Some (Limited) Signal
| Scenario | What It Suggests | Strength of Signal |
|---|---|---|
| Headache completely abolished by paracetamol, returns to baseline | Consistent with mild primary headache (tension-type, mild migraine) | Weak - coincidental relief is possible in any cause |
| Headache responds to indomethacin specifically | Strongly suggests a subset of headaches called "indomethacin-responsive headaches" - paroxysmal hemicrania, hemicrania continua, primary cough headache | Moderate-strong - this is diagnostically meaningful |
| Headache does not respond to triptans | Less consistent with migraine; raises possibility of secondary cause or incorrect diagnosis | Moderate |
| Headache responds only to high-dose steroids | Suggests giant cell (temporal) arteritis | Moderate |
The Practical Conclusion
- If paracetamol relieves it: This does not rule out SAH, RCVS, or any vascular cause. It also does not confirm migraine.
- If paracetamol does not relieve it: This does not rule in a serious cause. Given the already-established allodynia (central sensitization), a partial or absent paracetamol response is actually the expected pattern in migraine at this stage of the attack.
The bottom line: Paracetamol response is diagnostically neutral. Never use it to reassure yourself or the patient that a headache is benign.
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Lippincott Illustrated Reviews: Pharmacology
- Harrison's Principles of Internal Medicine 22nd Ed.
The pain also increases on laughing.
Laughing as a Headache Trigger - What This Means
"Cough headache is a headache of sudden onset that is precipitated by a brief, nonsustained Valsalva maneuver such as coughing, laughing, sneezing, or bending over."
What This Symptom Pattern Means
| Symptom | Mechanism |
|---|---|
| Triggered by climbing stairs | Sustained physical exertion |
| Worsens with sudden head position change | ICP-sensitive or vascular instability |
| Worsens with touch/pressure on scalp | Central sensitization / allodynia |
| Worsens with laughing | Valsalva / transient ICP spike |
The Differential Is Now More Specific
1. Secondary Structural Causes - Now More Prominently Considered
"The proportion of patients who have an underlying structural cause has varied between 11% and 59% in studies done in the MRI era."
- The cerebellar tonsils herniate below the foramen magnum, obstructing CSF flow
- Headache is characteristically occipital/suboccipital, worsened or even initiated by Valsalva (laughing, coughing, straining)
- May also cause: visual phenomena, blurred vision, dizziness, tinnitus, pressure in the ears, nystagmus, dysphagia
- Frequently missed because mild forms can remain asymptomatic for years before manifesting
- Posterior fossa tumors or brain metastases
- Middle cranial fossa tumors
- Pituitary tumors
- Posterior fossa arachnoid cysts
- Basilar impression
- Third ventricular colloid cyst (classically causes positional headache with ball-valve obstruction - directly relevant given your positional worsening too)
- Spontaneous spinal CSF leak - can present purely as Valsalva-triggered headache without the classic orthostatic (lying-vs-standing) component in ~12% of cases
- Subdural hematoma
- RCVS (reversible cerebral vasoconstriction syndrome)
- Unruptured intracranial aneurysm
2. Primary Cough/Valsalva Headache (Benign)
- Older age of onset (~60 years mean)
- Bilateral, explosive, lasting seconds to minutes
- Free from pain between attacks
- Normal MRI with gadolinium
The Critical Investigation This Symptom Mandates
"All patients presenting with cough headache should get an MRI with gadolinium to look for pachymeningeal enhancement [from CSF leak] ... it would be reasonable to obtain an MRA of the intracranial circulation in most cases [to exclude aneurysm and RCVS]."
- Noncontrast CT head - urgently, to exclude hemorrhage (as before)
- MRI brain with gadolinium - to look for Chiari malformation, posterior fossa lesions, pachymeningeal enhancement (CSF leak), and other structural causes
- MRA of intracranial vessels - to exclude unruptured aneurysm and RCVS
- LP - if CT is normal but SAH suspicion remains
Updated Picture: Does This Change the Migraine Hypothesis?
- Exertional trigger
- Positional worsening
- Valsalva/laughing worsening
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology 12th Ed.
I am a 23-year-old female. How does that change things?
How Being a 23-Year-Old Female Changes Things
What Goes Up in Probability
1. Migraine - Now the Strong Leading Diagnosis
- Migraine often first appears or dramatically worsens after menarche
- Attacks frequently cluster around menstruation ("menstrual migraine")
- Pregnancy (sustained high estrogen) often improves migraine, while the postpartum estrogen crash worsens it
- Combined oral contraceptive pills, by adding exogenous estrogen cycles, can worsen or trigger migraine
2. Idiopathic Intracranial Hypertension (IIH) - Now a Prominent Differential
"IIH is seen primarily in young, obese women of childbearing age." "Women are affected more frequently than men (6 to 8:1 ratio). Onset is usually in young adulthood." "Incidence is 19-20 per 100,000 among obese women aged 15-55."
"The headache may be pulsatile... It may awaken the patient from sleep and is exacerbated by bending forward and the Valsalva maneuver, both of which impede cerebral venous return."
"The headache may be pulsatile and is frequently felt behind the eyes. Patients often report neck pain... Pulse-synchronous tinnitus is a frequent accompaniment, as are transient visual obscurations and diplopia."
| Your Symptom | IIH Explanation |
|---|---|
| Throbbing/pulsating headache | Elevated ICP transmitted as pulsatile pain |
| Worse with exertion (stairs) | Exertion raises ICP further |
| Worse with Valsalva (laughing) | Impedes cerebral venous return, spikes ICP |
| Worse with position change | ICP fluctuates with posture |
| Holocephalic (all aspects) | Diffuse pressure elevation |
| Cutaneous allodynia | Central sensitization from sustained elevated ICP |
- Do you ever notice a whooshing or pulsing sound in your ears (pulsatile tinnitus)? This is highly characteristic of IIH.
- Have you had any transient visual blackouts - momentary loss of vision lasting a second or two, especially on standing or straining? These are "transient visual obscurations" (TVOs) and are a warning sign of optic nerve compression from raised ICP.
- Headache (present ✓)
- Papilledema (needs fundoscopic exam)
- Elevated CSF opening pressure ≥250 mm H₂O
- Normal CSF composition
- Normal neuroimaging (excluding secondary causes)
3. Cerebral Venous Sinus Thrombosis (CVST) - Must Actively Exclude
- It presents with progressive headache (often the only symptom early on)
- Headache is typically worsened by Valsalva and exertion due to impaired venous drainage
- Can mimic IIH or migraine completely
- OCPs increase the risk of CVST approximately 5-7 fold; the combination of OCP use + a thrombophilia (e.g., Factor V Leiden, prothrombin mutation) increases it dramatically further
What Goes Down in Probability
| Diagnosis | Why Less Likely at 23 |
|---|---|
| Subarachnoid hemorrhage from aneurysm rupture | Still possible (aneurysms can rupture at any age) but much less common under 30; peak is 40s-60s |
| Temporal arteritis (giant cell arteritis) | Almost never occurs under 50; essentially excluded |
| Brain tumor (primary) | Lower incidence in young adults, though not zero |
| Cough headache (primary benign form) | Mean onset ~60 years; very uncommon at 23 |
| Atherosclerotic/hypertensive causes | Rare in 23-year-olds without specific risk factors |
Additional History Questions Now Critical for You
- Are you on the OCP or any hormonal contraception? - relevant for CVST risk and migraine pattern
- Do you experience these headaches in relation to your menstrual cycle? - menstrual migraine pattern
- Any whooshing/pulsing sound in your ears? - pulsatile tinnitus pointing to IIH
- Any momentary visual blackouts? - transient visual obscurations in IIH
- Any blurring of vision? - papilledema risk in IIH
- Recent weight gain? - obesity is the strongest risk factor for IIH; even modest weight gain in a young woman can trigger it
- Are you taking any medications? - tetracyclines (used for acne), minocycline, isotretinoin (Accutane), vitamin A supplements, fluoroquinolones, lithium, and growth hormone can all cause secondary IIH (pseudotumor cerebri)
- Importantly, isotretinoin (very commonly prescribed in young women for acne) is a well-documented cause of IIH
Updated Priority Differential at Age 23, Female
- Migraine - most common cause by far in this demographic; strong prior probability
- Idiopathic Intracranial Hypertension (IIH) - demographic bull's-eye; symptom pattern fits very well; must be excluded with fundoscopy, MRI/MRV, and LP opening pressure
- Cerebral Venous Sinus Thrombosis - especially if on OCP; requires MRV to exclude
- Primary exertional headache - benign but diagnosis of exclusion
- SAH / structural causes - still possible but lower probability than in older patients
- Rosen's Emergency Medicine
- Goldman-Cecil Medicine, International Edition
- Bradley and Daroff's Neurology in Clinical Practice
- Park's Textbook of Preventive and Social Medicine
CVST risk factors, presentation and diagnosis
"cerebral venous thrombosis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
"cerebral venous sinus thrombosis" diagnosis management
Cerebral Venous Sinus Thrombosis (CVST)
"CVT is an easily overlooked diagnosis that should always be considered in the presence of headache, seizures or encephalopathy."
Risk Factors
Prothrombotic / Systemic Risk Factors
Hormonal (highest relevance for a 23-year-old woman)
- Oral contraceptive pill (OCP) - single most common risk factor in young women; increases CVST risk ~5-7 fold; risk is higher with higher estrogen doses and combined pills
- Pregnancy - especially third trimester
- Peripartum/postpartum period - highest risk window is the first few weeks after delivery
- Hormone replacement therapy
Inherited Thrombophilias
- Factor V Leiden mutation
- Prothrombin G20210A mutation
- Protein C deficiency
- Protein S deficiency
- Antithrombin III deficiency
- These interact multiplicatively with OCP use - a woman on the OCP with an undiagnosed Factor V Leiden has dramatically elevated risk
Acquired Thrombophilias
- Antiphospholipid antibody syndrome (APAS) - particularly relevant in young women with autoimmune tendency
- Hyperhomocysteinemia
- Nephrotic syndrome
- Polycythemia vera, essential thrombocythemia
- Paroxysmal nocturnal hemoglobinuria (PNH)
Inflammatory / Systemic Disease
- Behcet's disease - a recognized cause, especially where vasculitis is present
- Systemic lupus erythematosus (SLE)
- Inflammatory bowel disease (Crohn's, ulcerative colitis)
- Sarcoidosis
Local / Regional Risk Factors
- Intracranial infection - meningitis, cerebral abscess, subdural empyema
- Ear/mastoid infection - otogenic CVST (lateral/sigmoid sinus thrombosis from otitis media or mastoiditis)
- Sinusitis - particularly sphenoid sinusitis spreading to cavernous sinus
- Head trauma - direct injury or dural laceration
- Neurosurgical procedures
- Lumbar puncture (rare - reduced CSF pressure can predispose)
- Dehydration - especially with concurrent risk factors
Other
- Malignancy (any cancer increases hypercoagulability)
- Hematological disorders (sickle cell, polycythemia)
- Vaccine-induced immune thrombocytopenia and thrombosis (VITT) - a recently recognized entity following adenoviral vector COVID-19 vaccines, characterized by high D-dimer and CVST
Clinical Presentation
The Most Common Symptom: Headache (~90% of cases)
- Usually progressive, developing over days to weeks
- Can be focal or diffuse (holocephalic)
- Frequently throbbing/pulsating (from raised ICP)
- Worsened by Valsalva, exertion, and position change - because all of these further impede venous return
- In some cases, onset is thunderclap (sudden severe)
- The headache of CVST is indistinguishable from migraine or raised ICP headache on clinical grounds alone - this is why imaging is mandatory
Syndrome by Sinus Involved
| Sinus Thrombosed | Predominant Presentation |
|---|---|
| Superior sagittal sinus (most common) | Raised ICP headache, bilateral leg weakness/seizures (parasagittal cortex), papilledema |
| Transverse/sigmoid sinus | Raised ICP headache, pulsatile tinnitus, can mimic IIH; otogenic infection is a precipitant |
| Cavernous sinus | Periorbital pain, proptosis, chemosis, ophthalmoplegia (III, IV, VI nerve palsy), ptosis - usually from facial/sinus infection |
| Deep venous system (internal cerebral veins, vein of Galen) | Bilateral thalamic involvement - altered consciousness, cognitive change, coma; most severe |
| Cortical vein thrombosis | Focal deficit, focal seizure corresponding to cortical territory |
Broader Symptom Spectrum
- Raised ICP features: headache (worst on waking, worsened by Valsalva), nausea/vomiting, papilledema, transient visual obscurations, sixth nerve palsy (false localizing sign)
- Focal neurological deficits: hemiparesis, hemisensory loss, aphasia (from venous infarction)
- Seizures: focal or generalized; occur in ~40% of cases; more common than in arterial stroke
- Encephalopathy: confusion, altered consciousness - suggests deep venous involvement or extensive infarction
- Pulsatile tinnitus: from transverse sinus involvement (also seen in IIH)
"CVT should be suspected in patients (particularly female patients under age 50) presenting with stroke symptoms without risk factors, unexplained new seizures or refractory headaches, or signs of intracranial hypertension."
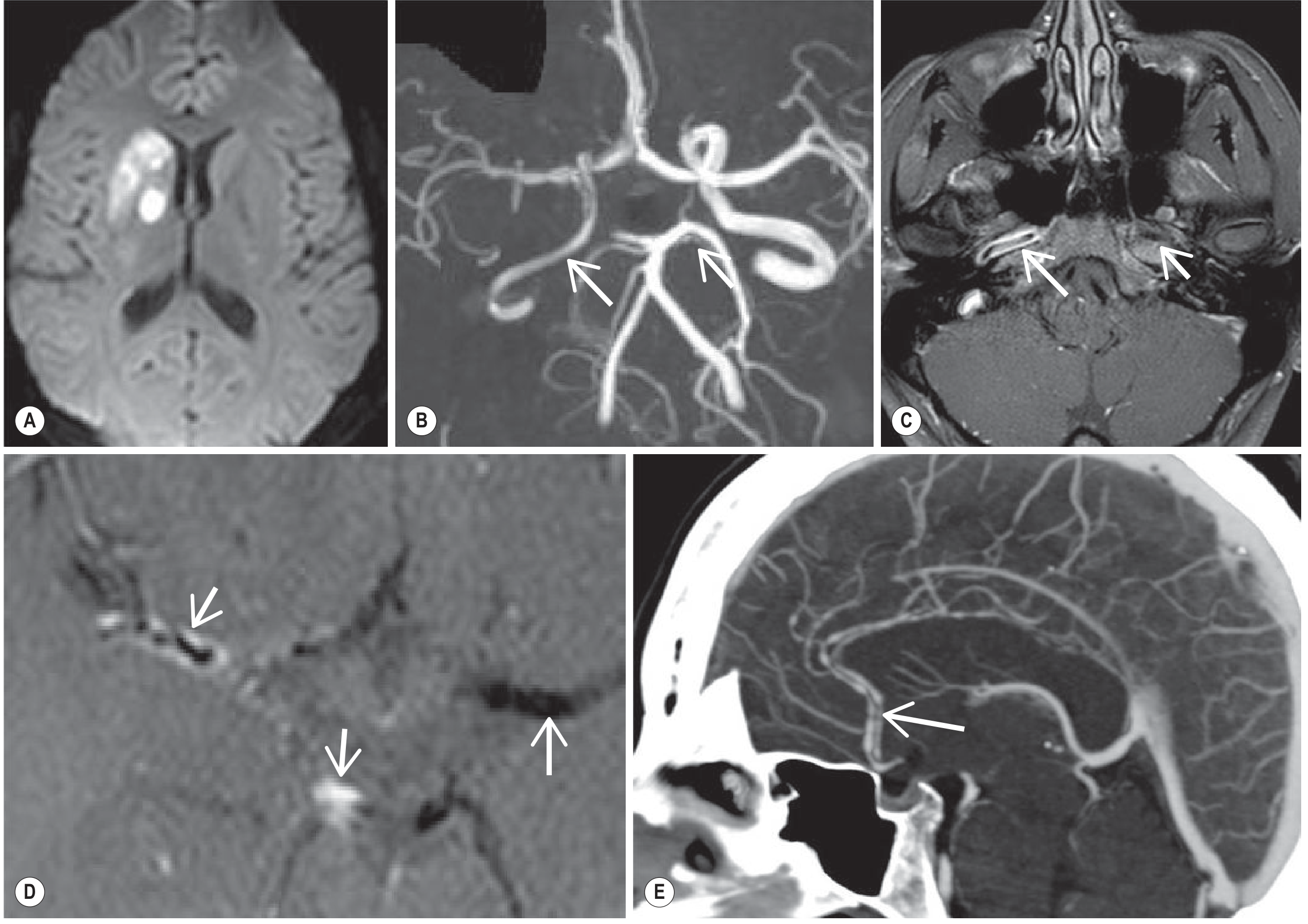
Diagnosis
Step 1: Non-Contrast CT Head
- Often the first investigation obtained in the ED
- May show the "dense triangle" or "dense cord" sign - hyperdensity of thrombosed sinus on plain CT (visible in ~30% of cases acutely)
- May show parenchymal oedema, haemorrhagic infarction (often bilateral or parasagittal - atypical for arterial stroke)
- Sensitivity is low (~30-50%) - a normal plain CT does NOT exclude CVST
Step 2: CT Venography (CTV) or MRI + MR Venography (MRV) - Definitive
"The combination of MRI and MRV is the gold standard for diagnosis of CVT, though contrast-enhanced CT with venous phase imaging is an alternative."
- "Empty delta sign" (or "empty triangle sign") on contrast CT: the thrombosed superior sagittal sinus appears as a triangular filling defect surrounded by a rim of enhancing dura - the clot is the dark centre, the enhanced dura forms the bright rim
- Loss of normal venous opacification on venous phase imaging
- Acute thrombus (0-5 days): intermediate T1, low T2 signal (deoxyhemoglobin) - can be mistaken for a flow void, making acute CVST easy to miss on T2 alone
- Subacute thrombus (5-15 days): bright on both T1 and T2 (methemoglobin) - most easily identified
- Chronic thrombus: variable, may recanalize
- Loss of normal flow void in the affected sinus
- SWI/GRE sequence: "blooming" hypointensity from thrombus, prominent dilated cortical veins (venous congestion)
- Loss of normal flow signal in the affected sinus
- Irregularity, severe narrowing, or complete occlusion
- Important caveat: a hypoplastic transverse sinus (normal variant) can mimic unilateral thrombosis - bilateral imaging and comparison are needed
Step 3: Ancillary Tests
| Test | Role |
|---|---|
| D-dimer | Elevated in most acute CVST; a normal D-dimer has moderate negative predictive value in low-to-intermediate pre-test probability, but is NOT reliable enough to exclude CVST alone |
| Lumbar puncture | If imaging is unavailable or equivocal; raised opening pressure common; CSF usually normal or mildly elevated protein - helps distinguish from SAH and meningitis |
| Thrombophilia screen | Factor V Leiden, prothrombin mutation, protein C/S, antithrombin, antiphospholipid antibodies, homocysteine - important for determining duration of anticoagulation after diagnosis |
| Full blood count | Polycythemia, thrombocytosis, thrombocytopenia (in VITT) |
| Fundoscopy | Papilledema if raised ICP |
Treatment (Brief)
"Primary treatment of CVT in the ED is anticoagulation with a weak recommendation for low molecular-weight heparin over unfractionated heparin."
Different types of migraine aura
Types of Migraine Aura
"Migraine auras occur in about one-third of migraine patients. Most patients who have attacks with aura also have attacks without aura, with only one-fifth of migraine-with-aura patients having aura with every attack."
ICHD-3 Criteria for Migraine With Aura
- Fully reversible
- Developing gradually over ≥5 minutes, or two or more symptoms occurring in succession
- Each symptom lasting no longer than 60 minutes
- Headache beginning during the aura or within 60 minutes after
The Six Recognized Aura Types
1. Visual Aura - Most Common (~80% of all auras)
- Scintillating scotoma - the most classic form: a flickering, shimmering arc or ring of light surrounding an area of visual loss. It typically starts as a small spot near the centre of vision, then expands outward as a crescent or horseshoe shape over 20-30 minutes
- Fortification spectra (teichopsia) - the border of the scotoma often has a characteristic zigzag, angular, battlements-like pattern resembling the walls of a medieval fortress, hence the name. This is highly specific to migraine
- Photopsia - simple flashes of light
- Wavy lines or "heat haze" distortions - shimmering visual distortions
- Scotoma - a blank or grey area in the visual field, usually following the positive phenomena as the depolarization wave passes
- Hemianopia (loss of half the visual field)
- Rarely: complete transient cortical blindness (usually in brainstem aura - see below)
"Initially a binocular negative scotoma is commonly present, but may go unrecognized or be perceived as a vague visual disturbance. Associated positive phenomena develop after a few minutes and may consist of scintillating scotomas (zig-zags or fortification spectra), 'heat haze' distortions... progressing slowly across the field over several minutes. Full visual recovery within 30 minutes is typical."
2. Sensory Aura - Second Most Common
"Sensory aura is characterized by positive symptoms (paraesthesias) followed by negative symptoms (numbness). The slowly spreading quality of aura symptoms is very helpful in establishing the migraine aura diagnosis."
- Often begins in the hand or fingertips, then spreads up the arm to the face/lips (the "cheiro-oral" distribution is classic - fingers to perioral area)
- Or may begin in the face
- The march takes 10-20 minutes, reflecting CSD spreading across the somatosensory cortex
- Followed by numbness in the same distribution
3. Speech/Language Aura (Dysphasic Aura)
- Dysphasia - difficulty finding words, garbled speech, paraphasic errors
- Aphasia - more complete language disruption
- Often accompanies sensory or visual aura rather than occurring in isolation
- Usually lasts less than 30 minutes and resolves completely
4. Motor Aura (Hemiplegic Migraine) - Most Severe
"Motor symptoms often start in the hand and gradually spread to other areas, over 20-30 minutes, although it may occur suddenly mimicking a stroke. The duration of symptoms can be variable, from a few hours to weeks."
- FHM1 (50-75% of families): CACNA1A mutation (chromosome 19p13), encoding P/Q-type calcium channel α1 subunit. Associated with cerebellar degeneration and overlap with episodic ataxia type 2. Severe attacks can cause fever, meningismus, confusion, or coma
- FHM2 (<25%): ATP1A2 mutation (chromosome 1q23), encoding Na⁺/K⁺-ATPase. No cerebellar signs
- FHM3 (rare): SCN1A mutation (chromosome 2q24), encoding neuronal voltage-gated sodium channel
- FHM4: Clinically typical FHM with no known mutation identified
5. Brainstem Aura (Migraine with Brainstem Aura; formerly Basilar Migraine)
"These patients first develop visual phenomena like those of typical migraine except that they occupy much or the whole of both visual fields (temporary cortical blindness may occur). There may be associated vertigo, staggering, incoordination of the limbs, dysarthria, and tingling in both hands and feet, and sometimes around both sides of the mouth... At the stage when headache would begin, patients may faint, and others become confused or stuporous. Exceptionally, there is an alarming period of coma or quadriplegia."
- Dysarthria
- Vertigo
- Tinnitus
- Hypacusia (hearing difficulty)
- Diplopia
- Ataxia (not attributable to sensory deficit)
- Decreased level of consciousness
- No motor weakness (if present, it's hemiplegic migraine instead)
6. Retinal Migraine
"Retinal migraine manifests with visual disturbance that may be similar to classical migraine but affects only one eye. It is a controversial entity, some authorities believing that most cases should be regarded as presumed recurrent ocular vasospasm rather than true migraine. Young women are most commonly affected... It may be prudent to investigate as for retinal embolization and peripheral vasospasm."
Special Category: Aura Without Headache (Acephalgic Migraine)
- More common in older migraineurs (especially men over 50)
- The aura appears in isolation, without the expected headache
- Particularly challenging to diagnose because it closely mimics TIA - especially sensory or visual auras without headache
- The gradual march, positive phenomena (e.g., scintillating scotoma), and prior history of migraine with headache are the main differentiating clues
Summary Table
| Aura Type | Cortical Origin | Key Features | Reversible? |
|---|---|---|---|
| Visual | Occipital cortex | Scintillating scotoma, fortification spectra, photopsia, hemianopia - binocular | Yes, fully |
| Sensory | Somatosensory cortex | Unilateral paraesthesias - cheiro-oral march | Yes, fully |
| Speech/Dysphasia | Dominant temporal/frontal | Word-finding difficulty, garbled speech | Yes, fully |
| Motor (Hemiplegic) | Motor cortex | Hemiparesis to hemiplegia; genetic subtypes; can last days-weeks | Usually yes; occasionally residual deficits in FHM1 |
| Brainstem | Brainstem/bilateral occipital | Vertigo, diplopia, dysarthria, ataxia, altered consciousness; no motor weakness | Yes, but first attack needs imaging |
| Retinal | Retina/optic nerve | Strictly monocular visual loss; controversial; diagnosis of exclusion | Usually yes; risk of infarction |
| Aura without headache | Any of above | Any aura type without subsequent headache; mimics TIA | Yes |
The Cortical Spreading Depression Unifier
- Occipital lobe → visual aura
- Parietal somatosensory cortex → sensory aura
- Dominant temporal/frontal → dysphasia
- Motor cortex → hemiplegic aura
- Brainstem → brainstem aura