Detailed life cycle of trypanosoma cruzi with stage
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Here is the detailed life cycle of Trypanosoma cruzi:
Life Cycle of Trypanosoma cruzi (Chagas Disease)
T. cruzi is a hemoflagellate protozoan with a complex, two-host life cycle involving three distinct morphological stages. The parasite alternates between a triatomine (reduviid/kissing) bug and a mammalian host (including humans). The key vectors belong to the genera Rhodnius, Triatoma, and Panstrongylus.
The Three Developmental Stages
| Stage | Host | Key Features |
|---|---|---|
| Trypomastigote | Mammalian bloodstream / Bug feces | Motile, elongated, flagellum present, C-shaped with large kinetoplast |
| Amastigote | Mammalian intracellular tissues | Non-motile, no flagellum, oval, 1-3 µm, multiplies by binary fission |
| Epimastigote | Triatomine bug midgut | Motile, replicating form in the insect |
Life Cycle Diagram (CDC DPDx)
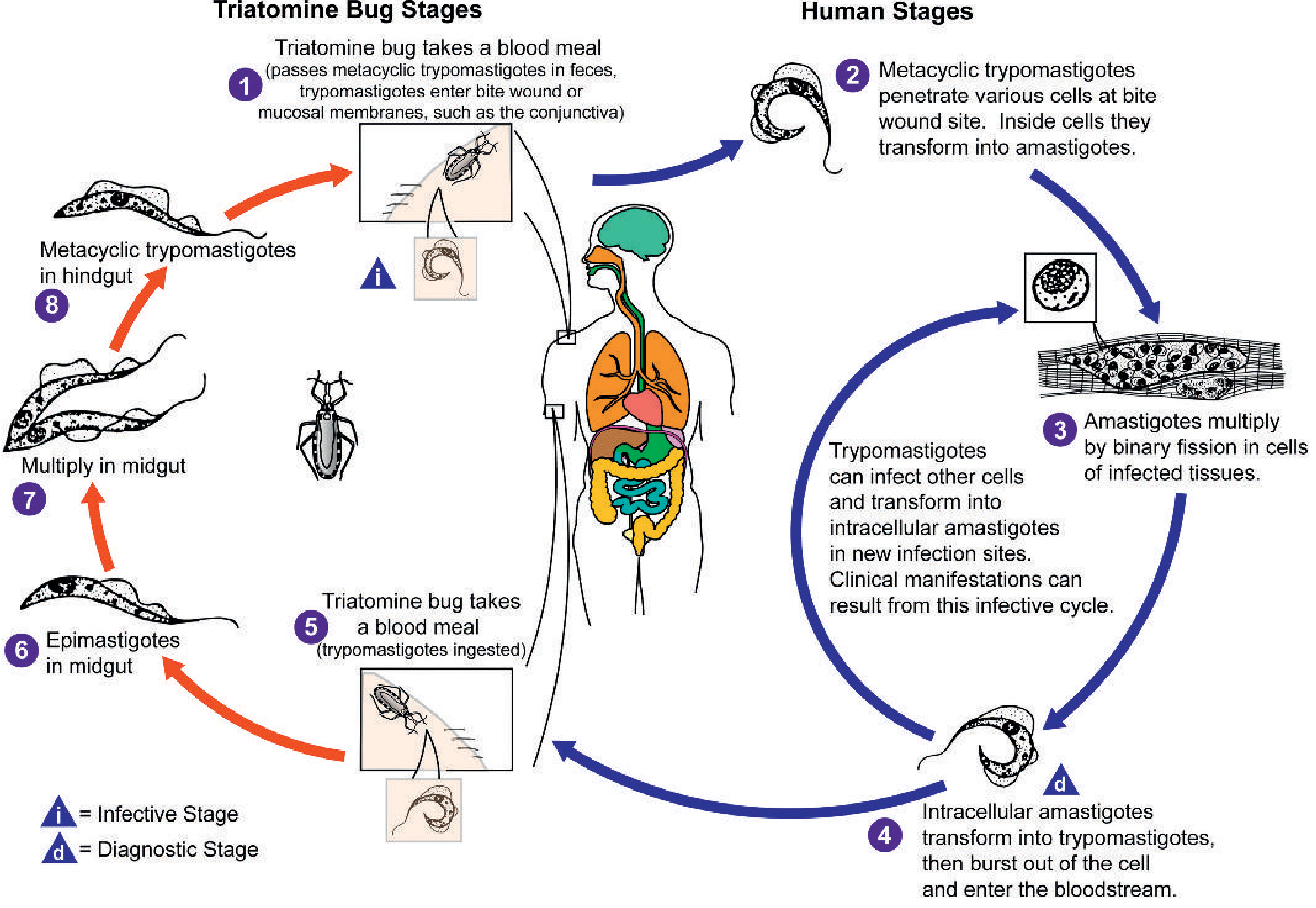
Fig. 88.26 - Life cycle of Trypanosoma cruzi. Tietz Textbook of Laboratory Medicine, 7th Edition
Detailed Step-by-Step Life Cycle
IN THE TRIATOMINE BUG (Vector Stages)
Step 1 - Blood meal & fecal transmission (Infective Stage - "i")
The triatomine bug feeds on a mammalian host (human, dog, rodent, or other reservoir animal) at night. While feeding, the infected bug defecates near the bite wound, depositing feces containing metacyclic trypomastigotes - the infective stage. This is the defining feature that distinguishes T. cruzi from African trypanosomes: the infective form is passed in feces, NOT in saliva. The patient's scratching then inoculates these forms into the wound or nearby mucosal membranes (e.g., conjunctiva).
IN THE HUMAN/MAMMALIAN HOST
Step 2 - Penetration & invasion of host cells
Metacyclic trypomastigotes penetrate cells at the bite wound site (skin, mucosa, conjunctiva). They invade local host cells actively, including macrophages, cardiomyocytes, smooth muscle cells, and neuronal cells. Multiple cell types can be invaded, not just phagocytes.
Step 3 - Transformation to amastigotes (intracellular stage)
Inside the host cell, trypomastigotes lose their flagellum and undulating membrane and transform into amastigotes - small (1-3 µm), oval, non-motile forms. These reside within the host cell cytoplasm (not in a parasitophorous vacuole - the parasite escapes into the cytosol).
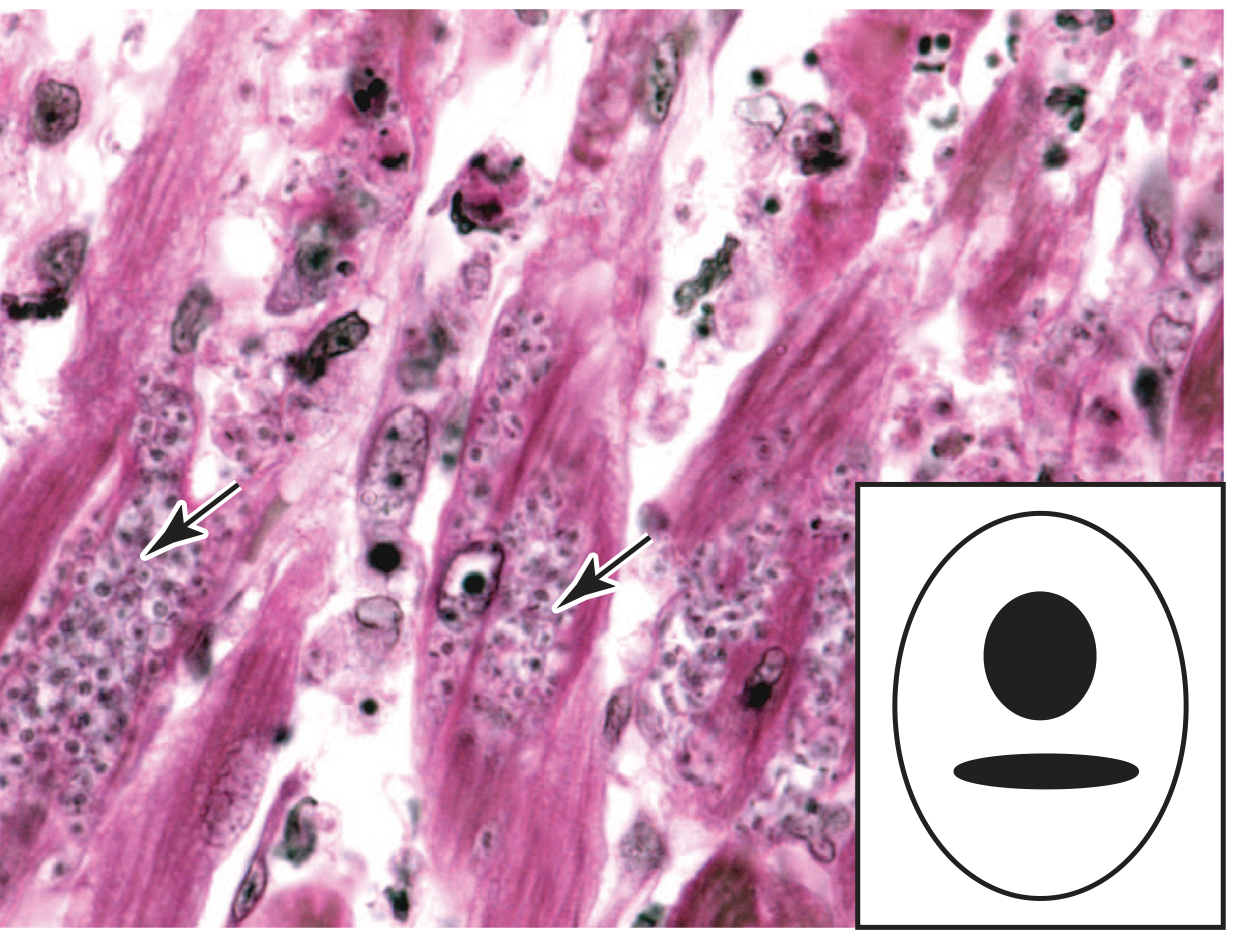
Fig. 46-5 - Amastigote colonies in heart muscle, Jawetz Melnick & Adelberg's Medical Microbiology 28E
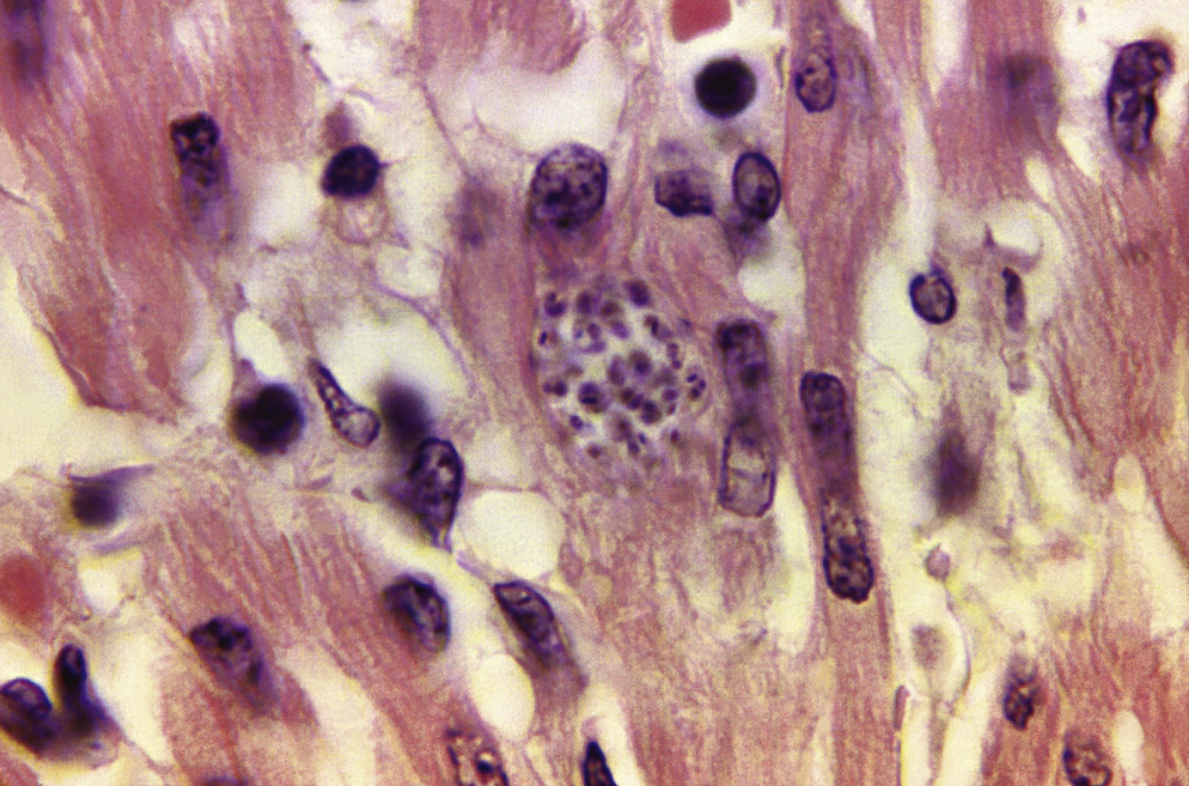
Fig. 73.15 - Amastigotes in cardiac tissue, Medical Microbiology 9e
Step 4 - Binary fission and pseudocyst formation
Amastigotes multiply by binary fission, filling the host cell with a large intracellular colony called a pseudocyst (not a true cyst - it has no distinct wall). Target organs include:
- Heart muscle (most important - leads to chagasic cardiomyopathy)
- Liver
- Brain
- Smooth muscle of GI tract (leads to megaesophagus, megacolon)
- Skeletal muscle
Step 5 - Transformation back to trypomastigotes & cell rupture (Diagnostic Stage - "d")
Intracellular amastigotes periodically differentiate back into bloodstream trypomastigotes. These burst out of the host cell, enter the bloodstream, and circulate as trypomastigotes (Diagnostic Stage - detectable on peripheral blood smear). Crucially, bloodstream trypomastigotes do NOT multiply in the blood - they are non-dividing in this stage. They can infect new host cells and repeat the amastigote cycle in other tissues, or be ingested by a feeding triatomine bug.
BACK IN THE TRIATOMINE BUG
Step 6 - Bug ingests trypomastigotes during another blood meal
When an uninfected triatomine bug bites an infected mammal, it ingests circulating trypomastigotes in the blood meal.
Step 7 - Transformation to epimastigotes in midgut
Ingested trypomastigotes travel to the midgut of the bug, where they transform into epimastigotes - the replicating form in the insect. Epimastigotes multiply by longitudinal binary fission in the midgut.
Step 8 - Migration to hindgut & metacyclic trypomastigotes
Epimastigotes migrate posteriorly to the hindgut/rectum of the bug, where they differentiate into metacyclic trypomastigotes - the infective, non-dividing form ready to be deposited in feces during the next blood meal, completing the cycle.
Summary Flowchart
TRIATOMINE BUG HUMAN HOST
─────────────────────────────────────────────────────
Metacyclic trypomastigotes (hindgut)
│
▼ (deposited in feces during bite)
Metacyclic trypomastigotes
penetrate wound/mucosa
│
▼
Invade host cells
│
▼
Amastigotes (intracellular)
multiply by binary fission
│
▼
Differentiate → Trypomastigotes
burst out → bloodstream
│
├── infect new host cells (repeat)
│
▼
Bug ingests trypomastigotes during blood meal
│
▼
Epimastigotes (midgut) - multiply by binary fission
│
▼
Metacyclic trypomastigotes (hindgut) ← CYCLE REPEATS
Key Points to Remember
| Feature | Detail |
|---|---|
| Infective stage for humans | Metacyclic trypomastigote (in bug feces) |
| Diagnostic stage | Bloodstream trypomastigote (peripheral blood smear, acute phase) |
| Intracellular stage | Amastigote (most tissue damage occurs here) |
| Replicating stage in bug | Epimastigote (midgut) |
| Unique kinetoplast | Large, rounded, terminal - distinguishing T. cruzi |
| Does NOT multiply in blood | Trypomastigotes are non-dividing in bloodstream |
| Mode of transmission | Fecal-oral inoculation (NOT salivary injection) |
Alternative Routes of Transmission
Beyond vector-borne transmission, T. cruzi can also be transmitted via:
- Blood transfusion from infected donors
- Organ transplantation
- Congenital/transplacental (mother to fetus)
- Oral ingestion of food/beverages contaminated with infected bug feces (documented in Brazil with fruit juices)
- Laboratory accidents
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed.; Medical Microbiology 9e; Jawetz, Melnick & Adelberg's Medical Microbiology, 28e
blood culture method for t.cruzi
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Searching the Web
Trypanosoma cruzi blood culture method hemoculture NNN medium procedure sensitivity
Reading Web Page
https://www.cdc.gov/dpdx/trypanosomiasisamerican/index.html
Finding Sources
Reading File
Finding Sources
I have sufficient information from textbooks, CDC, and clinical sources. Here is a comprehensive answer:
Blood Culture Methods for Trypanosoma cruzi
Culture (hemoculture) of T. cruzi is a parasitological (direct) method - one of several techniques used to confirm infection by directly detecting the parasite. It is most useful in the acute phase, when parasitemia is high, but is also employed when other methods fail.
Overview of Direct Diagnostic Methods
| Method | Best Phase | Sensitivity | Turnaround |
|---|---|---|---|
| Fresh blood film / Thick & thin smear | Acute | 40-90% (concentrated) | Hours |
| Buffy coat concentration | Acute | Moderate-high | Hours |
| Hemoculture (blood culture) | Acute > Chronic | Low-moderate | Weeks |
| Xenodiagnosis | Chronic | <50% | 30-60 days |
| Animal inoculation | Any | High (research) | Weeks |
| PCR | Acute & Chronic | 82-100% | Days |
Hemoculture (Blood Culture) - Detailed Method
Principle
Patient blood is inoculated into a biphasic or liquid culture medium that supports growth of T. cruzi. The bloodstream trypomastigotes (which do not divide in blood) transform into epimastigotes in the culture medium and multiply by binary fission. Cultures are then examined microscopically for motile epimastigotes.
Media Used
1. NNN Medium (Novy-MacNeal-Nicolle)
- The classical biphasic medium, originally designed for Leishmania but also used for T. cruzi
- Solid phase: Blood agar base (defibrinated rabbit blood + nutrient agar)
- Liquid phase: Locke's solution (saline + dextrose) overlaid on the solid phase
- Organisms multiply in the liquid (condensation water) phase as epimastigotes
2. Liver Infusion Tryptose (LIT) Broth
- A liquid medium; more commonly used for T. cruzi than NNN
- Contains: liver infusion broth + tryptose + hemin + fetal bovine serum (FBS) + antibiotics (penicillin, streptomycin to suppress bacterial contamination)
- Widely used in Latin American reference laboratories
3. Brain Heart Infusion (BHI) Broth
- Used as an alternative liquid medium
- Supplemented with fetal calf serum
4. RPMI-1640 or Schneider's Drosophila Medium
- Used in specialized/research settings, especially for axenic cultures
- Supplemented with serum and hemin
Procedure
Step 1 - Blood collection
- Draw 5-10 mL of venous blood in a heparinized or EDTA tube (anticoagulated)
- Heparin is preferred as EDTA may be less suitable for culture initiation
- Process promptly - the sample should ideally be inoculated within a few hours
Step 2 - Inoculation
- Inoculate 1-2 mL of blood into culture medium (LIT broth or biphasic NNN tubes)
- Some protocols concentrate trypomastigotes first via buffy coat preparation before inoculation to increase sensitivity:
- Centrifuge blood at 800-1000 rpm for 5-10 minutes
- Aspirate the buffy coat layer
- Inoculate the buffy coat into culture medium
Step 3 - Incubation
- Incubate at 26-28°C (this mimics the triatomine bug midgut temperature, which favors epimastigote growth)
- NOT at 37°C (human body temperature would maintain trypomastigotes but suppress epimastigote multiplication)
- Tubes are kept in a slanted/horizontal position initially
Step 4 - Examination
- Examine cultures weekly by withdrawing a small aliquot (0.1-0.2 mL)
- Prepare a wet mount and examine under low-power microscopy for motile epimastigotes
- Alternatively, make Giemsa-stained smears of the aliquot
- Continue examining for a minimum of 4-8 weeks before declaring negative
- Some protocols examine at: Day 7, 14, 21, 28, and 60 days
Step 5 - Identification
- Epimastigotes are recognized by their characteristic morphology:
- Kinetoplast located anterior to the nucleus (unlike trypomastigotes where kinetoplast is posterior/terminal)
- Elongated body with flagellum
- Motile
What Grows in Culture
When T. cruzi blood is cultured at 26-28°C, the trypomastigotes transform into epimastigotes - the same replicating form found in the triatomine bug midgut. The epimastigotes multiply and are what you detect on microscopy.

(CDC DPDx: epimastigotes from culture - kinetoplast is anterior to the nucleus)
Sensitivity & Limitations
| Factor | Detail |
|---|---|
| Acute phase sensitivity | Best - trypomastigotes numerous in blood |
| Chronic phase sensitivity | Very low - parasitemia is minimal or intermittent |
| Time to result | 2-8 weeks (prolonged turnaround) |
| Chronic Chagas culture | Only ~50% or less sensitivity |
| Advantage over smear | More sensitive when parasitemia is low |
| Risk | Biohazardous - requires BSL-2 precautions; lab-acquired infections via needlestick are documented |
Comparison With Other Direct Methods
Buffy Coat Concentration (Strout Method / Microhematocrit)
- Blood is centrifuged; buffy coat layer is examined for motile trypomastigotes
- Quick, sensitive in high parasitemia (acute phase)
- Microhematocrit centrifugation (QBC tube): spins in capillary tubes, examine interface microscopically
Xenodiagnosis
- Laboratory-reared, T. cruzi-free triatomine bugs are allowed to feed on the patient
- Bug feces/intestinal contents examined at 30-60 days for epimastigotes/trypomastigotes
- Sensitivity: <50% in chronic infection (per Sleisenger & Fordtran)
- Historically important in endemic areas; now largely replaced by PCR
Animal Inoculation
- Patient blood is inoculated into mice or guinea pigs
- Blood smears from the animal are examined at 7-30 days for trypomastigotes
- High sensitivity but strictly confined to research/reference labs
- Not practical for routine clinical use
When to Use Culture in Clinical Practice
| Clinical Situation | Recommended Test |
|---|---|
| Acute Chagas, early (days 10-30) | Thick/thin blood smear (trypomastigotes abundant) |
| Acute Chagas, smear negative | PCR > hemoculture |
| Chronic Chagas | Serology (2 tests by different methods) |
| Chronic Chagas, immunosuppressed | PCR + serology |
| Congenital Chagas (newborn) | Microhematocrit concentration + PCR |
| Blood/organ donor screening | EIA-based serology (FDA-approved) |
Key Points Summary
- Culture of T. cruzi is called hemoculture and uses LIT broth or NNN biphasic medium
- Blood is incubated at 26-28°C (not 37°C) to promote epimastigote growth
- Results read weekly for 4-8 weeks; presence of motile epimastigotes = positive
- Sensitivity is higher in acute phase and substantially lower in chronic infection
- In practice, PCR has largely replaced culture because it is faster, more sensitive (especially in chronic disease), and does not require live parasite growth
- The kDNA minicircle PCR for T. cruzi achieves up to 100% sensitivity compared with culture/serology/xenodiagnosis as reference standard (Medical Microbiology 9e)
Sources: Medical Microbiology 9e; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Henry's Clinical Diagnosis and Management by Laboratory Methods; CDC DPDx - American Trypanosomiasis; Public Health Ontario - T. cruzi Lab Methods
detailed life cycle of trponosoma brucei with stages
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
I now have all the diagrams, microscopy images, and comprehensive textbook content needed. Here is the full detailed answer:
Life Cycle of Trypanosoma brucei (Human African Trypanosomiasis / Sleeping Sickness)
T. brucei causes Human African Trypanosomiasis (HAT), also called sleeping sickness. Two subspecies cause human disease:
- T. b. gambiense - West/Central Africa; chronic disease (97% of cases)
- T. b. rhodesiense - East/Southeast Africa; acute, rapidly fatal disease (3% of cases)
The vector is the tsetse fly (Glossina species). Unlike T. cruzi, T. brucei has NO intracellular amastigote stage - it lives entirely extracellularly in blood, lymph, and CSF throughout the mammalian host.
Life Cycle Diagram
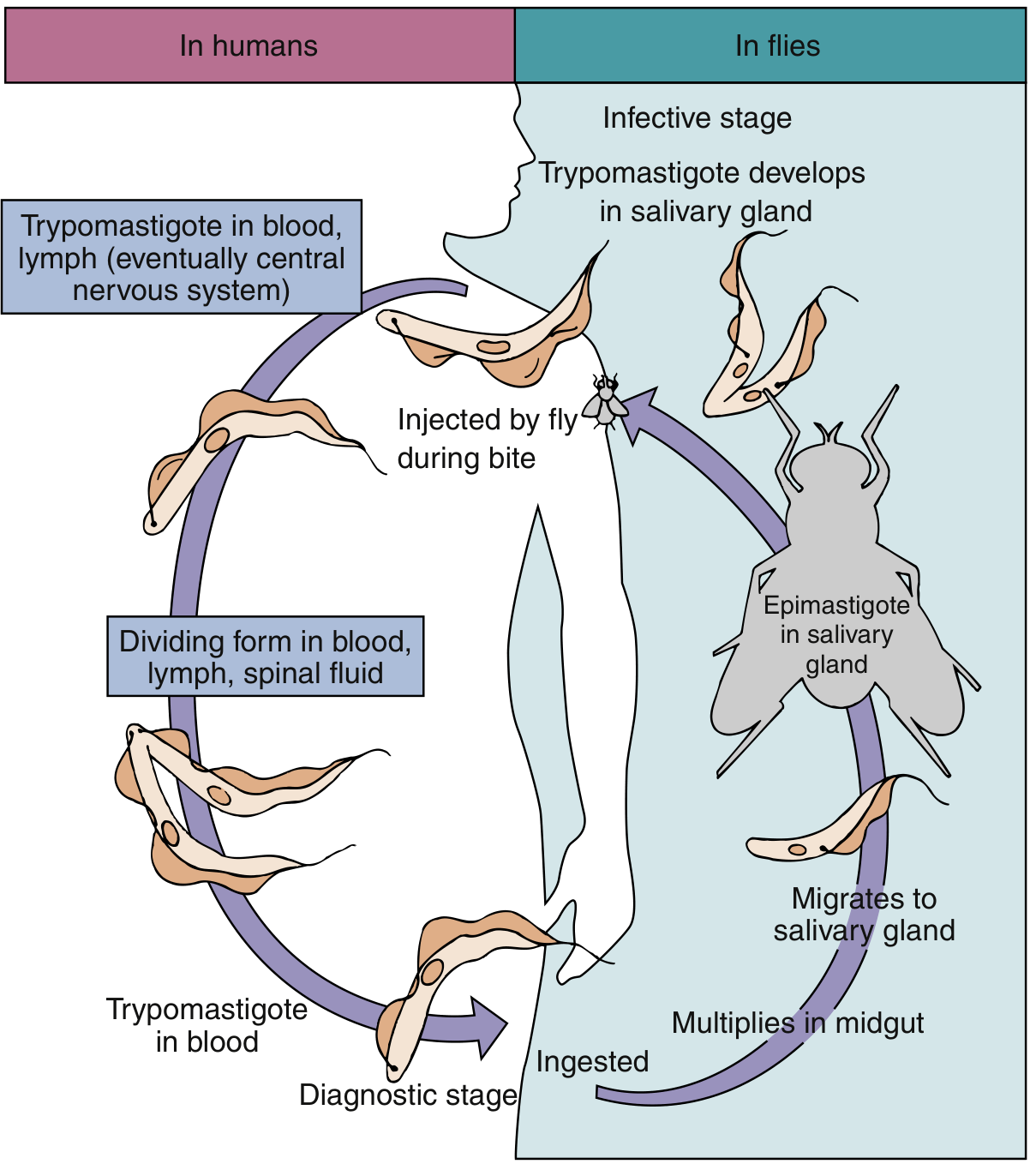
Fig. 73.12 - Life cycle of Trypanosoma brucei. Medical Microbiology 9e
The Three Key Morphological Stages
| Stage | Location | Features | Replication |
|---|---|---|---|
| Metacyclic trypomastigote | Tsetse salivary gland | Infective, non-dividing | No |
| Bloodstream trypomastigote | Human blood, lymph, CSF | Extracellular, motile, divides | Yes - binary fission |
| Epimastigote | Tsetse midgut & salivary gland | Kinetoplast anterior to nucleus | Yes - binary fission |
Key distinction from T. cruzi: T. brucei has NO amastigote stage and NO intracellular phase. The trypomastigote divides freely in blood and body fluids. In T. cruzi, bloodstream trypomastigotes do NOT divide - only amastigotes inside cells divide.
Detailed Step-by-Step Life Cycle
PART 1: IN THE TSETSE FLY (Vector Stages)
Step 1 - Tsetse fly takes a blood meal from infected host (Ingestion)
An uninfected Glossina species fly bites a mammalian host with circulating T. brucei trypomastigotes in the blood. The bloodstream trypomastigotes are ingested with the blood meal into the fly's midgut.
Step 2 - Transformation to procyclic trypomastigotes in the midgut
In the fly's midgut, the bloodstream trypomastigotes undergo a transformation - they differentiate into procyclic trypomastigotes (also called midgut trypomastigotes). These are morphologically similar to bloodstream forms but are adapted to the insect environment. They lose their variant surface glycoprotein (VSG) coat and express procyclins instead.
Step 3 - Multiplication in the midgut
Procyclic trypomastigotes multiply rapidly by binary fission in the fly's midgut over approximately 1-3 weeks. This is one of the key active replication phases in the fly.
Step 4 - Migration to the salivary glands
After multiplication in the midgut, the trypomastigotes migrate anteriorly through the fly's body - through the proventriculus (foregut) and then into the salivary glands via the salivary ducts.
Step 5 - Transformation to epimastigotes in the salivary glands
In the salivary glands, the organisms transform into epimastigotes - a distinct morphological form characterized by:
- Kinetoplast located anterior to the nucleus (vs. posterior in trypomastigotes)
- Free flagellum present
- Only a partial undulating membrane (shorter than in trypomastigotes)
- Continue to multiply by binary fission in the salivary glands
Step 6 - Final transformation to metacyclic trypomastigotes (Infective Stage)
Epimastigotes in the salivary glands undergo a final differentiation into metacyclic trypomastigotes - the infective stage for mammals. These:
- Re-acquire a VSG coat (variant surface glycoprotein)
- Are non-dividing but fully infective
- Are present in the fly's saliva ready for injection during the next blood meal
- This entire process in the fly takes approximately 4-6 weeks (the "extrinsic incubation period")
The fly remains infected for life after this transformation. Both male and female flies can transmit the disease.
PART 2: IN THE HUMAN/MAMMALIAN HOST
Step 7 - Tsetse fly bites; metacyclic trypomastigotes injected into skin (Infective Stage)
When an infected tsetse fly takes a blood meal, it injects metacyclic trypomastigotes from its saliva directly into the skin at the bite site. This is salivary (anterior station) transmission - fundamentally different from T. cruzi which is transmitted via feces (posterior station).
Step 8 - Primary lesion (Trypanosomal Chancre)
At the site of the bite, the injected trypomastigotes multiply locally and cause an area of induration and swelling - the trypanosomal chancre (also called the primary lesion). This local reaction is more prominent in T. b. rhodesiense infection.
Step 9 - Transformation to bloodstream trypomastigotes & entry into blood and lymphatics
The metacyclic trypomastigotes transform into bloodstream trypomastigotes and enter the circulatory system and lymphatics. These forms:
- Measure 14-35 µm in length
- Have a small, posteriorly located kinetoplast
- Have a centrally located nucleus
- Bear a full undulating membrane running the length of the body with a free anterior flagellum
- Are extracellular throughout their life in the mammalian host
Step 10 - Multiplication in blood and lymph (Hemolymphatic stage = Stage 1 of disease)
Bloodstream trypomastigotes actively multiply by binary fission in the blood, lymph, and lymph nodes. This is the first (hemolymphatic) stage of HAT. Key features:
- Waves of parasitemia occur, each suppressed by the immune response but replaced by a new antigenic variant
- This is driven by Antigenic Variation via Variant Surface Glycoproteins (VSGs)
- Each T. brucei genome encodes ~1000 VSG genes
- Only one VSG coat is expressed at a time; periodic switching allows immune evasion
- Posterior cervical lymphadenopathy (Winterbottom's sign) is characteristic of T. b. gambiense
Step 11 - CNS invasion (Meningoencephalitic stage = Stage 2 of disease)
Eventually, bloodstream trypomastigotes cross the blood-brain barrier and invade the central nervous system (CSF and brain parenchyma). They continue to divide in the CSF. CNS invasion leads to the classic sleeping sickness syndrome:
- T. b. rhodesiense: CNS invasion within ~1 month
- T. b. gambiense: CNS invasion after several months to years
- Symptoms: progressive somnolence, personality changes, tremors, meningoencephalitis, coma, death
Step 12 - Tsetse fly ingests trypomastigotes during another blood meal → cycle repeats
When a new tsetse fly bites the infected mammal, it ingests bloodstream trypomastigotes in the blood meal, and the cycle in the fly (Steps 1-6) begins again.
Complete Life Cycle Summary Diagram
TSETSE FLY HUMAN HOST
─────────────────────────────────────────────────────────────────
Metacyclic trypomastigotes (salivary gland)
│ [INFECTIVE STAGE]
│
▼ injected in saliva during bite
Metacyclic trypomastigotes
→ Local chancre at bite site
│
▼
Bloodstream trypomastigotes
→ Blood + lymph [STAGE 1: hemolymphatic]
→ Multiply by binary fission
→ Antigenic variation (VSG switching)
│
▼
Cross blood-brain barrier
→ CSF + brain [STAGE 2: meningoencephalitic]
→ Continue dividing
│
▼ [DIAGNOSTIC STAGE]
Tsetse fly ingests trypomastigotes during blood meal
│
▼
Procyclic trypomastigotes (midgut) - multiply
│
▼
Epimastigotes (salivary gland) - multiply
│
▼
Metacyclic trypomastigotes (salivary gland) ← CYCLE REPEATS
Microscopy Images
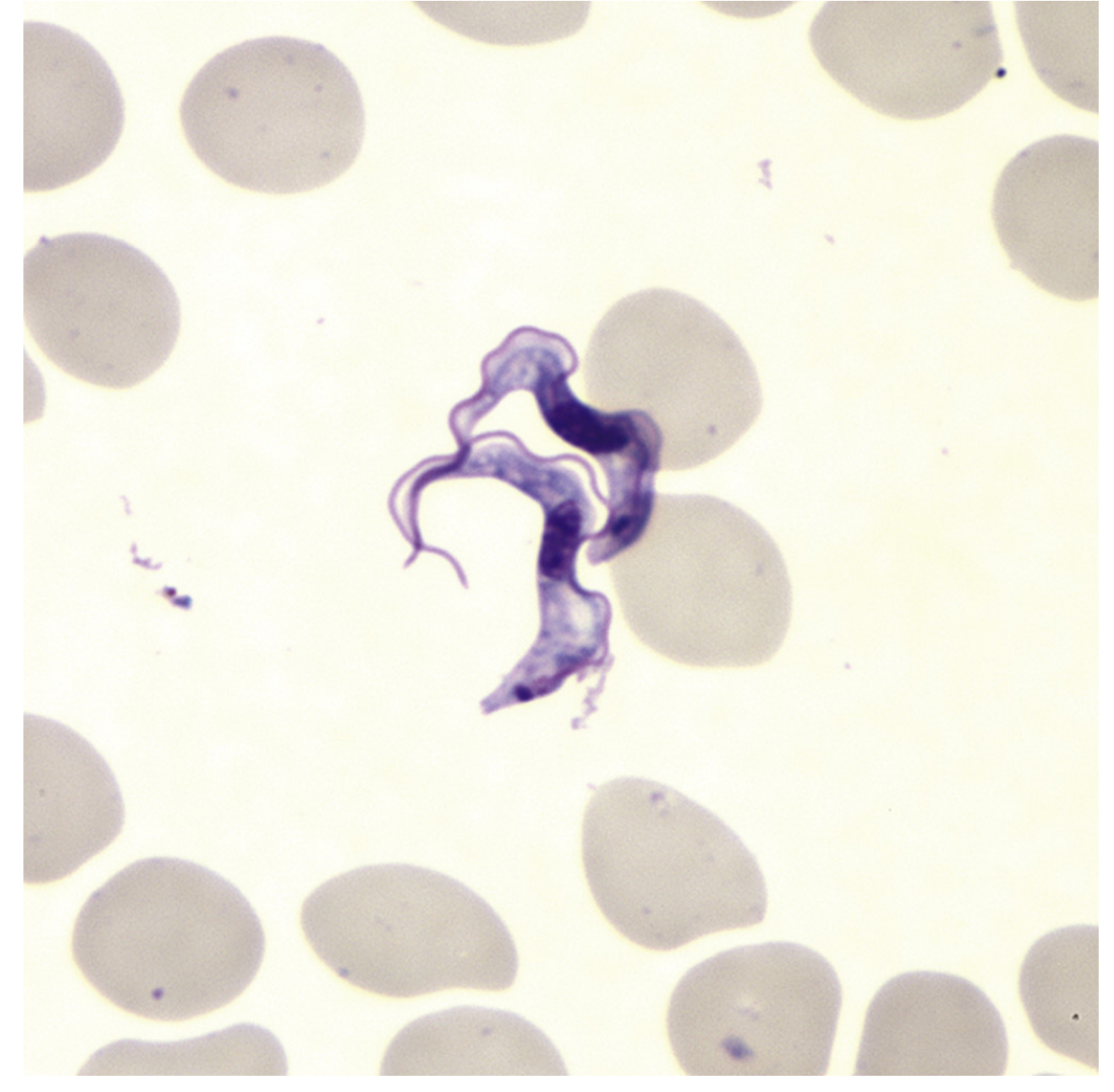
Fig. 73.13 - Trypomastigote stage of T. brucei gambiense in blood smear (CDC Public Health Image Library)
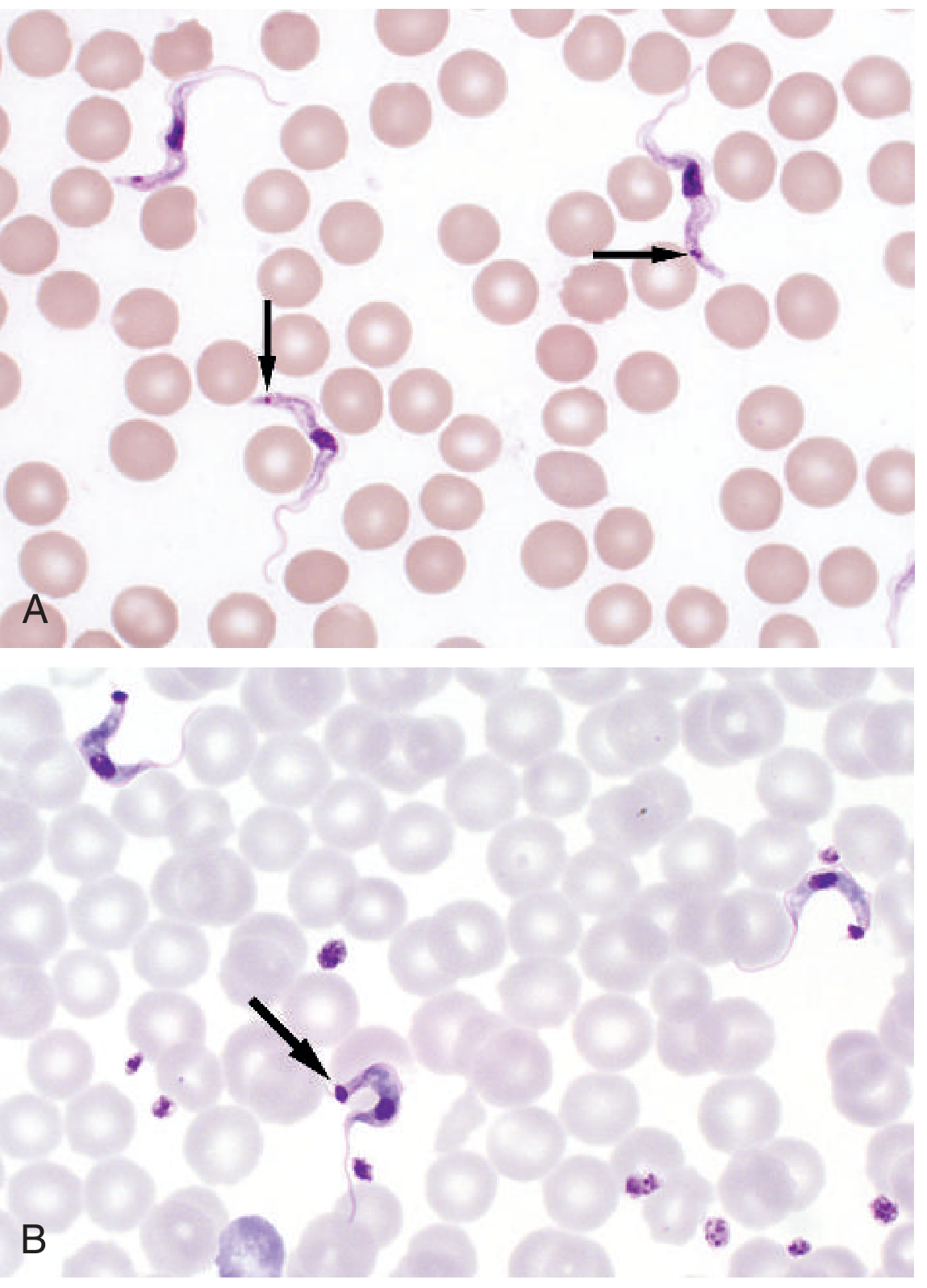
Fig. 88.25 - T. brucei (A) vs T. cruzi (B) in blood smear. Key distinction: kinetoplast is small in T. brucei, large in T. cruzi. Tietz Textbook of Laboratory Medicine, 7th Ed.
Comparison: T. b. gambiense vs T. b. rhodesiense
| Feature | T. b. gambiense | T. b. rhodesiense |
|---|---|---|
| Geographic distribution | West & Central Africa (24 countries) | East & Southeast Africa (13 countries) |
| % of HAT cases | >97% | ~3% |
| Disease course | Chronic, months-years | Acute, rapidly fatal (9-12 months) |
| CNS invasion timing | Months to years | ~1 month |
| Winterbottom's sign | Prominent | Less prominent |
| Reservoir | Humans primarily | Cattle, sheep, wild game (zoonosis) |
| Tsetse vector | G. palpalis (streamside) | G. morsitans (savanna brush) |
| Nagana (animal disease) | N/A | Related subspecies (T. b. brucei) |
Key Differences: T. brucei vs T. cruzi
| Feature | T. brucei (African) | T. cruzi (American) |
|---|---|---|
| Vector | Tsetse fly (Glossina) | Triatomine/kissing bug |
| Transmission route | Saliva (anterior station) | Feces (posterior station) |
| Stages in human | Trypomastigote only | Trypomastigote + Amastigote |
| Intracellular phase | None - entirely extracellular | Yes - amastigotes in cells |
| Divides in blood | Yes - actively | No - non-dividing in blood |
| Kinetoplast | Small, posterior | Large, terminal/subterminal |
| VSG antigenic variation | Yes (classic feature) | No |
| Infective stage location in vector | Salivary gland | Hindgut (feces) |
Antigenic Variation - The Key Immune Evasion Mechanism
T. brucei is coated with a dense layer of ~10⁷ molecules of Variant Surface Glycoprotein (VSG). When the host's antibodies eliminate one VSG variant, a small number of parasites expressing a different VSG gene escape destruction and repopulate the bloodstream. Each trypanosome carries ~1000 different VSG genes. This cyclical process of antibody elimination and VSG switching produces the characteristic waves of parasitemia seen in African trypanosomiasis and makes vaccine development extremely difficult.
Sources: Medical Microbiology 9e; Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Tietz Textbook of Laboratory Medicine 7th Ed.
life cycle of trchomonas vaginalis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I have all the content and images needed. Here is the complete, detailed answer:
Life Cycle of Trichomonas vaginalis
The Most Important Concept: Only ONE Stage Exists
Unlike virtually every other pathogenic protozoon, T. vaginalis has no cyst stage. It exists only as a trophozoite throughout its entire life cycle. There is no environmental resistant form - it lives exclusively in the human urogenital tract and dies rapidly outside of it. This means:
- The entire life cycle occurs within humans
- There is no soil, water, or environmental phase
- Transmission requires direct host-to-host contact
Life Cycle Diagram
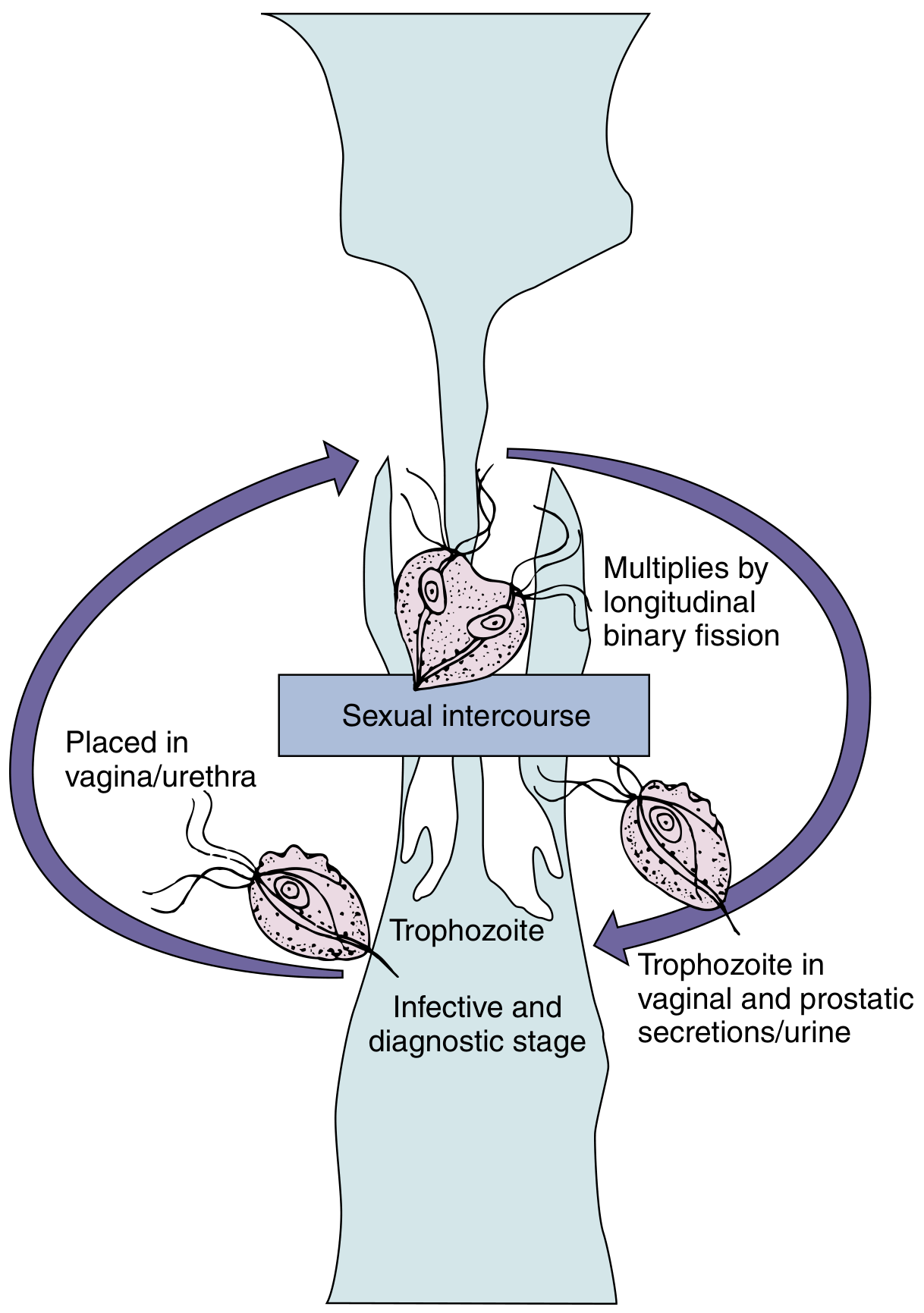
Fig. 72.5 - Life cycle of Trichomonas vaginalis. Medical Microbiology 9e
Morphology of the Trophozoite
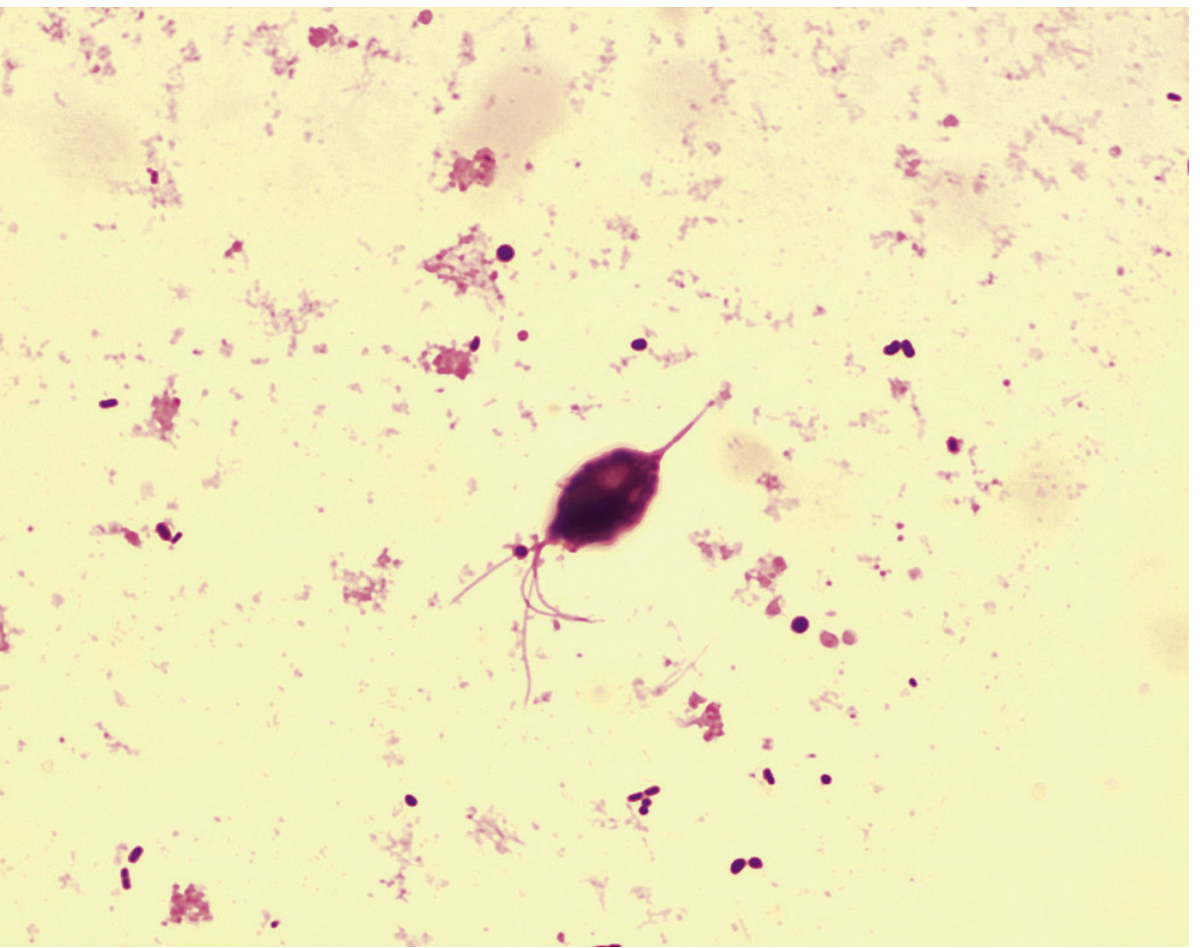
Fig. 72.6 - T. vaginalis trophozoite. Medical Microbiology 9e
Key Morphological Features
| Feature | Detail |
|---|---|
| Shape | Pyriform (pear-shaped) |
| Size | 7-23 µm long × 6-8 µm wide (average 13 × 7 µm) |
| Flagella | 4 free flagella arising from a single anterior stalk; 5th forms the undulating membrane |
| Undulating membrane | Short - extends only half the length of the body (unlike T. hominis where it extends the full length) |
| Axostyle | A stiff rod-like structure running through the center of the body and protruding posteriorly |
| Nucleus | Single, oval, anterior |
| Motility | Tumbling, rolling motion ("falling leaf") due to flagellar action |
| Cyst stage | ABSENT - no cyst ever formed |
Step-by-Step Life Cycle
Step 1 - Trophozoite in the Source Host
In an infected person, T. vaginalis trophozoites reside on and within the mucosal surfaces of the urogenital tract. Sites of colonization differ by sex:
In females:
- Vagina (primary site)
- Cervix
- Urethra
- Vulva
- (Does NOT normally extend to the uterus or fallopian tubes)
In males:
- Urethra (primary)
- Prostate gland
- Seminal vesicles
- (Men are most commonly asymptomatic carriers)
Trophozoites adhere to mucosal epithelium via surface adhesins and cause minute ulcerations through cytotoxic mechanisms and direct contact.
Step 2 - Replication by Longitudinal Binary Fission
T. vaginalis trophozoites multiply asexually by longitudinal binary fission (splitting lengthwise, along the long axis of the body). There is NO sexual reproduction stage and NO cyst formation at any point. The organism divides and replicates while remaining in the urogenital tract mucosa.
- Optimal pH for growth: 5.5-6.0 (the normal vaginal pH is 3.8-4.2, but T. vaginalis infection raises it to >4.5)
- The organism is anaerobic/microaerophilic - it lacks classic mitochondria, instead possessing hydrogenosomes (organelles that produce H₂ and CO₂ from pyruvate)
Step 3 - Shedding into Secretions (Infective & Diagnostic Stage)
Living trophozoites are shed into:
- Vaginal secretions (in women)
- Prostatic secretions (in men)
- Urine (in both sexes)
These secretions containing live trophozoites constitute both the infective stage and the diagnostic stage - the same form that infects a new host is the same form detected in laboratory specimens.
Step 4 - Transmission to a New Host
Primary Route: Sexual Intercourse
Transmission occurs almost exclusively through direct genital-to-genital contact during sexual intercourse. The trophozoites are deposited in the vagina or urethra of the new host. The incubation period is 5 to 28 days.
Secondary/Rare Routes:
- Fomites (toilet articles, shared underclothing, wet towels) - very limited because trophozoites are fragile and die rapidly when desiccated or cooled
- Neonatal infection - infants may acquire infection by passage through an infected mother's birth canal during delivery; rarely causes neonatal pneumonia and conjunctivitis
- NOT fecal-oral - unlike intestinal protozoa, T. vaginalis is NOT transmitted this way
Step 5 - Colonization of New Host's Urogenital Tract
After being deposited in the new host's urogenital tract, trophozoites:
- Adhere to urogenital epithelial cells via surface lectins and adhesins
- May undergo morphological change from pyriform to ameboid form when attached to epithelial surfaces (this pseudopod extension form aids in cytotoxicity and adherence)
- Begin multiplying by binary fission
- Cause tissue damage through contact-dependent cytotoxicity, release of cysteine proteases, and induction of host inflammatory response
- The cycle repeats indefinitely until treatment is given
Life Cycle Summary
INFECTED HOST NEW HOST
─────────────────────────────────────────────────────
Trophozoite colonizes vagina/urethra/prostate
│
▼
Multiplies by longitudinal binary fission
(no cyst ever formed)
│
▼
Trophozoites shed in vaginal secretions /
prostatic secretions / urine
│ [INFECTIVE STAGE = DIAGNOSTIC STAGE]
│
▼ SEXUAL INTERCOURSE (primary route)
Trophozoites deposited in
vagina or urethra of new host
│
▼
Adhere to mucosal epithelium
│
▼
Colonize and multiply
by binary fission
│
▼
[CYCLE REPEATS]
Why T. vaginalis Has No Cyst Stage
The absence of a cyst stage is directly linked to its transmission strategy. Since it is transmitted by direct sexual contact (moist, warm, body-temperature environment), it never needs to survive in a dry, cold, or hostile external environment. The cyst stage in other protozoa (e.g., Giardia, Entamoeba) evolved as a survival mechanism for fecal-oral transmission through soil and water - none of which applies to T. vaginalis. This is why:
- Trophozoites die rapidly outside the body
- Fomite transmission is rare and inefficient
- The parasite is entirely dependent on continuous sexual transmission
Comparison: T. vaginalis vs Other Flagellates
| Feature | T. vaginalis | Giardia lamblia | T. brucei |
|---|---|---|---|
| Cyst stage | Absent | Present | Absent |
| Location | Urogenital tract | Small intestine | Blood/CNS |
| Transmission | Sexual intercourse | Fecal-oral | Tsetse fly bite |
| Replication | Binary fission | Binary fission | Binary fission |
| Flagella | 4 anterior + 1 undulating | 8 | 1 with full undulating membrane |
| Infective stage | Trophozoite | Cyst | Metacyclic trypomastigote |
| Intracellular | No | No | No |
Clinical Correlations of the Life Cycle
| Life Cycle Feature | Clinical Consequence |
|---|---|
| No cyst - only trophozoite | Rapid death outside host; contact precautions mainly apply to sexual contact |
| Resides on mucosal surface | Strawberry cervix (punctate hemorrhages), frothy yellow-green malodorous discharge |
| Raises vaginal pH > 4.5 | Positive whiff test; amine (fishy) odor on KOH preparation |
| Males are asymptomatic carriers | Reservoir for reinfection of female partners; both partners MUST be treated |
| Neonatal acquisition via birth canal | Neonatal conjunctivitis, pneumonia (rare) |
| Mucosal ulceration | ~2× increased risk of HIV acquisition and transmission |
| No immune memory | Reinfection can occur repeatedly; no lasting immunity |
Treatment Note
Both sex partners must be treated simultaneously to break the transmission cycle. The drugs of choice are metronidazole or tinidazole (nitroimidazole class). Treating only the symptomatic partner leads to inevitable reinfection from the untreated (often asymptomatic male) partner.
Sources: Medical Microbiology 9e; Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Henry's Clinical Diagnosis & Management by Laboratory Methods; Tietz Textbook of Laboratory Medicine, 7th Ed.
pathogenesis of T. vaginalis in detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
Trichomonas vaginalis pathogenesis mechanism adherence virulence factors cytotoxicity protease
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11132421
Reading File
Loading Image
Reading File
I now have comprehensive, multi-source content. Here is the detailed pathogenesis:
Pathogenesis of Trichomonas vaginalis - Detailed
The pathogenesis of T. vaginalis is multifactorial - no single mechanism explains all tissue damage. It involves a sequence of events: colonization of the urogenital mucosa, contact-dependent and contact-independent cytotoxicity, protease-mediated injury, immune activation and evasion, and disruption of the vaginal microenvironment.
Structural Basis for Pathogenicity
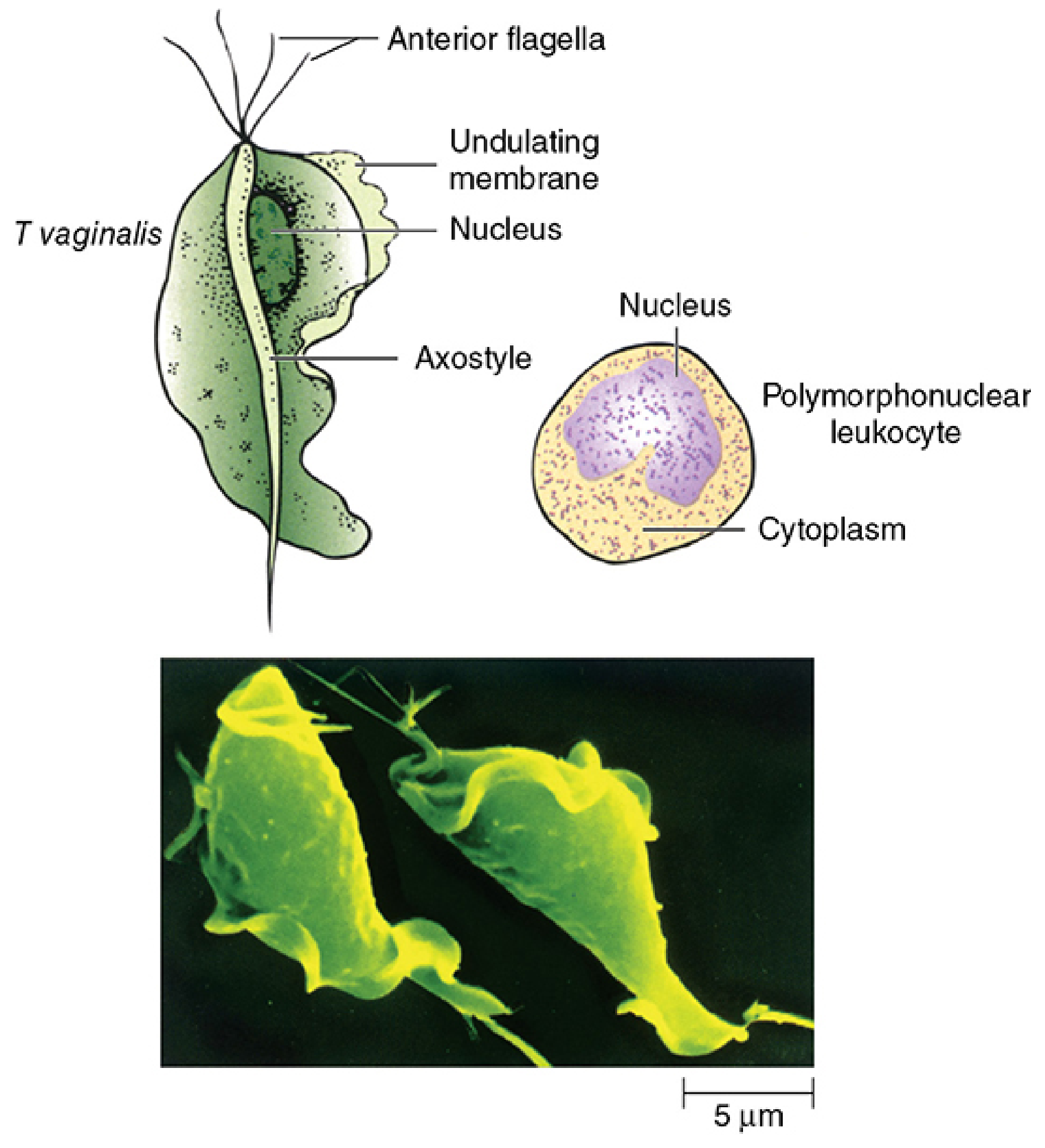
Fig. 53-1 - T. vaginalis trophozoite structure and SEM. Sherris & Ryan's Medical Microbiology, 8th Ed.
The trophozoite possesses several structures that directly contribute to pathogenesis:
- Axostyle - a rigid microtubule-containing rod that bisects the cell and protrudes posteriorly; the pointed tip is thought to mediate mechanical attachment to epithelial cells
- Undulating membrane - generates movement and helps in mucosal surface contact
- Flagella (4 anterior + 1 membrane-associated) - drive jerky, nondirectional motility that enables mucosal penetration
- Surface adhesins, lectins, and laminin-binding proteins - mediate specific host-cell recognition and binding
Step-by-Step Pathogenic Sequence
Step 1: Colonization - pH and Hormonal Prerequisites
After sexual transmission, trophozoites enter the vagina, where the microenvironment determines susceptibility:
- Normal vaginal pH is 3.8-4.2 (acidic, hostile to most pathogens)
- T. vaginalis grows optimally at pH 5.5-6.0 - it cannot establish infection in a fully acidic environment
- Several factors facilitate colonization:
- Elevated pH due to semen, menstrual blood, or co-existing bacterial vaginosis
- Estrogen status - estrogen increases glycogen in vaginal epithelial cells, which raises pH and provides nutrients for the parasite
- Neonatal infection - high maternal estrogen temporarily lowers neonatal vaginal pH to a susceptible range; once estrogen drops, the parasite is naturally cleared
- Symptoms worsen during menstruation and pregnancy because pH rises during these states, promoting parasite multiplication
Step 2: Morphological Transformation - Pyriform to Ameboid
A critical and unique step in pathogenesis is a shape change:
- In suspension or urine, trophozoites are oval/pyriform with active flagellar movement
- On contact with the vaginal epithelium, trophozoites retract their flagella and transform into a flattened, pseudopod-forming ameboid shape
- This shape change dramatically increases surface contact area with host epithelial cells
- It is triggered by host cell contact and is a prerequisite for effective adhesion and cytotoxicity
- This transformation is reversible - organisms revert to pyriform when detached
Step 3: Adherence to Mucosal Epithelium
Adherence is the critical initiating step of pathogenesis. It involves multiple molecular interactions:
Adhesins (Surface Proteins)
- T. vaginalis expresses at least four surface adhesin proteins (AP23, AP33, AP51, AP65) that bind to vaginal epithelial cells
- AP65 is the most studied and most important - it is upregulated on contact with host cells
- Adhesin expression is iron-regulated - higher iron availability in vaginal secretions (e.g., during menstruation) upregulates adhesin production, explaining increased severity during menses
Lectin-Mediated Binding
- Trophozoites express lectin-binding carbohydrates on their surface
- These bind to galectins (e.g., galectin-1) expressed on host epithelial cell surfaces
- This lectin-carbohydrate interaction is species-specific and site-specific
Laminin-Binding Proteins
- The parasite expresses proteins that bind to laminin in the extracellular matrix beneath the epithelium
- This facilitates deeper attachment once the surface epithelium is disrupted
Axostyle-Mediated Mechanical Attachment
- The protruding pointed tip of the axostyle physically inserts into epithelial cell surfaces, providing a mechanical anchor for firm adhesion
Step 4: Contact-Dependent Cytotoxicity (Primary Mechanism)
Once firmly adhered, the trophozoite kills host epithelial cells by direct cell-to-cell contact. This is the dominant cytopathic mechanism:
Cysteine Proteases (Most Important Virulence Factors)
- T. vaginalis secretes a family of cysteine proteinases (CPs) - at least 20-23 distinct CPs have been identified
- The most important is CP65 (a 65 kDa cysteine protease, also called TvCP65)
- These proteases:
- Degrade extracellular matrix proteins (fibronectin, collagen, laminin) - loosening the epithelial surface
- Cleave host cell surface proteins causing membrane destabilization
- Disrupt tight junctions between epithelial cells
- Enable deeper tissue penetration through the mucous layer
- CP activity is iron-dependent and upregulated under iron-replete conditions
Metalloprotease TvMP50
- A 50 kDa zinc-dependent metalloproteinase that directly contributes to host cell lysis
- Antibody to TvMP50 reduces epithelial cell killing by ~20%, confirming its direct role
- TvROM1 (a rhomboid-type protease) overexpression increases host cell lysis 4-fold
Contact-Dependent Cytolytic Process
- Direct killing proceeds through necrosis (not apoptosis) - host cell cytosol is released, indicating plasma membrane rupture
- Some studies show the parasite also phagocytoses (engulfs and eats) host epithelial cells and erythrocytes - a behavior called "trogocytosis" or phagocytic activity
Step 5: Contact-Independent Cytotoxicity (Secondary Mechanism)
T. vaginalis also damages cells it does not directly touch:
- A 200 kDa glycoprotein (heat- and acid-labile) is secreted into the surrounding environment and causes cell damage at a distance
- Secreted cysteine proteases in vaginal fluid can degrade host proteins remotely
- Hemolysins - the parasite secretes factors that lyse red blood cells (important when blood is present during menstruation)
- These contact-independent mechanisms contribute to the diffuse mucosal inflammation seen even beyond immediate parasite contact zones
Step 6: Innate Immune Activation and Inflammation
Toll-Like Receptor (TLR) Activation
- T. vaginalis surface components (lipoglycans and lipophosphoglycans) activate host TLR2 and TLR4 on vaginal epithelial cells and macrophages
- TLR activation triggers the NF-κB signaling pathway
- This leads to production of proinflammatory cytokines: IL-8, IL-6, TNF-α, IL-1β
Neutrophil Recruitment and Tissue Damage
- Cytokines recruit massive neutrophil (PMN) infiltration - the characteristic finding in trichomoniasis
- Neutrophils can kill T. vaginalis by trogocytosis (nibbling of the parasite's membrane) - a recently described mechanism
- However, neutrophils also release elastase and reactive oxygen species (ROS), causing collateral bystander tissue damage to the epithelium
- The characteristic "strawberry cervix" (colpitis macularis) - punctate hemorrhagic spots on the cervix - represents petechial hemorrhages from neutrophil-mediated microvasculature damage
CD4+ T Cell Response
- A CD4+ T helper response follows, contributing to adaptive immunity
- However, this does not produce lasting protective immunity - reinfection occurs readily
Step 7: Vaginal Microenvironment Disruption
T. vaginalis actively disrupts the protective vaginal microbiome:
- Healthy vagina is dominated by Lactobacillus species which maintain acidic pH (3.8-4.2) via lactic acid production
- T. vaginalis infection is strongly associated with bacterial vaginosis (BV) - dysbiosis of vaginal flora
- Mechanisms of microbiome disruption include:
- Parasite consumption of glycogen (the substrate Lactobacillus uses for lactic acid production) → loss of acidic pH → further parasite proliferation (a self-amplifying cycle)
- Inflammatory cytokines suppress Lactobacillus growth
- The parasite itself may directly inhibit Lactobacillus adherence to epithelium
- Loss of Lactobacillus → rise in pH → overgrowth of anaerobes → clinical BV pattern
- This bidirectional relationship means T. vaginalis and BV often co-exist and worsen each other
Step 8: Immune Evasion Mechanisms
T. vaginalis has evolved multiple strategies to persist despite immune activation:
Immunoglobulin Degradation
- Secreted cysteine proteases degrade IgG and IgA in vaginal secretions - destroying the primary antibody defense at the mucosal surface
- This is a critical immune evasion strategy that allows chronic persistence
Antigenic Variation
- T. vaginalis undergoes phenotypic variation of surface antigens (analogous to but mechanistically distinct from T. brucei VSG switching)
- Different clinical isolates express different surface antigen profiles
- This prevents the host from generating effective antibody responses to clear the infection
- It explains why repeated infections occur despite prior antibody production
Complement Evasion
- T. vaginalis acquires host complement regulatory proteins (Factor H, C4b-binding protein) from the host plasma onto its own surface
- This "molecular camouflage" prevents complement activation and membrane attack complex formation against the parasite
Mycoplasma Endosymbionts
- T. vaginalis harbors two mycoplasma species (Mycoplasma hominis and a second species) as intracellular endosymbionts
- These endosymbionts contribute to T. vaginalis virulence by:
- Amplifying the host inflammatory response (mycoplasma LPS activates TLRs independently)
- Potentially being transmitted to host tissue during trophozoite lysis
Trichomonas Vaginalis Virus (TVV)
- Many T. vaginalis strains harbor TVV (Trichomonas Vaginalis Virus), a double-stranded RNA endovirus
- TVV-positive strains express higher levels of cysteine proteases and surface antigens
- TVV-positive infections are associated with more severe symptoms
- Interestingly, isolates WITHOUT TVV are more likely to show metronidazole resistance
Step 9: Consequences - HIV Susceptibility, Obstetric Complications
The pathogenic mechanisms above lead to important clinical consequences beyond local symptoms:
HIV Susceptibility (2× Increased Risk)
- Mucosal ulceration and erosion create portals of entry for HIV
- Massive neutrophil and CD4+ T cell infiltration bring HIV target cells (CD4+ T cells, macrophages) to the site of infection in abundance
- Proinflammatory cytokines (TNF-α, IL-1β) upregulate HIV replication in latently infected cells
- HIV-positive men with T. vaginalis have higher HIV concentrations in semen, increasing transmission to partners
Adverse Pregnancy Outcomes
- Mucosal inflammation and cytokine production (especially IL-8, IL-6) can trigger prostaglandin release → uterine contractions → preterm labor
- Associated with premature rupture of membranes (PROM) and low birth weight
- Infected women also have higher rates of posthysterectomy cuff infections
Pelvic Inflammatory Disease (PID)
- Especially in HIV-positive women, T. vaginalis infection significantly increases risk of PID
- Ascent of the infection and secondary bacterial co-infection can reach the upper genital tract
Summary: Virulence Factors and Their Roles
| Virulence Factor | Mechanism | Effect |
|---|---|---|
| Adhesins (AP23, AP33, AP51, AP65) | Bind host epithelial receptors | Cytoadherence - initiates infection |
| Axostyle | Mechanical penetration | Firm attachment to epithelium |
| Cysteine proteases (CP65, TvCP2) | Degrade ECM and surface proteins; cleave IgG/IgA | Tissue damage + immune evasion |
| Metalloprotease TvMP50 | Zinc-dependent lysis | Direct host cell killing |
| 200 kDa glycoprotein | Secreted cytotoxin | Contact-independent cell damage |
| Hemolysins | Lyse RBCs | Tissue destruction, iron acquisition |
| Lipoglycans | Activate TLR2/TLR4 | Proinflammatory cytokine cascade |
| Surface antigen variation | Phenotypic switch | Escape from antibody response |
| Complement regulatory proteins (Factor H) | Molecular camouflage | Block complement attack |
| TVV endovirus | Upregulates cysteine proteases | Enhanced virulence |
| Mycoplasma endosymbionts | Independent TLR activation | Amplified inflammation |
Why Infection Is Often Asymptomatic
Despite these virulence mechanisms, up to 50% of infections are asymptomatic. This reflects a balance between:
- Host factors: normal acidic pH, intact Lactobacillus microbiome, competent innate immunity
- Parasite factors: lower iron availability reduces adhesin/protease expression; low parasite load
- Strain variation: TVV-negative strains are less virulent; different adhesin expression profiles
- Men are particularly likely to be asymptomatic because voiding urine mechanically flushes organisms from the urethra repeatedly, limiting colonization density
Sources: Sherris & Ryan's Medical Microbiology, 8th Ed.; Medical Microbiology 9e; Tietz Textbook of Laboratory Medicine, 7th Ed.; Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Trichomonas vaginalis: Pathogenesis, Symbiont Interactions, and Host Cell Immune Responses (PMC); Biological roles of cysteine proteinases in pathogenesis of T. vaginalis (PMC)
This is a shared conversation. Sign in to Orris to start your own chat.