Short bowel syndrome flowchart
"short bowel syndrome" management
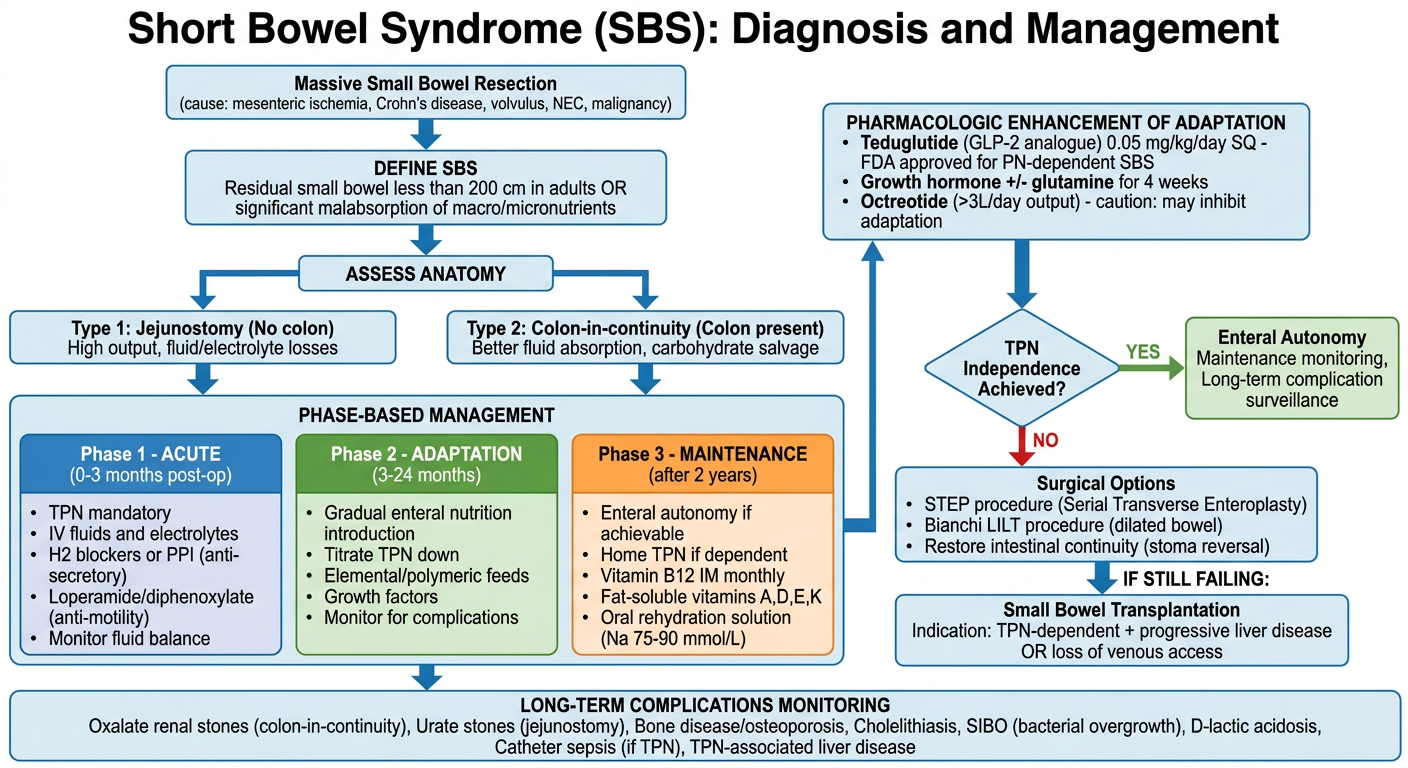
A detailed clinical flowchart titled "Short Bowel Syndrome (SBS): Diagnosis and Management" with the following structure: TOP BOX: "Massive Small Bowel Resection" (cause: mesenteric ischemia, Crohn's disease, volvulus, NEC, malignancy) Arrow down to: "DEFINE SBS" box: Residual small bowel less than 200 cm in adults OR significant malabsorption of macro/micronutrients Arrow down to: "ASSESS ANATOMY" - two branches side by side: LEFT branch: "Type 1: Jejunostomy (No colon)" - High output, fluid/electrolyte losses RIGHT branch: "Type 2: Colon-in-continuity (Colon present)" - Better fluid absorption, carbohydrate salvage Both branches arrow down to: "PHASE-BASED MANAGEMENT" - 3 columns: Column 1: "Phase 1 - ACUTE (0-3 months post-op)" with bullets: TPN mandatory, IV fluids and electrolytes, H2 blockers or PPI (anti-secretory), Loperamide/diphenoxylate (anti-motility), Monitor fluid balance Column 2: "Phase 2 - ADAPTATION (3-24 months)" with bullets: Gradual enteral nutrition introduction, Titrate TPN down, Elemental/polymeric feeds, Growth factors, Monitor for complications Column 3: "Phase 3 - MAINTENANCE (after 2 years)" with bullets: Enteral autonomy if achievable, Home TPN if dependent, Vitamin B12 IM monthly, Fat-soluble vitamins A,D,E,K, Oral rehydration solution (Na 75-90 mmol/L) Arrow down to: "PHARMACOLOGIC ENHANCEMENT OF ADAPTATION" box: - Teduglutide (GLP-2 analogue) 0.05 mg/kg/day SQ - FDA approved for PN-dependent SBS - Growth hormone +/- glutamine for 4 weeks - Octreotide (>3L/day output) - caution: may inhibit adaptation Arrow down to diamond: "TPN Independence Achieved?" YES arrow to: "Enteral Autonomy - Maintenance monitoring, Long-term complication surveillance" NO arrow to: "Surgical Options" box: - STEP procedure (Serial Transverse Enteroplasty) - Bianchi LILT procedure (dilated bowel) - Restore intestinal continuity (stoma reversal) IF STILL FAILING: arrow to "Small Bowel Transplantation" box: Indication: TPN-dependent + progressive liver disease OR loss of venous access BOTTOM BOX: "LONG-TERM COMPLICATIONS MONITORING": Oxalate renal stones (colon-in-continuity), Urate stones (jejunostomy), Bone disease/osteoporosis, Cholelithiasis, SIBO (bacterial overgrowth), D-lactic acidosis, Catheter sepsis (if TPN), TPN-associated liver disease Use a clean medical diagram style with color-coded phases (blue for acute, green for adaptation, orange for maintenance), clear arrows, white background, readable fonts, professional clinical appearance.
Short Bowel Syndrome (SBS) - Full Flowchart Breakdown
Definition
Step 1 - Identify the Cause
- Adults: mesenteric ischemia, Crohn's disease, malignancy
- Pediatrics: NEC (35%), intestinal atresia (25%), gastroschisis (18%), midgut volvulus (14%)
Step 2 - Assess Anatomy (Critical for Prognosis)
| Feature | Jejunostomy (no colon) | Colon-in-continuity |
|---|---|---|
| TPN threshold | < 100 cm jejunum | < 60 cm jejunum |
| Main problem | High Na/fluid losses | Oxalate stone risk |
| Colonic benefit | None | Fluid + carbohydrate salvage |
| Diet | High-salt, small meals | High complex carbohydrate |
Step 3 - Phase-Based Management
- Mandatory TPN + IV fluid/electrolyte resuscitation
- PPI or H2 blocker (hypergastrinemia lasts 1-2 years post-op)
- Anti-motility agents: loperamide 2-8 mg QID, diphenoxylate, or codeine 15-60 mg QID
- Octreotide 100-250 mcg SQ TID if output > 3 L/day (caution: inhibits adaptation at > 300 mcg/day)
- Gradually introduce enteral nutrition once ileus resolves
- Titrate TPN down as enteral tolerance improves
- Intestinal adaptation driven by: enteral nutrients, GLP-2, EGF, IGF-1, TGF-alpha, IL-11
- Oral rehydration solution with Na 75-90 mmol/L (best absorbed)
- Vitamin B12 500-1000 mcg IM/SC monthly (ileum-specific absorption lost)
- Fat-soluble vitamins A, D, E, K supplementation
- Mg as liquid preparation sipped throughout day (oral Mg causes osmotic diarrhea)
- Home TPN if enteral autonomy not achieved
Step 4 - Pharmacologic Enhancement of Adaptation
| Drug | Dose | Mechanism | Notes |
|---|---|---|---|
| Teduglutide (GLP-2 analogue) | 0.05 mg/kg/day SQ | Stimulates intestinal adaptive hyperplasia, increases villus height | FDA-approved for PN-dependent SBS; reduces PN days/volume |
| Growth hormone +/- glutamine | 0.1 mg/kg/day SQ x 4 weeks; glutamine 30 g/day PO | Trophic effects | Reduces PN requirements |
| Octreotide | 100-250 mcg SQ TID | Reduces GI secretions | Risk of inhibiting adaptation; use only for high-output |
Step 5 - Surgical Options (if TPN-dependent after adaptation)
- Stoma reversal - restore continuity first to use all residual bowel
- STEP procedure (Serial Transverse Enteroplasty) - serial stapling of dilated bowel; 47% achieved enteral autonomy at 21 months follow-up
- Bianchi LILT (Longitudinal Intestinal Lengthening and Tailoring) - doubles bowel length; technically demanding, mostly pediatric use
- Small Bowel Transplantation - indicated when TPN-dependent + progressive liver failure OR loss of central venous access. 5-year survival on TPN: 50-75%.
Long-Term Complications to Monitor
- Renal stones: oxalate (colon-in-continuity) or urate (jejunostomy)
- Bone disease / osteoporosis
- Gallstones (bile acid disruption)
- SIBO (bacterial overgrowth)
- D-lactic acidosis
- Catheter sepsis, venous thrombosis, TPN-associated liver disease