tuberculosis complete with abdominal and tbm
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, detailed answer.
Tuberculosis: Complete Review
Overview and Epidemiology
Tuberculosis (TB) is caused by Mycobacterium tuberculosis, an obligate intracellular aerobe, and remains the world's leading infectious disease killer. In 2018, approximately 10 million new TB cases were reported globally with 1.5 million deaths. Latent TB infects one-quarter of the world's population, carrying a lifetime reactivation risk of 5-15%. HIV coinfection accounts for ~9% of new cases and dramatically raises the risk - the incidence of TB in persons with full-blown HIV is nearly 500 times that of the general population.
Extrapulmonary TB (EPTB) accounts for 15% of global TB cases. Most commonly affected sites:
- Lymphatic
- Pleural
- Skeletal
- Genitourinary
- Gastrointestinal (next most common)
- CNS (~5% of EPTB in the US)
I. PULMONARY TUBERCULOSIS
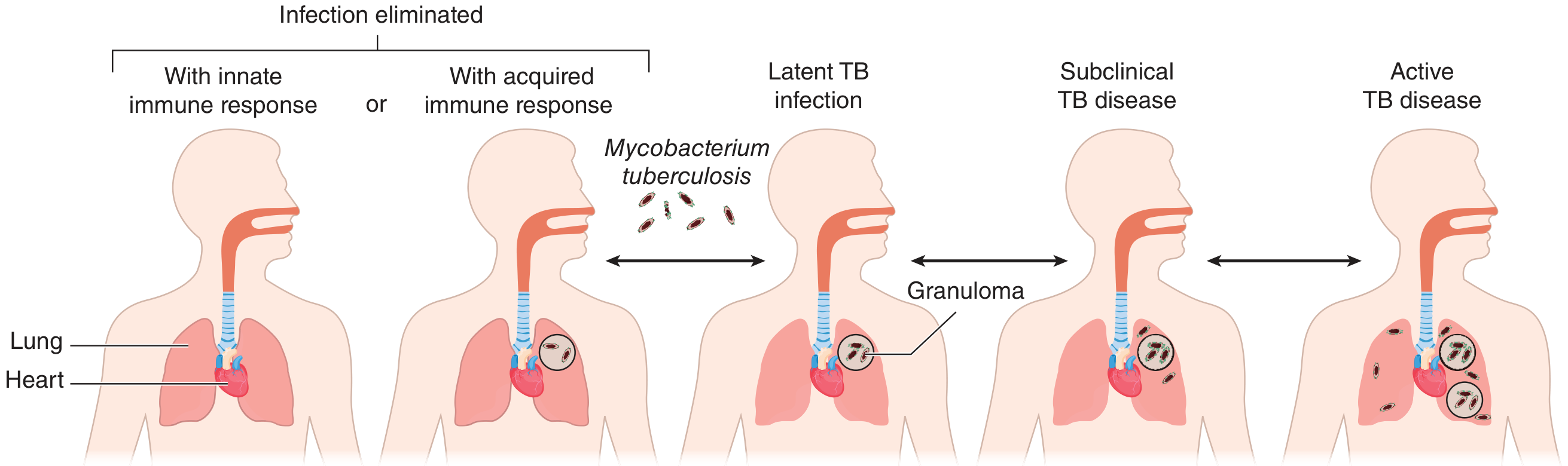
Pathogenesis and Disease Spectrum
After initial infection, the spectrum of outcomes includes:
- Bacterial elimination (no disease)
- Latent TB infection (TST/IGRA positive, asymptomatic, culture negative)
- Subclinical disease
- Progressive primary disease (within 1 year of infection)
- Reactivation (post-primary disease, distant from initial infection)
Clinical Features
- Most common symptom: Persistent cough (productive or nonproductive) - up to 25% of culture-confirmed cases do not report cough
- Constitutional symptoms: Fever, chills, night sweats, weight loss
- Hemoptysis - occurs in advanced disease
- Physical exam: Post-tussive rales in upper lung zones; amphoric breath sounds indicate a cavity; lymphadenopathy uncommon in immunocompetent adults
Chest Radiology
- Primary TB: Parenchymal consolidation, hilar/paratracheal lymphadenopathy, pleural effusion
- Post-primary/Reactivation: Upper lobe predominance, cavitation, fibrosis, volume loss
- Miliary TB: Diffuse 1-2 mm nodules throughout both lung fields
TB Pleuritis
TB pleuritis is due to a type IV (delayed) hypersensitivity reaction triggered by release of TB antigens into the pleural space from rupture of subpleural disease. Key points:
- Pleural fluid is exudative, predominantly lymphocytic
- Fulminant TB empyema is much rarer
- 10% of patients develop restrictive spirometric defects after a median of 23 months
- Cochrane evidence shows oral corticosteroids may improve radiographic appearances of residual pleural changes but do not improve long-term respiratory function and are associated with more adverse events
II. ABDOMINAL TUBERCULOSIS
Abdominal TB encompasses three main compartments: gastrointestinal (intestinal), peritoneal, and lymph node disease.
A. Gastrointestinal (Intestinal) Tuberculosis
Epidemiology:
- 3.5% of extrapulmonary cases in the US
- Ileocecal region: most common site (64% of GI TB cases), followed by jejunum and colon
- Only 15-25% of GI TB cases have concomitant pulmonary TB
- M. bovis from unpasteurized dairy products is an additional cause in developing countries
Pathogenesis routes:
- Swallowing of infected sputum (direct seeding)
- Hematogenous spread
- Lymphatic spread
- Direct spread from adjacent structures (lymph nodes, fallopian tubes)
Clinical Features:
- Abdominal pain and GI obstruction (most common presentation)
- Fever, nausea, diarrhea, weight loss
- Gastrointestinal bleeding
- Palpable mass in ileocecal region
- Can mimic Crohn disease, acute appendicitis, or carcinoma
Differential Diagnosis of Intestinal TB (Box 145.1 - Yamada's Gastroenterology):
- Crohn's disease (key mimic - granulomas are noncaseating, <400 μm, poorly organized)
- Appendicitis, malignancies (lymphoma, carcinoma)
- Sarcoidosis, amyloidosis
- NSAIDs-related enteropathy
- Infectious: Salmonellosis, Yersiniosis, Cytomegalovirus, Histoplasmosis, MAC enteritis
- Actinomycosis, Anisakiasis, Typhlitis, Eosinophilic enteritis, Vasculitides, Ischemia
Diagnosis:
- AFB smear/culture of tissue (gold standard but positive in <40% of cases with ZN staining positive in only ~3%)
- Endoscopic biopsy showing caseating granulomas
- PCR/Xpert MTB-RIF assay (sensitivity 50-100%, specificity 62-97% - further validation needed)
- CD4+ T-cell activation markers (CD38, HLA-DR, Ki67+) are being studied as differentiating tools
B. Peritoneal Tuberculosis
Pathogenesis: M. tuberculosis enters the peritoneal space from adjacent lymph nodes.
Clinical Features:
- Subacute abdominal pain, anorexia, abdominal swelling
- Systemic symptoms: fever, night sweats, weight loss
- Can mimic acute abdomen
- Often underlies liver disease (cirrhosis) - may obscure TB symptoms
- Intra-abdominal lymphadenopathy on CT
- Active pulmonary TB is uncommon in patients with TB peritonitis
- Fever + abdominal tenderness in a person with ascites should always prompt paracentesis
Ascitic Fluid Analysis:
| Parameter | Finding |
|---|---|
| Character | Exudative |
| WBC count | 50-10,000 leukocytes/μL, predominantly lymphocytes |
| AFB smear | Rarely positive |
| Culture | ~50% positive (increases with large volume) |
| SAAG | Low (<1.1 g/dL) in non-cirrhotic; high in cirrhotic (cirrhosis dominates) |
| ADA | High sensitivity 93-100%, specificity 96-97%; cut-off 36-40 IU/L (optimal 39 IU/L) |
Diagnosis:
- Laparoscopy with biopsy = best diagnostic test (characteristic findings + histology + culture)
- ADA in ascitic fluid: sensitivity 100%, specificity 97% at cut-off 39 IU/L (meta-analysis of 12 studies)
- In cirrhotic patients, ADA may be less sensitive (but not confirmed by systematic reviews)
- Paracentesis mandatory whenever TB peritonitis is suspected
III. TUBERCULOUS MENINGITIS (TBM)
Pathogenesis
TBM results from two sequential events:
- Hematogenous seeding of meninges and subpial regions → formation of tubercles
- Rupture of one or more tubercles → discharge of bacteria into the subarachnoid space
The rich's concept: TBM always originates from a subependymal tubercle (part of miliary disease), though conventional hematogenous implantation is debated.
Pathological Findings
- Small, discrete white tubercles scattered over the base of the cerebral hemispheres (and lesser degree on convexities)
- Thick, gelatinous exudate accumulates in basal meninges - obliterating the pontine and interpeduncular cisterns, extending to the floor of the 3rd ventricle, optic chiasm, and undersurfaces of temporal lobes
- Microscopically: central zone of caseation surrounded by epithelioid cells, giant cells, lymphocytes, plasma cells
- Cranial nerves frequently involved as they traverse the subarachnoid space
- Arteries become inflamed and occluded → brain infarction
- Blockage of basal cisterns → obstructive hydrocephalus
- Process is a true meningoencephalitis (penetrates pia and ependymia into brain parenchyma)
MRI in Tuberculous Meningitis
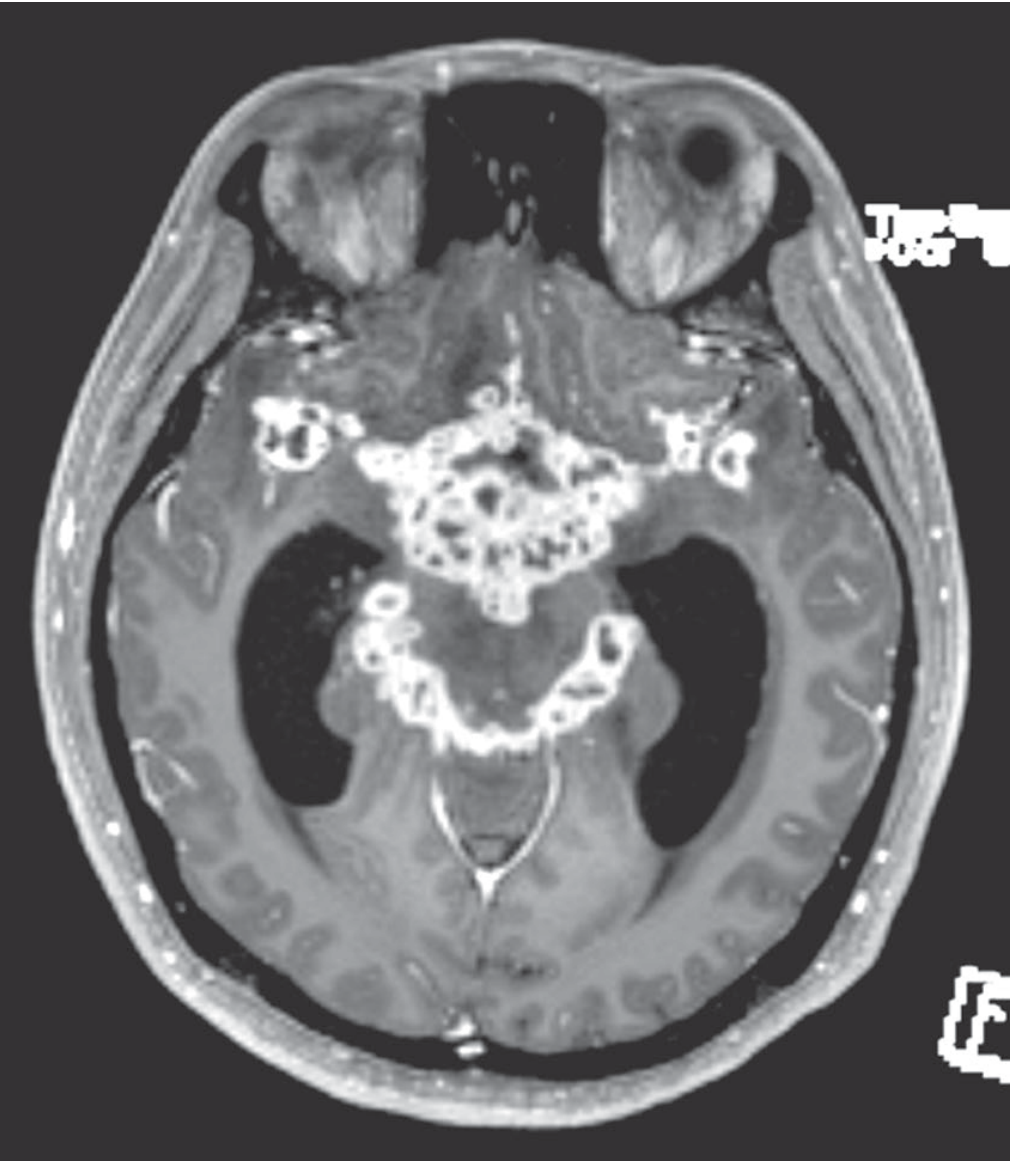
Gadolinium-enhanced MRI demonstrating enhancement of basal meninges reflecting multiple abscesses, with accompanying hydrocephalus and cranial nerve palsies (Adams & Victor's Principles of Neurology, 12th ed.).
Clinical Features
Prodrome (weeks 1-2):
- Low-grade fever, malaise, headache (>50% of cases), lethargy, confusion
- Stiff neck (75% of cases), Kernig and Brudzinski signs
- Symptom evolution over 1-2 weeks - much slower than bacterial meningitis
In young children and infants: Apathy, hyperirritability, vomiting, seizures - stiff neck may be absent
Later features (reflecting basal disease):
- Cranial nerve palsies - ocular palsies (most common), facial palsy, deafness - in 20% at diagnosis
- Papilledema
- Diplopia (basilar exudate) - up to 70% of patients
- Focal neurologic deficit from hemorrhagic infarction
- Hypothermia and hyponatremia (SIADH is common)
- Lacunar infarcts / movement disorders (basal ganglia vessel involvement)
- Hemiparesis / hemiplegia (middle cerebral artery involvement)
- Ultimate evolution: coma, hydrocephalus, intracranial hypertension
In ~two-thirds of TBM patients: Evidence of active TB elsewhere (usually lungs, occasionally small bowel, bone, kidney, or ear)
CSF Findings
| Parameter | Finding in TBM |
|---|---|
| Opening pressure | Elevated |
| Leukocytes | Up to 1000/μL (up to 1500); lymphocyte predominance; PMNs may predominate early |
| Protein | Elevated 1-8 g/L (100-800 mg/dL) |
| Glucose | Low (typically) |
| AFB smear | Infrequently positive (repeated LPs increase yield) |
| Culture | Positive up to 80% - gold standard |
| Xpert MTB/RIF | Sensitivity up to 80% - preferred initial test |
Neuroradiology (Classic Triad on CT/MRI)
- Basal meningeal enhancement
- Hydrocephalus
- Cerebral or brainstem infarction
Tuberculoma
- Tumor-like masses of tuberculous granulation tissue, 2-12 mm
- Multiple or single, in brain parenchyma
- Can cause mass effect, periventricular obstructive hydrocephalus, seizures, focal signs
- CT/MRI: contrast-enhanced ring lesions
- In developing countries: 5-30% of all intracranial mass lesions
- CSF: small lymphocytosis, increased protein, glucose not reduced (serous meningitis pattern)
- Biopsy required for diagnosis; responds to anti-TB drugs
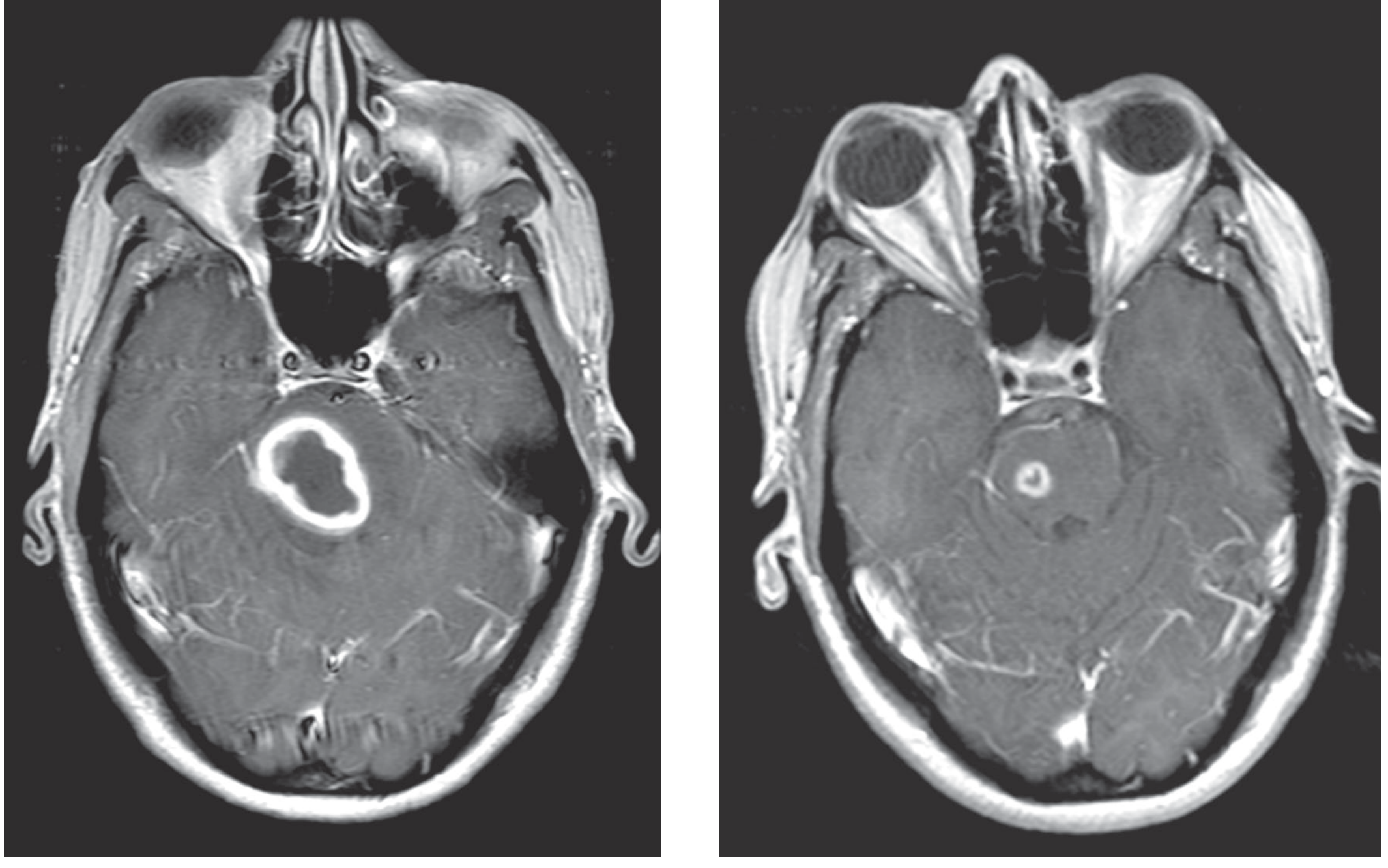
Tuberculoma of the pons on gadolinium-enhanced MRI (left: thick uniform enhancing rim; right: same lesion after antituberculous treatment) - Adams & Victor's Neurology.
Tuberculous Serous Meningitis
A self-limited meningitis from adjacent tuberculous focus. CSF: modest pleocytosis, normal/elevated protein, normal glucose. Mild meningeal signs, headache, confusion.
IV. TREATMENT
Standard Anti-TB Regimen (All Forms)
Two-phase approach:
| Phase | Duration | Drugs | Notes |
|---|---|---|---|
| Intensive | 2 months | HRZE - Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) | 4-drug regimen |
| Continuation | 4 months | HR - Isoniazid + Rifampicin | 85% global success rate |
Patients at higher risk of relapse: up to 9 months total.
Dosing (Adults)
| Drug | Dose | Key Side Effects |
|---|---|---|
| Isoniazid (INH) | 5 mg/kg/day (single dose) | Peripheral neuropathy, hepatitis (give pyridoxine 50 mg/day to prevent neuropathy) |
| Rifampin | 10 mg/kg/day | Hepatitis, drug interactions, orange discoloration of secretions |
| Pyrazinamide | 20-35 mg/kg/day | Hepatitis, rash, GI upset, hyperuricemia |
| Ethambutol | 15 mg/kg/day | Optic neuropathy (visual acuity + red-green color discrimination monitoring required) |
| Ethionamide (MDR-TB) | 15-25 mg/kg/day (divided doses) | Gastric irritation, optic neuropathy |
INH is the single most effective drug. INH and rifampin can be given parenterally; all others only orally/NG tube.
TBM-Specific Treatment
- Same 4-drug regimen (HRZE) for first 2 months
- Total duration: 9-12 months
- Alternative: INH + PZA + high-dose rifampin + moxifloxacin
- Adjunctive dexamethasone (IV 0.4 mg/kg/day with tapering) reduces mortality from 41% to 32% (RCT, Thwaites et al, Vietnam) - WHO recommends dexamethasone or prednisolone tapered over 6-8 weeks
- Note: A recent placebo-controlled study showed no benefit in PLWH (people living with HIV)
- For intracranial tuberculoma: same regimen; surgical excision if mass effect persists or if no radiological response
- For Pott disease with cord compression: surgical exploration + triple-drug therapy
GI TB Treatment
Same standard 4-drug 6-month regimen. Start immediately if clinical picture is compatible + positive AFB stain or caseating granulomas on histology (don't wait for culture results). In untreated HIV-infected patients, disease progresses rapidly and is invariably fatal.
V. DIAGNOSIS SUMMARY
| Test | Pulmonary TB | Abdominal/Peritoneal TB | TBM |
|---|---|---|---|
| TST/IGRA | Positive in active disease | Positive | Positive |
| Smear (AFB) | Positive or negative | Rarely positive (ascitic fluid ~3%) | Rarely positive (CSF) |
| Culture | Gold standard | ~50% ascitic fluid; best with laparoscopic biopsy | Up to 80% CSF |
| Xpert MTB/RIF | Preferred initial test | Equivocal for pericardial/peritoneal | Sensitivity up to 80%; preferred initial test |
| ADA | Pleural fluid (high sensitivity) | Ascitic fluid ≥39 IU/L (sensitivity 100%, specificity 97%) | CSF ADA elevated |
| Imaging | CXR: cavitation, upper lobe; CT: miliary | CT: LAD, omental thickening, ascites | CT/MRI: basal enhancement, hydrocephalus, infarction |
| Laparoscopy/Biopsy | - | Best diagnostic test for peritoneal TB | LP is cornerstone |
VI. OTHER EXTRAPULMONARY MANIFESTATIONS (Brief)
- Osteoarticular TB (Pott disease): Lower thoracic/upper lumbar vertebral involvement; starts in subchondral anterior vertebral body; involves two adjacent vertebrae + intervertebral disc; paravertebral abscesses; gibbus deformity; spinal cord compression
- Pericardial TB: Exudative pericardial effusion (serosanguineous); ADA sensitivity 87%, specificity 89%; chronic constrictive pericarditis in 30-60%
- Immunologic manifestations: Erythema nodosum, erythema induratum (tuberculids); Poncet disease (reactive arthritis + erythema nodosum); TB-IRIS (5-50% of patients starting ART)
- Genitourinary TB: Presents as sterile pyuria; dysuria, hematuria
- Lymphadenitis: Most common site of EPTB
Sources:
- Goldman-Cecil Medicine, 26th ed. - Chapters 299 (Pulmonary TB, Intestinal TB, Peritoneal TB)
- Adams & Victor's Principles of Neurology, 12th ed. - Chapter 31 (Tuberculous Meningitis, Tuberculoma)
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Extrapulmonary TB, TBM, CSF findings
- Murray & Nadel's Textbook of Respiratory Medicine - TB pleuritis, peritoneal TB, pericardial TB
- Yamada's Textbook of Gastroenterology, 7th ed. - GI TB epidemiology, differential diagnosis, treatment
- ROSEN's Emergency Medicine - CNS TB, GI disease clinical features
Search for latest WHO TB treatment guidelines and drug-resistant TB protocols
Searching the Web
WHO tuberculosis treatment guidelines 2024 2025 update drug resistant
Searching PubMed
"tuberculosis" AND "treatment guidelines" AND "drug resistant"
Searching the Web
WHO DR-TB MDR-TB XDR-TB BPaLM regimen 2025 guidelines update
Reading Web Page
WHO MDR-TB XDR-TB BPaLM BPaL treatment regimen 2025 guidelines
Searching PubMed
"tuberculosis" AND "BPaLM" OR "bedaquiline pretomanid linezolid"
Reading Web Page
ATS CDC ERS IDSA 2025 tuberculosis treatment guidelines drug susceptible drug resistant
Reading Article
Reading Article
Searching the Web
WHO 2025 consolidated TB guidelines Module 4 drug susceptible 4-month regimen rifapentine moxifloxacin
I now have rich, current data from WHO 2025, ATS/CDC/ERS/IDSA 2025, and the pivotal trials. Let me compile the full answer.
WHO TB Treatment Guidelines: 2025 Updates
This covers the WHO Consolidated Guidelines on Tuberculosis, Module 4 (2025) and the parallel ATS/CDC/ERS/IDSA 2025 update - the most significant revision in a decade, driven by multiple phase 3 trials that have fundamentally shortened treatment across both drug-susceptible and drug-resistant TB.
PART 1: DRUG-SUSCEPTIBLE TB (DS-TB)
Standard Regimen (Still Valid)
The classic 6-month regimen remains the backbone and is still the preferred option for certain groups:
| Phase | Duration | Drugs | Notation |
|---|---|---|---|
| Intensive | 2 months | Isoniazid + Rifampin + Pyrazinamide + Ethambutol | 2HRZE |
| Continuation | 4 months | Isoniazid + Rifampin | 4HR |
Preferred for: PLHIV with CD4 <100 cells/mm³, children <12 years, pregnant/breastfeeding women.
NEW: 4-Month Regimen (2025 WHO + ATS/CDC/ERS/IDSA Update)
This is the landmark new option based on the TBTC Study 31/ACTG A5349 phase 3 trial (Dorman et al., NEJM 2021):
| Phase | Duration | Drugs | Notation |
|---|---|---|---|
| Intensive | 2 months | Isoniazid + Rifapentine + Moxifloxacin + Pyrazinamide | 2HPMZ |
| Continuation | 2 months | Isoniazid + Rifapentine + Moxifloxacin | 2HPM |
Key changes vs. standard:
- Ethambutol replaced by Moxifloxacin (fluoroquinolone backbone)
- Rifampin replaced by Rifapentine (longer half-life, more potent rifamycin)
- Total duration: 4 months vs. 6 months
Dosing (fixed):
- Rifapentine: 1200 mg daily (7 days/week)
- Moxifloxacin: 400 mg daily
Trial evidence:
- Non-inferiority demonstrated vs. 2HRZE/4HR in adults and adolescents ≥12 years
- Cure rate 84.5%, retention 99.7%, all-cause mortality 0.4% at end of treatment
- Grade 3+ adverse events: 18.8% (4-month arm) vs. 19.3% (6-month arm) - similar safety
Eligible patients (ATS/CDC/ERS/IDSA 2025):
- Adults and adolescents ≥12 years
- Smear and culture-positive pulmonary DS-TB
NOT eligible for 4-month regimen:
- PLHIV with CD4 <100 cells/mm³ (6-month preferred)
- Children <12 years
- Pregnant, breastfeeding, or postpartum women
- Those who fail eligibility criteria for the pivotal trials
Note: A 2025 commentary in AJRCCM (Wilson et al., Mayo Clinic) urges caution in broad adoption of the 4-month regimen pending real-world evidence outside controlled trial settings.
PART 2: DRUG-RESISTANT TB (DR-TB) - 2025 WHO Guidelines
Definitions
| Classification | Resistance Pattern |
|---|---|
| Isoniazid-resistant TB (Hr-TB) | Isoniazid-resistant, rifampicin-susceptible |
| RR-TB | Rifampicin-resistant (any pattern) |
| MDR-TB | Resistant to both isoniazid + rifampicin |
| Pre-XDR-TB | MDR/RR-TB + resistance to any fluoroquinolone |
| XDR-TB | MDR/RR-TB + resistance to any fluoroquinolone + ≥1 of bedaquiline or linezolid |
Three Tiers of DR-TB Regimens (WHO 2025)
Tier 1 - Preferred: 6-Month All-Oral Regimens
For MDR/RR-TB (fluoroquinolone-susceptible) - Two options:
| Regimen | Drugs | Duration |
|---|---|---|
| BPaLM | Bedaquiline + Pretomanid + Linezolid + Moxifloxacin | 6 months |
| BDLLfx (NEW in 2025) | Bedaquiline + Delamanid + Linezolid + Levofloxacin + Clofazimine | 6 months |
The BDLLfx (also written BDLLfxC) regimen was added in 2025 based on evidence from the BEAT-TB and endTB clinical trials.
For pre-XDR-TB (fluoroquinolone-resistant) - Two options:
| Regimen | Drugs | Duration |
|---|---|---|
| BPaL | Bedaquiline + Pretomanid + Linezolid | 6 months |
| BDLC | Bedaquiline + Delamanid + Linezolid + Clofazimine | 6 months |
Extension to 9 months is permitted for severe/extensive disease or immunosuppression.
BPaLM Evidence - TB-PRACTECAL Trial (Lancet Respir Med, 2024, PMID 37980911)
This phase 2B-3 non-inferiority RCT (7 sites, Uzbekistan/Belarus/South Africa) directly established BPaLM superiority:
- Unfavorable outcomes: BPaLM 12% vs. standard care 41% (risk difference -29.2%, p<0.0001)
- Grade 3+ or serious adverse events: 23% vs. 48% (risk difference -25.2%)
- Deaths: 0 in BPaLM vs. 5 in standard care group
- Conclusion: BPaLM is both more effective and safer than standard of care
BPaLM Systematic Review (Silva et al., J Bras Pneumol, 2025, PMID 39813501)
- BPaLM reduced risk of unfavorable composite outcome (NNT = 7)
- Reduced early treatment discontinuation (NNT = 8)
- Reduced serious adverse events (NNT = 5)
- Better safety profile than standard of care
Tier 2: 9-Month All-Oral Short Regimens
For MDR/RR-TB when fluoroquinolone resistance is excluded. Modified 9-month regimens endorsed in 2025. As of end of 2024, 99 countries were using 9-month regimens.
Tier 3 - Last Resort: 18-20 Month Individualized Regimens
For XDR-TB or when bedaquiline/linezolid intolerance prevents use of shorter regimens. May include injectable agents (amikacin). Individualized combination therapy guided by drug susceptibility testing.
Drug Key (Abbreviations)
| Letter | Drug |
|---|---|
| B | Bedaquiline |
| Pa | Pretomanid |
| L | Linezolid |
| M | Moxifloxacin |
| D | Delamanid |
| Lfx | Levofloxacin |
| C | Clofazimine |
| H | Isoniazid |
| R | Rifampicin |
| Z | Pyrazinamide |
| E | Ethambutol |
| P | Rifapentine |
Isoniazid-Resistant TB (Hr-TB)
WHO recommends: 6RZES (rifampin + pyrazinamide + ethambutol + streptomycin) or 6RZE - without isoniazid. Fluoroquinolone-containing regimens are an alternative.
PART 3: SPECIAL SITUATIONS
TB-HIV Coinfection
- Start ART in all TB patients regardless of CD4 count (expanded 2025 recommendation)
- Preferred DS-TB regimen in PLHIV with CD4 <100 cells/mm³: 6-month 2HRZE/4HR
- The 4-month rifapentine-moxifloxacin regimen has been studied in PLHIV but the 6-month regimen is still preferred at very low CD4 counts
- For TBM in PLHIV: a recent placebo-controlled trial showed no survival benefit from adjunctive dexamethasone (unlike non-HIV patients)
- TB-IRIS: Occurs in 5-50% starting ART; high morbidity when CNS involvement
TB in Pregnancy
- 4-month rifapentine-moxifloxacin regimen is NOT recommended (women excluded from S31/A5349 trial)
- Standard 6-month 2HRZE/4HR is used
- Avoid: Pyrazinamide in first trimester per some guidelines; streptomycin (ototoxic to fetus); fluoroquinolones (teratogenic concern)
TB Meningitis
- 4-drug regimen (HRZE) for 2 months, then HR to complete 9-12 months total
- Adjunctive dexamethasone IV (0.4 mg/kg/day tapering over 6-8 weeks) - WHO-recommended for non-HIV TBM patients; reduces mortality
- Drugs with best CNS penetration: INH > PZA > rifampin > ethambutol
PART 4: NEW WHO 2025 MODULE 6 - TB AND UNDERNUTRITION (October 2025)
- Nutritional assessment and counselling for ALL people with TB and their household contacts (formal recommendation for the first time)
- Nutritional interventions for TB patients with undernutrition regardless of age, drug resistance status, pregnancy, or severity
- Food assistance to prevent TB in household contacts in food-insecure settings (based on RATIONS trial)
REAL-WORLD ADOPTION (WHO Global TB Report 2025)
| Year | Countries using 6-month MDR/RR-TB regimens | People started on 6-month regimens |
|---|---|---|
| 2022 | 41 | 1,744 |
| 2023 | 60 | 5,653 |
| 2024 | 97 | 34,256 |
This ~6x increase from 2023 to 2024 reflects rapid scale-up of BPaLM globally after WHO endorsement.
SUMMARY COMPARISON TABLE
| Feature | DS-TB (Standard) | DS-TB (New) | MDR/RR-TB (Preferred) | Pre-XDR/XDR-TB |
|---|---|---|---|---|
| Duration | 6 months | 4 months | 6 months | 6-9 months (individualized 18-20 months for XDR) |
| Key drugs | HRZE / HR | HPMZ / HPM | BPaLM or BDLLfx | BPaL or BDLC |
| Route | Oral | Oral | All-oral | All-oral (injectable as last resort) |
| Guideline year | Classic | 2025 | 2022-2025 | 2025 |
Key references:
- WHO Global TB Report 2025 - DR-TB Treatment
- TB-PRACTECAL trial (Lancet Respir Med, 2024) - PMID 37980911
- BPaLM systematic review (J Bras Pneumol, 2025) - PMID 39813501
- ATS/CDC/ERS/IDSA 2025 clinical practice update (February 2025) - endorsing 4-month DS-TB regimen for eligible patients
- WHO Module 6: TB and Undernutrition (October 2025)
The full video walkthrough of the ATS/CDC/ERS/IDSA 2025 update is available here:
arrange all this material in on single pdf including treatment
Reading File
Running Command
Running Command
Running Command
Writing File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.