Tumour markers
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Now I have comprehensive information. Let me compile the full response.
Tumour Markers
Definition
Tumour markers are substances present in abnormally high concentrations in body fluids or tissue from patients with cancer. They are surrogate indicators that can help confirm a cancer diagnosis, monitor treatment effectiveness, estimate prognosis, and/or predict whether a specific therapy is likely to be effective. They may be tumour-derived or tumour-associated, and include a wide variety of molecular species: proteins, hormones, enzymes, glycoproteins, mucins, and molecular/genomic markers.
- Tietz Textbook of Laboratory Medicine, 7th Ed, p. 1011
Types of Serum Tumour Markers
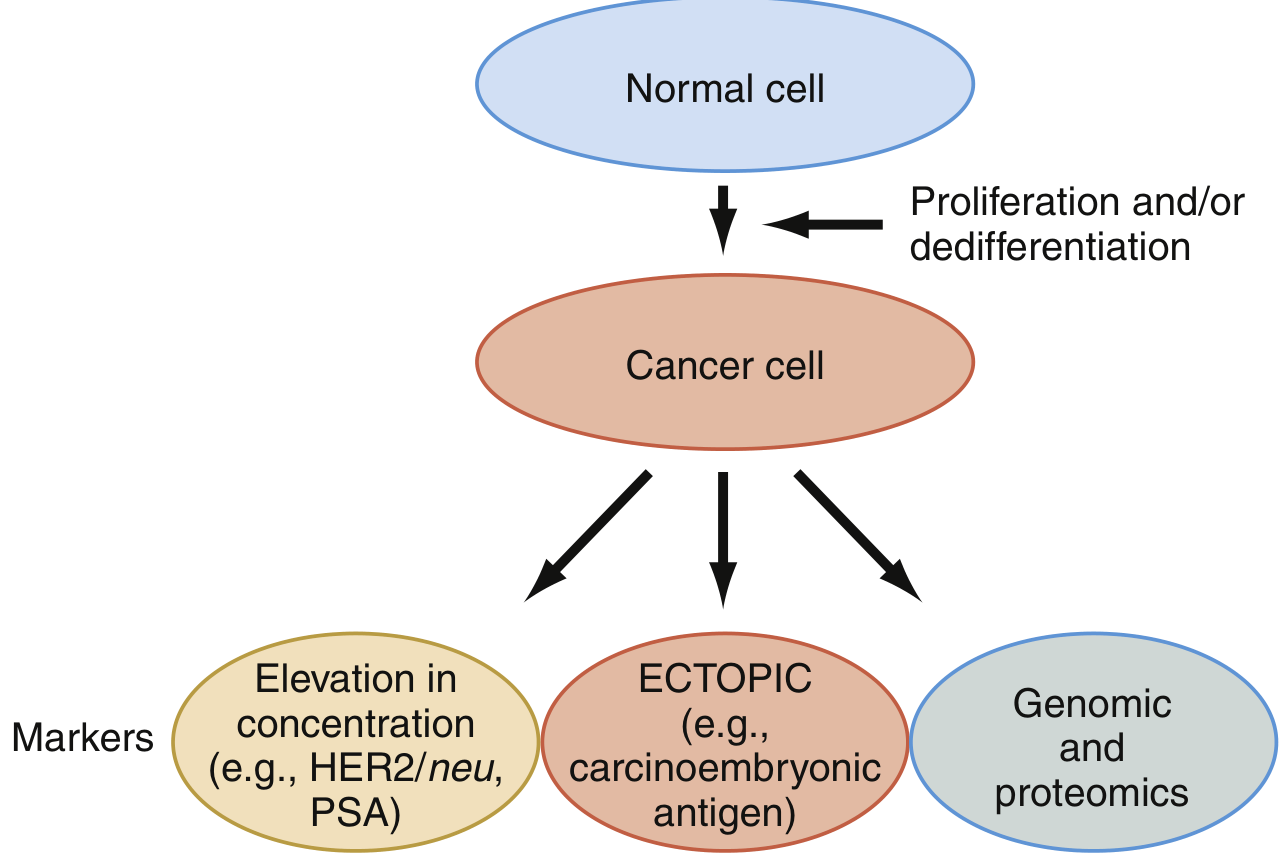
Three functional categories of tumour markers are commonly recognised (Henry's Clinical Diagnosis and Management):
1. Oncofetal Antigens
Normally expressed during fetal development but re-expressed in malignant cells:
- AFP (alpha-fetoprotein) - hepatocellular carcinoma, germ cell tumours
- CEA (carcinoembryonic antigen) - colorectal cancer (most widely used GI marker)
- beta-hCG (human chorionic gonadotropin) - germ cell/testicular tumours, gestational trophoblastic neoplasia
2. Mucin/Glycoprotein CA Antigens (Monoclonal Antibody-Defined)
| Marker | Major Malignancy |
|---|---|
| CA 125 | Ovarian carcinoma |
| CA 19-9 | Pancreatic carcinoma |
| CA 15-3 | Breast carcinoma |
| CA 72-4 | Gastric carcinoma |
| HER2/neu | Breast carcinoma |
3. Polypeptide Hormones and Enzymes
- PSA (prostate-specific antigen) - prostate cancer; organ-specific but not cancer-specific (elevated in BPH and prostatitis too)
- Calcitonin - medullary carcinoma of the thyroid; ectopically in bronchogenic carcinoma
- LDH (lactate dehydrogenase) - testicular cancer staging/prognosis
- Chromogranin A - pheochromocytoma, medullary thyroid carcinoma, small cell lung carcinoma, pancreatic neuroendocrine tumours
- Thyroglobulin - papillary and follicular thyroid cancer (post-thyroidectomy monitoring)
- CYFRA 21-1 - cytokeratin 19 fragment; useful in squamous cell lung carcinoma
Clinical Applications
1. Screening
Only PSA has widespread application in screening (prostate cancer). Most markers have insufficient sensitivity/specificity for population screening. The UK does not routinely screen with PSA, but men can request testing.
2. Diagnosis
Tumour marker results rarely replace biopsy for primary diagnosis. A raised result never definitively indicates malignancy; a normal result never excludes it. Use is recommended only when clinical presentation raises specific cancer suspicion.
3. Prognosis and Risk Stratification
- PSA stratifies men with newly diagnosed prostate cancer into risk groups
- AFP, beta-hCG, LDH contribute to the International Germ Cell Cancer Collaborative Group (IGCCCG) prognostic classification for testicular cancer
- ER, PR, HER2/neu are mandatory prognostic and predictive markers in breast cancer on surgical specimens
4. Treatment Prediction
- ER (oestrogen receptor): Positive = likely benefit from antiestrogen therapy (tamoxifen, aromatase inhibitors). Negative = unlikely to benefit
- HER2/neu overexpression: Predicts response to trastuzumab (Herceptin); associated with poor prognosis
5. Monitoring Therapy and Detecting Recurrence
This is the most validated use of tumour markers, particularly for:
- Choriocarcinoma (beta-hCG, AFP) - mandatory
- Germ cell tumours (AFP, beta-hCG, LDH)
- Colorectal cancer (CEA) - post-surgical surveillance
- Ovarian cancer (CA 125)
- Prostate cancer (PSA after treatment)
Clinical Presentations and Markers
| Marker | Primary Cancer | Typical Presentation | Also Raised In |
|---|---|---|---|
| AFP | Germ cell tumour; HCC | Testicular swelling; ascites/jaundice | Gastric, colorectal, biliary, pancreatic, lung |
| CA 125 | Ovarian cancer | Pelvic mass; bloating | Breast, endometrial, lung, pancreas |
| CA 19-9 | Pancreatic cancer | Obstructive jaundice, weight loss | Colorectal, gastric, HCC, ovary |
| CEA | Colorectal cancer | Abdominal pain, bleeding, palpable mass | Breast, gastric, lung, mesothelioma |
| hCG | Germ cell tumour; GTN | Testicular swelling; cannonball secondaries on CXR | Lung cancer |
| Paraproteins | Multiple myeloma | Bone pain, anaemia, recurrent infections | - |
| PSA | Prostate cancer | LUTS, acute retention, bone pain | None (organ specific) |
Tietz Textbook of Laboratory Medicine, 7th Ed, Table 33.13
Testicular Cancer Markers (Summary)
AFP, beta-hCG, and LDH are the three routinely used markers for testicular cancer. They provide insight into:
- Likely histological subtype (e.g., AFP not elevated in pure seminoma)
- Success of treatment
- Recurrence
- IGCCCG prognostic categorisation
Bailey and Love's Short Practice of Surgery, 28th Ed
Important Practical Principles
- Pretreatment baseline is essential - always obtain before starting therapy
- Confirm on repeat specimen before making therapy decisions
- Half-life matters - e.g., PSA half-life is ~3-4 days; wait at least 30 days post-surgery before assessing success of prostate cancer resection
- Organ/metabolic disease can falsely elevate markers - CEA rises in liver disease (impaired clearance); beta-2 microglobulin rises in renal failure
- Multiple markers improve sensitivity - tumour heterogeneity means no single marker is 100% sensitive; combining markers can improve detection rates
- Ectopic expression - some markers appear in unexpected cancers at advanced/metastatic stages, often indicating poor prognosis (e.g., AFP in metastatic GI cancer with normal LFTs)
PSA - Key Points
- Glycoprotein produced by prostatic epithelial cells
- Not significantly altered by digital rectal examination (DRE)
- Significantly altered by UTI - returns to baseline 6 weeks after infection treatment
- Artificially lowered (up to 2-fold) by 5-alpha reductase inhibitors (finasteride, dutasteride)
- Also lowered by aspirin, statins, and thiazide diuretics
- No single "normal" threshold - influenced by age, ethnicity, and family history
Bailey and Love's Short Practice of Surgery, 28th Ed, p. 1473
Sources: Tietz Textbook of Laboratory Medicine (7th Ed); Henry's Clinical Diagnosis and Management by Laboratory Methods; Bailey and Love's Short Practice of Surgery (28th Ed); Schwartz's Principles of Surgery (11th Ed).
This is a shared conversation. Sign in to Orris to start your own chat.