I have all the information I need. Now I'll write the complete, well-organized exam answer.
HYPERSENSITIVITY REACTIONS
Classification, Mechanism, Mediators, Examples & Pharmacological Management
[M. Pharm | Immunopharmacology / Pharmacology | 10 Marks Long Answer]
DEFINITION
Hypersensitivity is defined as an exaggerated or augmented immune response to an antigen (allergen) that is harmful to the host. It requires a presensitized state - meaning the individual must first be exposed to the antigen (sensitization), and the harmful response occurs upon second or subsequent exposure to the same antigen.
"Hypersensitivity responses lead to tissue damage: immunopathology. The mechanisms underlying them are the same as those normally employed by the body in combating infection - the problem is they occur with too high an intensity, directed against antigens that pose no threat." - Roitt's Essential Immunology
1. CLASSIFICATION TABLE
Classified by Gell and Coombs (1963)
| Feature | Type I (Immediate) | Type II (Cytotoxic) | Type III (Immune Complex) | Type IV (Delayed/Cell-Mediated) |
|---|
| Other Name | Anaphylactic / Atopic | Antibody-Dependent Cytotoxic | Immune Complex-Mediated | Delayed-Type Hypersensitivity (DTH) |
| Immunoglobulin | IgE | IgG, IgM | IgG, IgM | None (T-cell mediated) |
| Effector Mechanism | Mast cell degranulation | Complement + ADCC | Complement activation + neutrophil recruitment | T-lymphocytes + Macrophages |
| Onset Time | Seconds to minutes | Minutes to hours | 6-12 hours | 48-72 hours |
| Key Cells | Mast cells, Basophils, Eosinophils | NK cells, Macrophages, Neutrophils | Neutrophils, Macrophages | CD4+ Th1 cells, CD8+ T cells, Macrophages |
| Complement | Not involved | Involved | Involved | Not involved |
| Mediators | Histamine, Leukotrienes, Prostaglandins | Complement fragments (C3b, MAC) | C5a, C3a, Lysosomal enzymes | IFN-γ, IL-2, TNF-β |
| Example | Anaphylaxis, Asthma, Hay fever | Hemolytic anemia, ABO transfusion reaction | SLE, Post-streptococcal GN, Serum sickness | Contact dermatitis, Tuberculin test, Graft rejection |
2. MECHANISM OF EACH TYPE
Type I - Immediate (IgE-Mediated) Hypersensitivity
Step-by-step mechanism:
Phase 1 - Sensitization:
- Allergen (e.g., pollen, penicillin) enters the body for the first time
- Antigen-presenting cells (APCs) present the antigen to Th2 cells
- Th2 cells release IL-4 and IL-13, which stimulate B cells to switch to IgE production
- IgE antibodies bind by their Fc portion to high-affinity FcεRI receptors on mast cells and basophils
- Patient is now sensitized (no symptoms yet)
Phase 2 - Elicitation (on re-exposure):
- Same allergen enters again and cross-links two or more IgE molecules on the surface of mast cells
- This cross-linking triggers mast cell degranulation
- Preformed mediators (histamine, tryptase) are released immediately
- Newly synthesized mediators (leukotrienes, prostaglandins) are formed from arachidonic acid within minutes
Type II - Cytotoxic (Antibody-Dependent) Hypersensitivity
Mechanism:
- IgG or IgM antibodies are directed against cell-surface antigens or antigens on extracellular matrix
- Antibody binding activates complement via classical pathway, producing MAC (membrane attack complex) → cell lysis
- Cells coated with IgG are also destroyed by:
- ADCC (Antibody-Dependent Cellular Cytotoxicity): NK cells and macrophages with FcγR bind and kill the target cell
- Opsonization: C3b-coated cells are phagocytosed by macrophages
- Drugs (e.g., penicillin) can haptenize red blood cells, triggering antibody formation against drug-RBC complex → hemolysis
- In some cases (e.g., Graves' disease), antibodies to cell-surface receptors stimulate or block function without causing lysis - sometimes called Type V
Type III - Immune Complex-Mediated Hypersensitivity
Mechanism:
- Antigen-antibody (IgG/IgM) complexes form in excess in circulation
- Normally, immune complexes are cleared by phagocytes, but when they persist, they deposit in tissues (glomeruli, joints, blood vessel walls)
- Deposited immune complexes activate complement → C3a and C5a (anaphylatoxins)
- C5a is a potent chemoattractant, recruiting neutrophils to the site
- Neutrophils release lysosomal enzymes and reactive oxygen species → tissue damage and inflammation
- Leads to vasculitis, nephritis, arthritis
Two subtypes:
- Arthus reaction (local): IgG + injected antigen → local complement activation (12 hours)
- Serum sickness (systemic): Large antigen excess → systemic immune complex deposition (6-12 hours)
Type IV - Delayed-Type (Cell-Mediated) Hypersensitivity
Mechanism:
- No antibody involved - purely T-cell mediated
- On first exposure, antigen is processed by APCs (Langerhans cells in skin) and presented to CD4+ Th1 cells via MHC Class II
- Th1 cells become sensitized and memory T cells form
- On re-exposure (48-72 hours later), antigen is re-presented to sensitized T cells
- Activated Th1 cells release cytokines: IFN-γ, IL-2, TNF-β
- IFN-γ activates macrophages, which release more TNF and lysosomal enzymes
- Results in granuloma formation, tissue induration, and necrosis
Subtypes of Type IV:
- Contact hypersensitivity - chemicals (nickel, urushiol from poison ivy) act as haptens
- Tuberculin-type - tuberculin test (positive = induration in 24-72 hrs)
- Granulomatous - chronic macrophage activation (e.g., tuberculosis, leprosy)
3. MEDIATORS TABLE
| Type | Preformed Mediators | Newly Formed / Secondary Mediators |
|---|
| Type I | Histamine, Tryptase, Heparin, Eosinophil Chemotactic Factor | Leukotrienes (LTC4, LTD4, LTE4), Prostaglandins (PGD2), PAF, TNF-α, IL-4 |
| Type II | - | Complement fragments (C3b, C5a, MAC), Perforin/Granzymes (ADCC) |
| Type III | - | C3a, C5a (anaphylatoxins), Lysosomal enzymes, Reactive oxygen species |
| Type IV | - | IFN-γ, IL-2, TNF-β, IL-17, Macrophage activating factor (MAF) |
4. EXAMPLES (DISEASE-WISE)
| Disease | Type |
|---|
| Anaphylaxis (bee sting, penicillin) | Type I |
| Bronchial Asthma | Type I |
| Hay Fever (Allergic Rhinitis) | Type I |
| Atopic Dermatitis (Eczema) | Type I |
| Hemolytic Transfusion Reaction (ABO mismatch) | Type II |
| Rh hemolytic disease of newborn | Type II |
| Autoimmune Hemolytic Anemia | Type II |
| Goodpasture Syndrome | Type II |
| Graves' Disease (TSH receptor antibody) | Type II (V) |
| Myasthenia Gravis (AChR antibody) | Type II (V) |
| Systemic Lupus Erythematosus (SLE) | Type III |
| Post-streptococcal Glomerulonephritis | Type III |
| Serum Sickness | Type III |
| Arthus Reaction | Type III |
| Contact Dermatitis (poison ivy, nickel) | Type IV |
| Tuberculin (Mantoux) Test | Type IV |
| Graft Rejection (allograft) | Type IV |
| Leprosy (tuberculoid), TB | Type IV |
5. PHARMACOLOGICAL MANAGEMENT
Type I Hypersensitivity - Management
| Drug Class | Drug Name | Mechanism of Action | Clinical Use |
|---|
| First-line (Anaphylaxis) | Epinephrine (Adrenaline) | Activates α1 (vasoconstriction) and β2 (bronchodilation) receptors; reverses bronchoconstriction and hypotension | Severe anaphylaxis - IM injection |
| H1 Antihistamines | Diphenhydramine, Cetirizine, Loratadine | Competitive block of H1 receptors; reduces vasodilation, pruritus, urticaria | Allergic rhinitis, urticaria, mild allergy |
| Corticosteroids | Prednisolone, Dexamethasone, Hydrocortisone | Inhibit phospholipase A2 → block arachidonic acid cascade → reduces leukotrienes + prostaglandins; suppress cytokine production | Severe allergy, asthma, late-phase reaction |
| Leukotriene Receptor Antagonists (LTRA) | Montelukast, Zafirlukast | Block cysteinyl leukotriene (CysLT1) receptors → reduce bronchoconstriction and mucus secretion | Bronchial asthma, allergic rhinitis |
| Mast Cell Stabilizers | Sodium Cromoglycate, Nedocromil | Prevent mast cell degranulation by blocking chloride channels → inhibit release of histamine and other mediators | Prophylaxis in asthma, allergic rhinitis |
| β2-Agonists | Salbutamol, Formoterol | Bronchodilation by activating β2 receptors on bronchial smooth muscle | Acute asthma attack |
| Xanthines | Theophylline | Inhibit phosphodiesterase → increase cAMP → bronchodilation + mast cell stabilization | Chronic asthma |
| Monoclonal Antibody | Omalizumab (anti-IgE) | Binds free IgE → prevents IgE binding to FcεRI on mast cells → no degranulation | Severe allergic asthma, chronic urticaria |
| Immunotherapy | Allergen desensitization | Repeated low-dose allergen exposure shifts Th2 → Th1, increases IgG4 (blocking antibody), reduces IgE | Long-term allergy treatment |
Type II Hypersensitivity - Management
| Drug / Approach | Mechanism |
|---|
| Corticosteroids (Prednisolone) | Suppress antibody production and complement activation |
| Plasma exchange (Plasmapheresis) | Removes circulating autoantibodies and immune complexes |
| IVIG (Intravenous Immunoglobulin) | Saturates FcRn receptors → faster degradation of pathogenic IgG |
| Rituximab (anti-CD20) | Depletes B cells → reduces antibody production |
| Supportive: Blood transfusion for hemolytic anemia | Replace destroyed RBCs |
Type III Hypersensitivity - Management
| Drug / Approach | Mechanism |
|---|
| Corticosteroids | Suppress inflammation, inhibit complement activation and neutrophil function |
| NSAIDs | Relieve joint pain and inflammation (COX inhibition) |
| Plasmapheresis | Remove immune complexes from circulation |
| Hydroxychloroquine (in SLE) | Inhibits Toll-like receptor signaling → reduces immune complex deposition |
| Immunosuppressants (Azathioprine, Cyclophosphamide, Mycophenolate) | Reduce B and T cell activity; first-line in SLE nephritis |
| Anti-TNF agents (in vasculitis) | Block TNF-mediated inflammation |
| Antigen removal | Treat underlying infection (e.g., antibiotics for post-streptococcal GN) |
Type IV Hypersensitivity - Management
| Drug / Approach | Mechanism |
|---|
| Corticosteroids (topical + systemic) | Suppress T-cell activation; reduce cytokine release and macrophage activation - first-line for contact dermatitis |
| Calcineurin Inhibitors (Tacrolimus, Cyclosporine) | Block calcineurin → inhibit IL-2 transcription → suppress T-cell proliferation; used in contact dermatitis and organ transplant rejection |
| Anti-TNF biologics (Infliximab, Adalimumab) | Block TNF-α → reduce macrophage activation and granuloma formation |
| Dapsone | Anti-inflammatory; used in leprosy (Type IV component) |
| Antituberculosis drugs | Treat the cause of Type IV granuloma in TB |
| Avoidance of antigen | Fundamental approach in contact hypersensitivity |
6. TYPE I HYPERSENSITIVITY - FLOWCHART
┌─────────────────────────────────────────────────────────┐
│ TYPE I HYPERSENSITIVITY FLOWCHART │
│ (IgE-Mediated / Immediate Type) │
└─────────────────────────────────────────────────────────┘
┌──────────────────────────────────────┐
│ FIRST EXPOSURE TO ALLERGEN │
│ (Pollen, Dust mite, Penicillin, Food) │
└────────────────┬─────────────────────┘
│
▼
┌──────────────────────────────────┐
│ Allergen → APCs present to │
│ Th2 cells │
└─────────────────┬────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ Th2 cells secrete IL-4 and IL-13 │
│ → B cells undergo class switching │
│ → B cells produce IgE antibodies │
└──────────────────┬──────────────────────┘
│
▼
┌────────────────────────────────────────────┐
│ IgE binds to FcεRI receptors on │
│ MAST CELLS and BASOPHILS │
│ (Patient is now SENSITIZED - no symptoms) │
└─────────────────┬──────────────────────────┘
│
═══════════════════════════════════
SECOND EXPOSURE TO ALLERGEN
═══════════════════════════════════
│
▼
┌────────────────────────────────────────────┐
│ Allergen CROSS-LINKS two IgE molecules │
│ on the surface of mast cells │
└──────────────────┬─────────────────────────┘
│
▼
┌──────────────────────────────────────────────────┐
│ MAST CELL DEGRANULATION │
└─────────────┬──────────────────┬─────────────────┘
│ │
┌─────────▼──────┐ ┌───────▼──────────────┐
│ PREFORMED │ │ NEWLY FORMED │
│ MEDIATORS │ │ MEDIATORS │
│ (Released │ │ (Synthesized from │
│ immediately) │ │ Arachidonic acid) │
│ │ │ │
│ • Histamine │ │ • Leukotrienes │
│ • Tryptase │ │ (LTC4, LTD4, LTE4) │
│ • Heparin │ │ • Prostaglandin D2 │
│ • ECF-A │ │ • PAF │
│ (Eosinophil │ │ • TNF-α, IL-4 │
│ Chemo Factor) │ │ │
└──────┬─────────┘ └───────┬───────────────┘
│ │
└──────────┬──────────┘
▼
┌─────────────────────────────────────────────────────┐
│ CLINICAL EFFECTS │
├─────────────────────────────────────────────────────┤
│ Histamine → Vasodilation, Edema, Bronchospasm, │
│ Pruritus, Urticaria │
│ Leukotrienes → Bronchoconstriction, Mucus↑ │
│ PGD2 → Vasodilation, Bronchospasm │
│ PAF → Platelet aggregation, Bronchospasm │
└───────────────────┬─────────────────────────────────┘
│
┌─────────────┴──────────────┐
▼ ▼
┌──────────────────────┐ ┌───────────────────────────┐
│ LOCAL REACTION │ │ SYSTEMIC REACTION │
│ (Atopy) │ │ (Anaphylaxis) │
│ │ │ │
│ • Hay fever │ │ • Hypotension │
│ • Asthma │ │ • Laryngeal edema │
│ • Urticaria │ │ • Bronchospasm │
│ • Eczema │ │ • Cardiovascular collapse │
│ • Food allergy │ │ • Can be FATAL │
└───────────────────────┘ └───────────────────────────┘
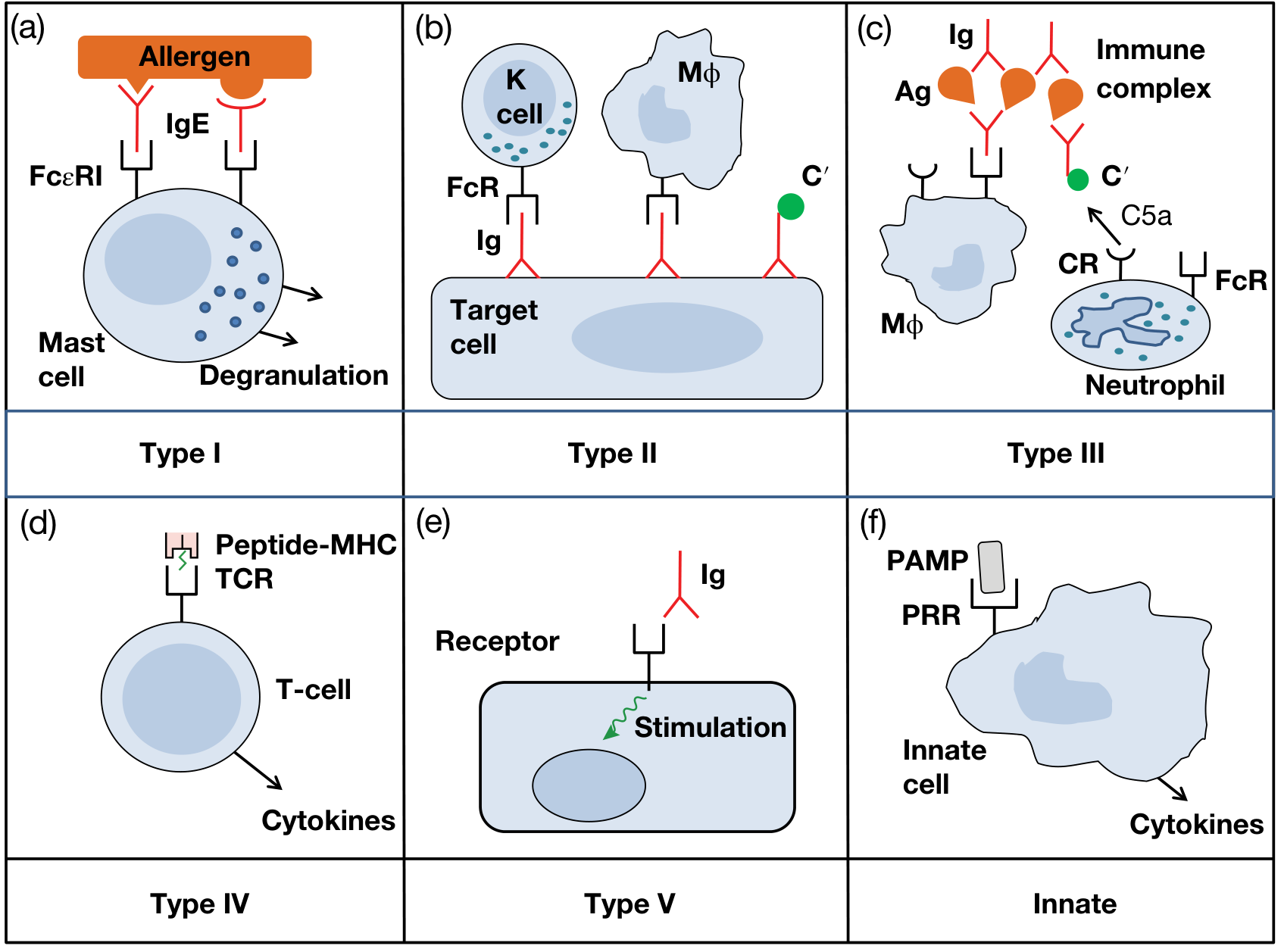
Visual reference from Roitt's Essential Immunology (6 types of hypersensitivity):
Figure: The Gell and Coombs Classification - Types I to IV (+ Type V and Innate). Source: Roitt's Essential Immunology, 13th Edition.
DIFFERENTIATION TABLE (Quick Comparison for Exam)
| Parameter | Type I | Type II | Type III | Type IV |
|---|
| Antibody | IgE | IgG/IgM | IgG/IgM | None |
| Complement | No | Yes | Yes | No |
| Cells involved | Mast cell, Basophil | NK cell, Macrophage | Neutrophil | T-cell, Macrophage |
| Onset | Seconds - minutes | Minutes | 6-12 hours | 48-72 hours |
| Passive transfer possible by | Serum (IgE) | Serum (IgG) | Serum (IgG) | Cells (T cells) |
| Skin test reaction | Wheal and flare (immediate) | - | Arthus (6 hrs) | Induration (48-72 hrs) |
| Characteristic disease | Anaphylaxis | Hemolytic anemia | SLE | Contact dermatitis |
| Histopathology | Mast cell degranulation | Cell lysis, opsonization | Neutrophilic infiltrate | Mononuclear infiltrate, granuloma |
CONCLUSION
Hypersensitivity reactions represent a spectrum of immune-mediated tissue damage with distinct mechanisms, mediators, and clinical presentations - their understanding is clinically indispensable for the rational selection of pharmacological agents, from epinephrine in anaphylaxis to calcineurin inhibitors in delayed-type hypersensitivity, and forms the immunological basis for treating allergic, autoimmune, and inflammatory diseases in clinical practice.
References:
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition - Hypersensitivity (pp. 150-153)
- Roitt's Essential Immunology, 13th Edition - Chapter 14: Allergy and Other Hypersensitivities
- Janeway's Immunobiology, 10th Edition - Chapter 14: Allergic Diseases and Hypersensitivity Reactions
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Katzung's Basic and Clinical Pharmacology, 16th Edition