
Rt. Hand 5th metacarpal fracture. Further investigations and line of management
Reading File
analyse_media
Finding Sources
Finding Sources
Searching PubMed
fifth metacarpal base fracture "reverse Bennett" treatment
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Let me compile the complete response.
X-Ray Findings
The AP/oblique hand X-ray shows a Reverse Bennett's fracture - an intra-articular fracture-subluxation at the base of the right 5th metacarpal, with the following features:
- Intra-articular fracture extending into the 5th carpometacarpal (CMC) joint
- Moderate comminution at the articular base with multiple visible fragments
- Significant proximal and radial displacement of the 5th metacarpal shaft, pulled by the extensor carpi ulnaris (ECU) tendon (which inserts at the dorsal base of the 5th metacarpal)
- A small ulnar fragment remains aligned with the hamate, resulting in 5th CMC joint subluxation
- Prominent periarticular soft tissue swelling over the ulnar aspect of the wrist/hand
- Remaining metacarpals and visible phalanges appear intact
Further Investigations
Radiological
- 30-degree pronation oblique view of the hand - gives a better profile of the 5th metacarpal base articular surface for accurate fragment assessment (specifically recommended by Campbell's Operative Orthopaedics)
- True lateral view of the hand/wrist - assess dorsal displacement and CMC subluxation extent
- CT scan of the hand/wrist - recommended when comminution is moderate-to-severe; provides 3D assessment of fragment size, number, and joint congruency, and aids pre-operative planning for ORIF
Clinical
- Neurovascular assessment of the small finger (check ulnar digital nerve and capillary refill)
- Assess for malrotation by having the patient flex fingers toward the scaphoid tubercle - scissoring indicates rotational deformity
- Check for any open wound (fight bite if injury from punching)
- Document grip strength for baseline
Mechanism and Pathoanatomy
This is the ulnar analog of Bennett's fracture of the thumb. The ECU tendon inserts at the dorsal base of the 5th metacarpal and, analogous to the abductor pollicis longus in a Bennett fracture, pulls the metacarpal shaft proximally and radially away from the small hamate fragment. The 5th CMC joint allows ~30 degrees of flexion/extension and contributes to palmar cupping and power grip - loss of articular congruity here leads to painful post-traumatic arthritis and grip weakness if not properly reduced.
Line of Management
Acute (Emergency Department)
- Analgesia - oral NSAIDs + paracetamol; consider haematoma block for manipulation
- Temporary splinting in ulnar gutter splint with wrist in 20-30° extension pending definitive management
- Orthopaedic/Hand Surgery referral - this fracture is inherently unstable and almost always requires operative fixation
Definitive - Operative (Indicated in this case)
Because of the intra-articular nature, significant displacement, comminution, and CMC subluxation, non-operative management is insufficient for this fracture. The two main operative options are:
1. Closed Reduction and Percutaneous Pinning (CRPP) - First-line if adequate reduction achievable
- Traction applied to the small finger under fluoroscopy with the wrist ulnarly deviated
- Direct pressure over the displaced metacarpal base to reduce the CMC subluxation
- 1-2 K-wires (0.045-0.062 inch) placed percutaneously to transfix the 5th metacarpal base to the hamate or 4th metacarpal
- Pin configuration: transverse cross-pinning through the 4th and 5th metacarpal bases is most common
- Post-op: short arm dorsal splint/ulnar gutter cast for 4-6 weeks; pins removed at 4-6 weeks
- Preferred when fracture is reducible and comminution is moderate
2. Open Reduction and Internal Fixation (ORIF) - For irreducible fractures or severe comminution
- Dorsal-ulnar approach over the 5th metacarpal base
- Direct visualization and reduction of articular fragments
- Fixation with mini-fragment screws (1.3 or 1.5 mm lag screws) or a small T/L-plate on the dorsal base
- Allows restoration of joint congruency under direct vision
- Post-op: splinting for 3-4 weeks, then early protected mobilization
- Preferred when CRPP cannot restore articular congruency, or CT shows large displaced fragments
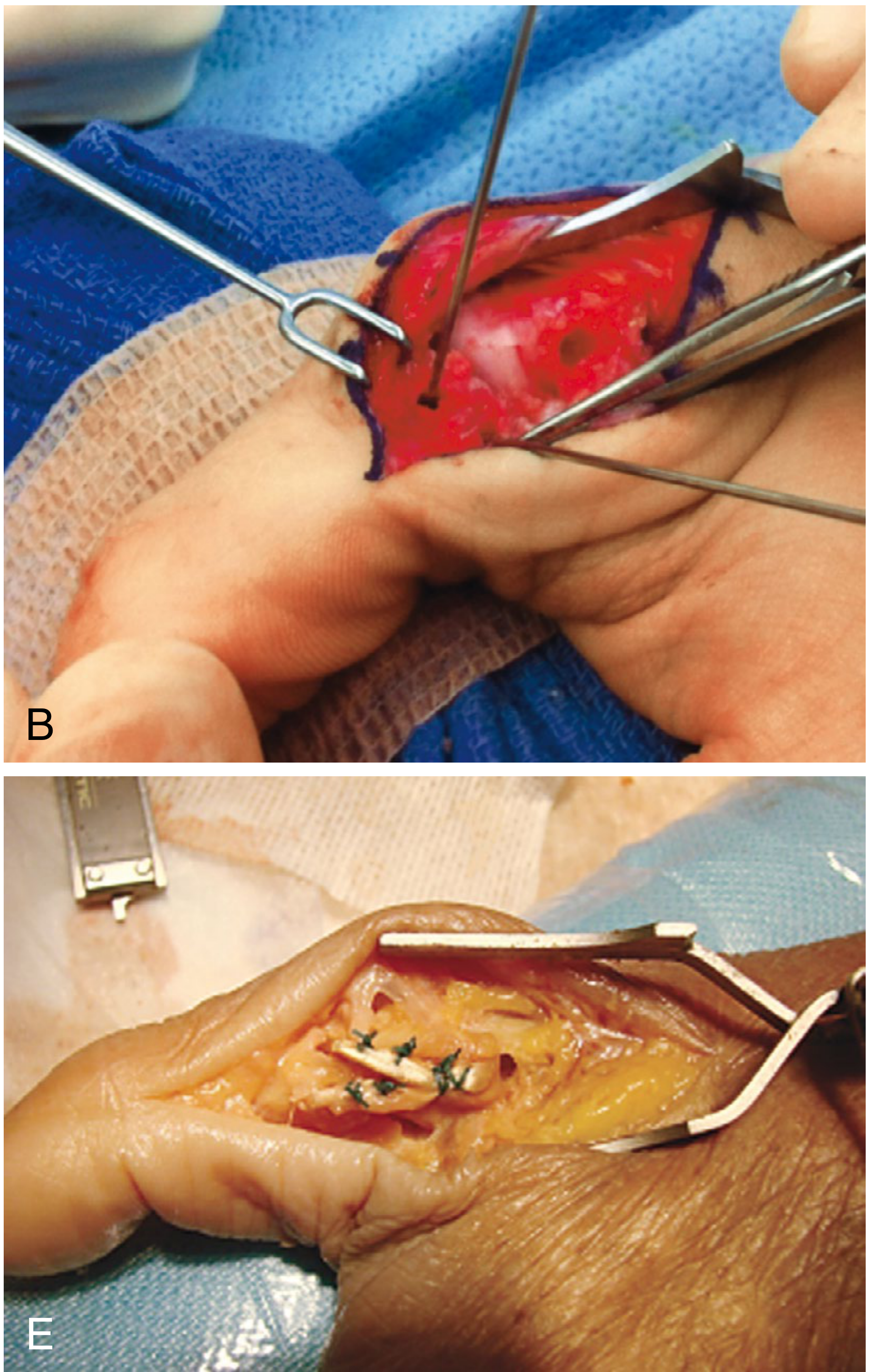
Surgical Technique Note (Campbell's Operative Orthopaedics, 15th Ed)
"This fracture often can be reduced by traction and percutaneous pinning and is then protected by splint immobilization. Fractures that are not recognized early and are healing in a displaced position may benefit from corrective osteotomy of the malunion, resection arthroplasty, or fusion provided that the fracture is symptomatic."
The operative image below shows open reduction of a 5th metacarpal base fracture-subluxation:
Post-Operative Management
| Phase | Timing | Actions |
|---|---|---|
| Immobilization | 0-4 weeks | Ulnar gutter splint or short arm cast; fingers free |
| Pin removal | 4-6 weeks (if CRPP) | Clinical + radiological union assessment |
| Physiotherapy | From week 3-4 | Active ROM exercises of MCP/PIP joints; edema control |
| Strengthening | 6-10 weeks | Progressive grip and pinch strengthening |
| Full activity | 10-12 weeks | Based on radiological union and functional recovery |
Complications to Counsel
- Post-traumatic CMC arthritis (most significant long-term risk if articular reduction is not anatomical)
- Grip weakness and reduced power with palmar cupping
- Stiffness of the small finger MCP joint
- Pin tract infection (if CRPP)
- Malunion / re-displacement (especially if non-operative treatment attempted)
- Neurovascular injury to the dorsal ulnar sensory branch during surgery
Summary: This is a Reverse Bennett's fracture - an unstable intra-articular CMC fracture-subluxation. It requires urgent hand surgery referral. Obtain a 30° pronation oblique view and CT for pre-operative planning. CRPP is first-line if reduction is achievable under fluoroscopy; ORIF is indicated for irreducible or severely comminuted patterns.
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 4115-4116
- Rockwood and Green's Fractures in Adults 10th Ed 2025, pp. 2042-2043
This is a shared conversation. Sign in to Orris to start your own chat.