Brachial plexus and it’s lesions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content and excellent diagrams. Let me compile the full answer.
Brachial Plexus and Its Lesions
Anatomy of the Brachial Plexus
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5, C6, C7, C8, and T1. It originates in the posterior triangle of the neck, passes between the anterior and middle scalene muscles, crosses over rib I, and enters the axilla - where it surrounds the axillary artery.
Fig. 7.52 - Structure of the Brachial Plexus (Gray's Anatomy for Students)

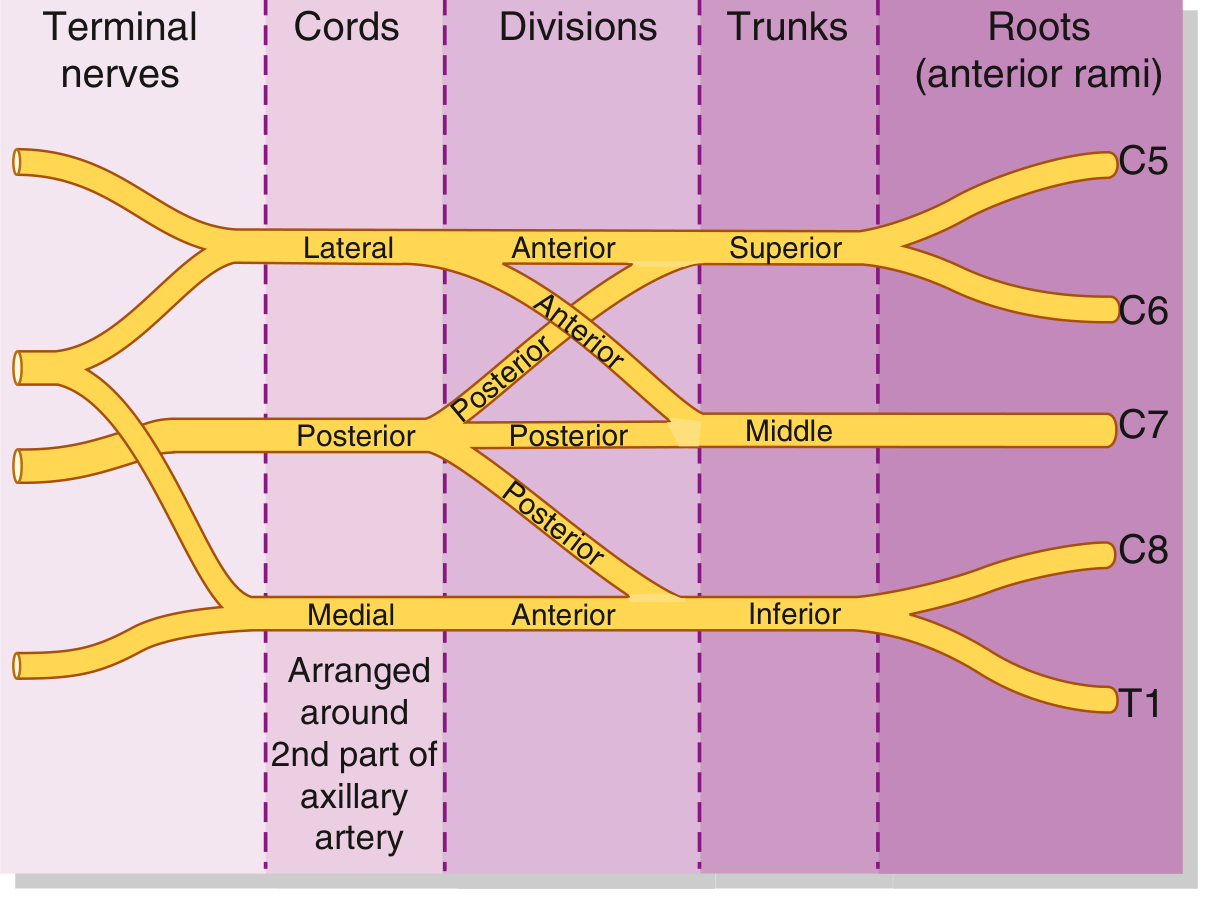
Structure: The "RTDC-B" Mnemonic
The plexus has 5 sequential levels: Roots → Trunks → Divisions → Cords → Branches
1. Roots
The five anterior rami (C5-T1) pass between the anterior and middle scalene muscles. They receive gray rami communicantes from the sympathetic trunk.
Branches directly from roots:
- Dorsal scapular nerve (C5) - rhomboid major and minor
- Long thoracic nerve (C5, C6, C7) - serratus anterior
- Small contribution to the phrenic nerve (C5)
2. Trunks (3 trunks)
| Trunk | Formed by | Location |
|---|---|---|
| Superior (upper) | C5 + C6 | Above subclavian artery |
| Middle | C7 alone | Above subclavian artery |
| Inferior (lower) | C8 + T1 | On rib I, behind subclavian artery |
Branches from trunks (both from superior trunk only):
- Suprascapular nerve (C5, C6) - supraspinatus and infraspinatus
- Nerve to subclavius (C5, C6)
3. Divisions
Each trunk splits into an anterior and a posterior division (6 divisions total). No nerves arise directly from divisions.
- Anterior divisions - supply anterior (flexor) compartments
- Posterior divisions - supply posterior (extensor) compartments
4. Cords (named by relation to the 2nd part of the axillary artery)
| Cord | Formed by | Root values | Position |
|---|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5, C6, C7 | Lateral to axillary artery |
| Medial | Anterior division of inferior trunk | C8, T1 | Medial to axillary artery |
| Posterior | All 3 posterior divisions | C5-T1 | Posterior to axillary artery |
5. Branches (Terminal and Collateral)
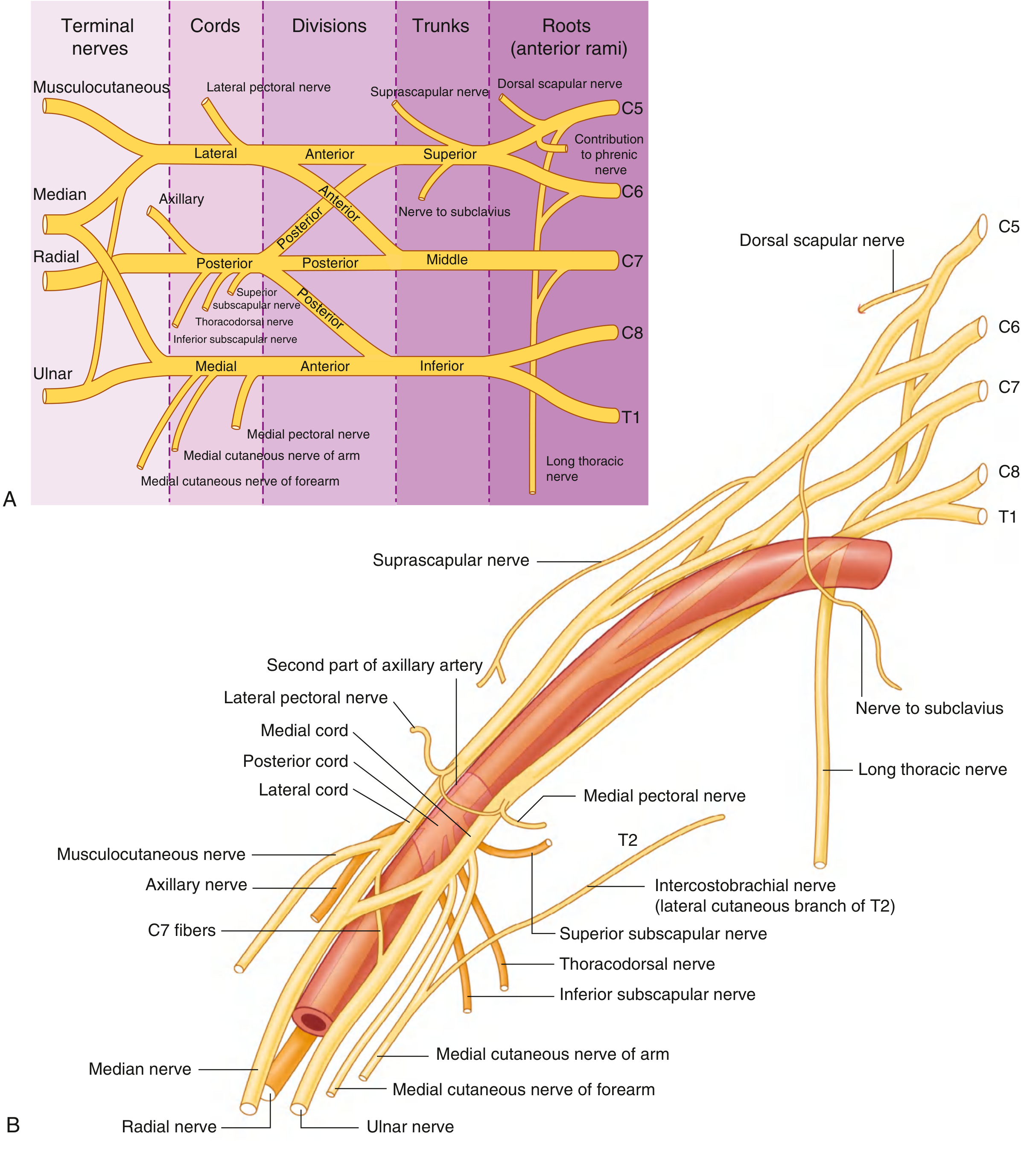
From Lateral Cord:
- Lateral pectoral nerve (pectoralis major)
- Musculocutaneous nerve (biceps, brachialis, coracobrachialis; terminates as lateral cutaneous nerve of forearm)
- Lateral root of the median nerve
From Medial Cord:
- Medial pectoral nerve (pectoralis minor and major)
- Medial cutaneous nerve of the arm
- Medial cutaneous nerve of the forearm
- Ulnar nerve (C8, T1)
- Medial root of the median nerve
From Posterior Cord:
- Upper subscapular nerve (subscapularis)
- Thoracodorsal nerve (latissimus dorsi)
- Lower subscapular nerve (subscapularis and teres major)
- Axillary nerve (deltoid, teres minor)
- Radial nerve (C5-T1; all extensors of arm, forearm, and hand)
Median nerve = lateral root (from lateral cord) + medial root (from medial cord)
Lesions of the Brachial Plexus
Complete Lesion
Rare; occurs only after severe trauma (e.g., high-speed accidents). All roots are damaged. Results in:
- Complete paralysis of the upper limb
- Anaesthesia of the entire limb except the upper arm (C3, C4 territory)
- The long thoracic nerve (serratus anterior) or dorsal scapular nerve (rhomboids) may occasionally escape
(S Das, Manual on Clinical Surgery, 13th Ed.)
Incomplete/Partial Lesions
A. Upper Brachial Plexus Lesion - Erb-Duchenne Palsy (C5, C6)
Mechanism: Forcible widening of the angle between neck and shoulder (shoulder depression + head/neck lateral flexion away). This stretches/damages the upper trunk of the plexus at Erb's point (junction of C5 and C6, just above the clavicle).
Causes:
- Birth injury (difficult labour - excessive lateral traction on the head during delivery)
- Motorcycle accidents (head forced away from shoulder)
- Fall of a heavy load on the shoulder
Muscles paralysed: Deltoid, biceps, brachialis, brachioradialis, supinator (C5/C6 muscles)
Classic posture: "Policeman's tip" or "Waiter's tip" deformity
- Arm: adducted, internally rotated (deltoid paralysed)
- Elbow: extended (biceps/brachialis paralysed)
- Forearm: pronated (supinator/biceps paralysed)
Sensory loss: Over the lateral aspect of the arm and upper lateral forearm (C5/C6 dermatomes)
B. Lower Brachial Plexus Lesion - Klumpke's Palsy (C8, T1)
Mechanism: Forcible hyperabduction of the arm, which stretches the lower trunk (C8, T1).
Causes:
- Birth injury (breech presentation with arms above the head)
- Adult: catching a falling object; grabbing a rail of a moving bus
- Pancoast tumour (apex lung tumour invading T1 root)
Muscles paralysed: All intrinsic muscles of the hand (interossei, lumbricals, thenar, hypothenar) - combined median + ulnar intrinsic palsy
Deformity: Clawhand (intrinsic minus hand) - hyperextension at MCPs, flexion at IPJs
Sensory loss: Medial forearm, medial hand, and medial 1½ fingers (C8, T1 dermatomes)
Associated finding: Horner's syndrome (ptosis, miosis, enophthalmos, anhidrosis) - because T1 root carries preganglionic sympathetic fibres to the superior cervical ganglion via the cervicothoracic (stellate) ganglion. Indicates a root avulsion or proximal injury.
Summary Table of Plexus Lesions
| Feature | Erb-Duchenne (C5, C6) | Klumpke's (C8, T1) |
|---|---|---|
| Level | Upper trunk | Lower trunk |
| Mechanism | Neck-shoulder angle forced open | Arm hyperabducted |
| Deformity | "Waiter's tip" | Claw hand |
| Paralysis | Deltoid, biceps, brachialis, brachioradialis | Hand intrinsics |
| Sensory loss | Lateral arm and forearm | Medial forearm and hand, ulnar 1½ fingers |
| Horner's | Absent | Present (if T1 root involved) |
Other Clinically Important Lesions
| Nerve | Root | Cause | Deficit |
|---|---|---|---|
| Long thoracic nerve | C5-C7 | Stab, radical mastectomy, rucksack palsy | Serratus anterior paralysis → winged scapula |
| Axillary nerve | C5, C6 | Shoulder dislocation, surgical neck of humerus fracture | Deltoid paralysis, loss of shoulder abduction; sensory loss over the "regimental badge" area |
| Musculocutaneous | C5-C7 | Penetrating injury, coracobrachialis tear | Weak elbow flexion and supination; sensory loss lateral forearm |
| Radial nerve | C5-T1 | Humeral shaft fracture (spiral groove), crutch palsy | Wrist drop, finger drop; sensory loss dorsal hand/thumb web |
| Median nerve | C6-T1 | Carpal tunnel, supracondylar fracture | "Ape hand" (thenar wasting), loss of thumb opposition; sensory loss lateral 3½ fingers palmar |
| Ulnar nerve | C8, T1 | Medial epicondyle fracture, cubital tunnel | "Claw hand" (lateral 2 fingers), interosseous wasting; sensory loss medial 1½ fingers |
Causalgia
A constant, intense burning pain after partial nerve injury. It may begin immediately after injury or weeks later (after the wound has healed). Caused by partial nerve damage with autonomic fibre involvement.
(S Das, Manual on Clinical Surgery, 13th Ed.)
Key Clinical Points
- Erb's point is where C5 and C6 roots merge to form the upper trunk - the most vulnerable point in birth injuries.
- Pre-ganglionic vs post-ganglionic avulsion: Presence of Horner's syndrome in lower plexus injury strongly suggests preganglionic root avulsion (the nerve root is torn from the spinal cord), which cannot recover spontaneously and requires nerve transfer surgery rather than repair.
- Pancoast tumour (apex lung carcinoma) can mimic Klumpke's palsy by compressing the lower trunk/T1 root from below.
- Rucksack/backpack palsy classically damages C5/C6 (upper trunk) by prolonged shoulder strap compression.
- The posterior cord gives rise to radial and axillary nerves - posterior cord injuries present with wrist drop and inability to abduct the shoulder.
- Gray's Anatomy for Students (Gray's), pp. 858-861
- S Das Manual on Clinical Surgery, 13th Ed., pp. 140-141
This is a shared conversation. Sign in to Orris to start your own chat.