ECMO 10 marks short note for MD ANAESTHESIOLOGY exam
Reading File
Finding Sources
Searching the Web
ECMO extracorporeal membrane oxygenation anaesthesiology MD exam short note 10 marks
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent comprehensive content from Miller's Anesthesia and Fishman's Pulmonary Diseases. I have enough to write a thorough 10-mark short note. Let me compose the answer:
ECMO (Extracorporeal Membrane Oxygenation)
Short Note - MD Anaesthesiology (10 Marks)
Definition
ECMO is a form of prolonged extracorporeal cardiorespiratory support that adds oxygen to and removes CO2 from circulating blood outside the body, supporting failing heart and/or lungs for days to weeks. It evolved from the cardiopulmonary bypass circuit first used by Gibbon in 1953. The first successful prolonged ECMO use outside the OR was reported by Hill et al. in 1972 in an ARDS patient.
- Miller's Anesthesia, 10e, p. 12105
ECMO Circuit - Components
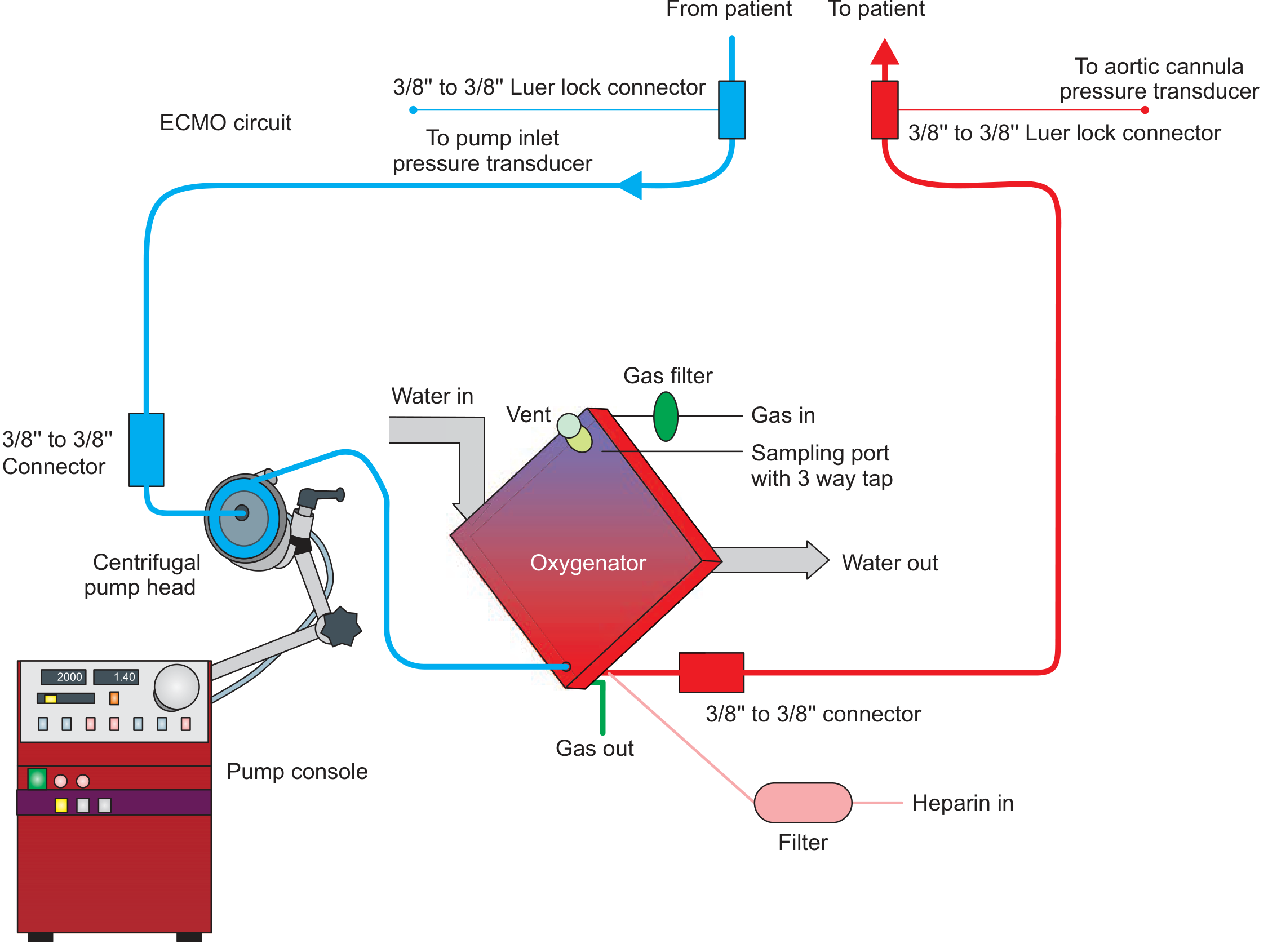
The circuit comprises:
- Inflow (drainage) cannula - drains venous blood from the patient
- Centrifugal pump - nonpulsatile; generates blood flow (2-7 L/min)
- Membrane oxygenator - hollow-fiber design; oxygen diffuses through a lattice membrane (<1 µm pore size) into blood; CO2 removed in the opposite direction. The gas flow through the oxygenator is called the "sweep"
- Outflow (return) cannula - returns oxygenated blood to patient
- Heat exchanger - warms blood returning to patient
- It is a closed system (no open reservoir), unlike CPB circuits
Key distinction from CPB: ECMO circuits are heparin-bonded, designed for long-term use (days/weeks), and use smaller-bore cannulae; CPB is an open system for short-term surgical use.
- Miller's Anesthesia, 10e, p. 12105; Fishman's Pulmonary Diseases, p. 2642
Types / Configurations
1. Venovenous (VV) ECMO
- Drains venous blood and returns oxygenated blood to the venous system (right heart)
- Supports lungs only - no cardiac support
- Cannulation: femoral vein (drainage) + internal jugular vein (return), OR single dual-lumen cannula via right internal jugular
- Used for: isolated respiratory failure (ARDS, pneumonia, ECCO2R)
- Native cardiac output must be maintained
2. Venoarterial (VA) ECMO
- Drains venous blood and returns oxygenated blood to the arterial system
- Supports both heart and lungs
- Cannulation: femoral artery (return) + femoral/internal jugular vein (drainage), or central (aorta/RA)
- Used for: cardiogenic shock, cardiac arrest, combined cardiorespiratory failure
- Risk: differential hypoxia (Harlequin syndrome) - hypoxic blood from the native heart perfuses coronary and cerebral circulation when proximal aorta is supplied by the failing heart and distal aorta by ECMO
3. Venous-Pulmonary Artery (VPA) ECMO
- Supports right heart + lungs; left heart not supported
- Used for: right heart failure combined with respiratory failure
4. Hybrid circuits: VV-A and V-AV
-
VV-A: provides additional venous return for low-flow states
-
V-AV: manages cerebral hypoxemia seen in peripheral VA ECMO
-
Miller's Anesthesia, 10e, p. 12103-12105
Indications
VV ECMO (Respiratory)
| Indication | Criteria |
|---|---|
| Severe ARDS | PaO2 <80 mmHg on FiO2 100%, or pH <7.2 with hypercarbia unresponsive to conventional therapy |
| Severe pneumonia (viral/bacterial) | Refractory to conventional ventilation |
| Status asthmaticus | Refractory |
| Bridge to lung transplant | As stabilizing measure |
| ECCO2R | Isolated hypercapnia, permissive hypercapnia |
VA ECMO (Cardiac)
-
Refractory cardiogenic shock (any cause) - hypotension/poor tissue perfusion despite maximum medical therapy ± IABP
-
Failure to separate from CPB
-
Fulminant myocarditis
-
Peripartum cardiomyopathy
-
Decompensated chronic heart failure, right heart failure
-
Drug/toxin-induced cardiac failure
-
Postcardiotomy shock
-
Massive pulmonary embolism
-
Refractory ventricular arrhythmias
-
ECPR (ECMO-assisted CPR) - for refractory cardiac arrest
-
Bridge to durable VAD or cardiac transplant
-
Intraoperative lung/heart transplant support
-
Fishman's Pulmonary Diseases, p. 2647; Miller's Anesthesia, 10e, p. 12120
Contraindications
| Absolute | Relative |
|---|---|
| Age >70 years (VV ECMO) | Weight >140 kg |
| Irreversible organ damage (brain death, terminal malignancy) | Prolonged mechanical ventilation (>7 days, high settings) |
| Uncontrolled systemic infection/sepsis | Immunosuppression |
| Severe aortic regurgitation (VA ECMO) | Unwitnessed cardiac arrest |
ECMO should only be initiated when the underlying condition is potentially reversible or when the patient is a candidate for transplant or durable mechanical support (bridge strategy).
Physiological Principles
- Oxygenation is controlled by blood flow rate through the oxygenator
- CO2 removal is controlled by sweep gas flow rate (increasing sweep = more CO2 removed)
- The membrane oxygenator uses hollow-fiber technology; pore size <1 µm prevents plasma leakage
- Diffusion path for gas exchange is ~100 µm through the lattice matrix
- Recirculation is a key problem in VV ECMO - returned oxygenated blood is re-drained before reaching the right heart, reducing effective circuit output
Anticoagulation
- Systemic heparin is the standard anticoagulant (infused via circuit)
- Target: activated clotting time (ACT) 180-220 sec, or anti-Xa levels, or aPTT 60-80 sec (institution-specific)
- Heparin-bonded circuits reduce but do not eliminate the need for anticoagulation
- Higher anticoagulation required at lower flow rates
- Alternatives: bivalirudin (HIT, heparin resistance), argatroban
Management During ECMO - Role of the Anaesthesiologist
The cardiac anaesthesiologist plays a key role in:
- Cannulation and decannulation - providing procedural sedation/anaesthesia, echocardiographic guidance for cannula placement
- Echocardiography (TOE/TTE) - assessing cannula position, cardiac function, ventricular filling
- Sedation management - optimising patient comfort and preventing circuit disruption
- Pharmacokinetic alterations - ECMO causes significant sequestration and altered distribution of drugs; increased volume of distribution; lipophilic and protein-bound drugs (propofol, fentanyl, midazolam) are adsorbed by the circuit; antibiotic dosing must be adjusted
- Ventilator management - "lung rest" strategy: low tidal volumes (4-6 mL/kg), low FiO2, low PEEP, low RR
- ICU co-management - as anaesthesiologist-intensivist for ongoing ECMO management
Complications
| Category | Complications |
|---|---|
| Vascular | Limb ischaemia (most common with femoral VA), vessel injury during cannulation, distal limb ischaemia (requires distal perfusion cannula) |
| Bleeding | Intracranial haemorrhage, cannula site bleeding, GI bleed (anticoagulation + coagulopathy) |
| Thrombotic | Circuit thrombus, oxygenator failure, DVT, stroke |
| Haematological | Haemolysis (elevated LDH, plasma Hb), thrombocytopenia, HIT |
| Infectious | Cannula-site infection, circuit contamination, nosocomial pneumonia |
| Circuit-specific | Air embolism, oxygenator failure, pump failure, tubing rupture |
| VA-specific | Harlequin/differential hypoxia syndrome, LV distension and pulmonary oedema, increased LV afterload |
| Renal | AKI - often requiring CRRT (can be integrated into ECMO circuit) |
- Fishman's Pulmonary Diseases, p. 2647; Miller's Anesthesia, 10e
Weaning from ECMO
VV ECMO weaning:
- Gradually reduce blood flow; if SpO2 and PaO2 maintained on moderate ventilator settings, patient is ready
- Perform a 1-4 hour "trial off" (circuit kept primed and flowing at minimal rate but clamp trial)
- Successful weaning: adequate gas exchange on lung-protective ventilation without ECMO
VA ECMO weaning:
- Gradually reduce flow while increasing inotropic support
- Monitor: arterial pulse pressure (increasing pulse pressure = recovering LV function), LVOT VTI on echo, mixed venous O2
- Failure to wean: consider upgrading to durable VAD or listing for transplant
Outcomes
| Setting | Survival to Discharge |
|---|---|
| VV ECMO (ARDS - viral/bacterial) | ~60% in adults |
| VA ECMO (severe cardiac failure) | ~40% |
| ECMO-CPR (ECPR) | ~29% in adults |
| VA ECMO - myocarditis | ~67% |
| VA ECMO - postcardiotomy | 45-66% |
- Miller's Anesthesia, 10e, p. 12119
ELSO (Extracorporeal Life Support Organization)
Founded in 1989 at the University of Michigan; European ELSO group 1991. ELSO maintains international registry, sets guidelines, and provides education. Current ELSO guidelines are the standard reference for ECMO indications, management, and outcomes reporting.
Key Points for Exam
- ECMO = "bridging therapy" - always aimed at recovery, transplant, or durable device
- VV ECMO = lungs only; VA ECMO = heart + lungs
- CO2 controlled by sweep gas; O2 delivery controlled by blood flow
- Harlequin syndrome = differential hypoxia specific to peripheral VA ECMO
- Anticoagulation = heparin (institution-specific targets)
- Drug pharmacokinetics are profoundly altered - especially lipophilic, protein-bound drugs
- Decision to initiate ECMO must be team-based, with pre-ECMO assessment of likelihood of survival or candidacy for transplant/device
Sources: Miller's Anesthesia 10th Edition, Chapter 81 (pp. 12103-12121); Fishman's Pulmonary Diseases and Disorders, Chapter 149 (pp. 2641-2648); Fischer's Mastery of Surgery 8th Edition
Golden hour 10 marks short note for MD ANAESTHESIOLOGY exam
Reading File
Finding Sources
Finding Sources
Searching the Web
golden hour trauma anaesthesiology MD exam short note resuscitation ATLS
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Excellent - I now have comprehensive, authoritative textbook content from multiple sources. Let me compile the full short note:
THE GOLDEN HOUR
Short Note - MD Anaesthesiology (10 Marks)
Definition and Origin
The "Golden Hour" in trauma refers to the first 60 minutes following traumatic injury, during which prompt and prioritized medical and surgical intervention has the highest likelihood of preventing death and permanent disability. The concept is attributed to R. Adams Cowley, founder of the Baltimore Shock Trauma Institute, who stated in 1975: "the first hour after injury will largely determine a critically injured person's chances for survival."
The ATLS (Advanced Trauma Life Support) course of the American College of Surgeons, developed in the late 1970s and now taught in over 60 countries, formally enshrines this principle - emphasizing that timely, prioritized interventions are necessary to prevent death and disability.
Important caveat: The term is now understood as a conceptual framework for urgency rather than a strict 60-minute biological cutoff. Survival does not uniformly drop after exactly 60 minutes; the window depends on injury type. Some injuries (e.g., penetrating cardiac wounds) allow minutes; others allow more time.
- Schwartz's Principles of Surgery, 11e, p. 211; Mulholland & Greenfield's Surgery, 7e, p. 1043
Epidemiology of Trauma - Why the Golden Hour Matters
-
Trauma is the most common cause of death for individuals aged 1 to 44 years, and the third most common cause of death regardless of age
-
Most victims are young males - enormous societal burden of years of life lost
-
Most preventable trauma deaths are due to haemorrhage and traumatic brain injury (TBI)
-
Bleeding remains the number one cause of preventable death during the first 6 hours following trauma
-
Haemorrhage accounts for ~30-40% of all trauma deaths
-
Schwartz's Principles of Surgery, 11e, p. 211
Trimodal Distribution of Trauma Deaths
Trauma deaths classically follow a trimodal distribution (described by Trunkey, 1983):
| Peak | Timing | Causes | Preventability |
|---|---|---|---|
| 1st peak - Immediate | Seconds to minutes at scene | Loss of airway, devastating brain/spinal cord injury, great vessel rupture, massive haemorrhage | Mostly unpreventable |
| 2nd peak - Early | Minutes to hours (within the "Golden Hour") | Subdural/epidural haematoma, haemothorax, pneumothorax, solid organ injury, pelvic/long bone haemorrhage | Highly preventable with ATLS-guided resuscitation |
| 3rd peak - Late | Days to weeks | Multi-organ failure (MOF), sepsis, ARDS | Preventable with optimal early and critical care |
The Golden Hour specifically targets the 2nd peak - the early preventable deaths.
Contemporary update: With modern ICU care, the late peak has markedly diminished. Recent multinational data (>20,000 patients) show a predominantly bimodal distribution - 61% immediate, 29% early, only 10% late - the third peak has been "flattened" by improved critical care.
- Mulholland & Greenfield's Surgery, 7e, p. 1036-1037; Rockwood & Green's Fractures, 10e
The "Platinum 10 Minutes" - Prehospital
A related concept - Platinum 10 Minutes - limits prehospital scene time to no more than 10 minutes for stabilisation before transport to a trauma centre. The key prehospital principle is "scoop and run" rather than prolonged on-scene treatment for penetrating trauma, while providing "stay and play" is reserved for specific interventions (airway, tourniquet, tension pneumothorax decompression).
Key prehospital interventions during the Golden Hour:
- Airway control (jaw thrust, BVM, supraglottic airway, RSI if trained)
- Haemorrhage control (tourniquet for limb haemorrhage, direct compression, wound packing)
- Cervical spine immobilisation (blunt trauma)
- Rapid transport to appropriate facility (trauma centre)
ATLS Framework - Management During the Golden Hour
The ATLS primary survey provides the structured approach:
ABCDE
| Step | Action | Key Points |
|---|---|---|
| Tourniquet, direct pressure, wound packing | "XABC" format (haemorrhage first) | |
| A - Airway (+ C-spine) | Inspect, suction, open; RSI/intubation if indicated | Cervical collar for blunt trauma |
| B - Breathing | Assess, decompress tension pneumothorax (2nd ICS MCL), seal open chest wounds, drain haemothorax | Immediate intervention for life threats |
| C - Circulation | IV/IO access x2 large bore, fluid resuscitation, haemorrhage control | Identify shock; activate MTP if needed |
| D - Disability | GCS, pupils, motor, AVPU | Identify herniation; treat with hyperventilation/mannitol temporarily |
| E - Exposure | Fully expose patient, logroll, prevent hypothermia | Remove all clothes, warm blankets |
- Schwartz's Principles of Surgery, 11e, p. 211; Mulholland & Greenfield's Surgery, 7e, p. 1043
Haemorrhage Classification (ATLS / ACS)
| Class | Blood Loss | % of CBV | HR | BP | Signs | Management |
|---|---|---|---|---|---|---|
| I | <750 mL | <15% | Normal | Normal | Minimal | Observe; crystalloid if needed |
| II | 750-1500 mL | 15-30% | >100 bpm | Normal/↑DBP | Anxious, tachycardia | IV crystalloid |
| III | 1500-2000 mL | 30-40% | >120 bpm | ↓SBP | Confused, tachypnoeic | Blood transfusion, damage control |
| IV | >2000 mL | >40% | >140 bpm | Profoundly ↓ | Unresponsive | DCR + damage control surgery |
(CBV = circulating blood volume; adult ~70 mL/kg; child ~80 mL/kg; infant ~90 mL/kg)
- Morgan & Mikhail's Clinical Anaesthesiology, 7e, p. 1537
The "Lethal Triad" (Bloody Vicious Cycle)
Class III/IV haemorrhage risks the lethal triad:
Hypothermia → Coagulopathy → Acidosis → ↑ Bleeding → ↑ Hypothermia...
This is a self-perpetuating cycle. Any prolonged operation in the severely injured patient accelerates this triad. Recognition and interruption during the Golden Hour is essential.
Trauma-Induced Coagulopathy (TIC):
-
Present in up to 25% of major trauma patients on arrival, before any resuscitative fluids
-
Driven by global tissue hypoperfusion (base deficit >6 mEq/L)
-
Not dilutional - it is a primary physiological coagulopathy
-
Independent risk factor for death
-
Morgan & Mikhail's Clinical Anaesthesiology, 7e, p. 1538; Mulholland & Greenfield's Surgery, 7e
Damage Control Resuscitation (DCR) - Core Principle of the Golden Hour
DCR replaces traditional crystalloid-heavy resuscitation and consists of:
- Permissive hypotension - target SBP 80-90 mmHg (MAP ~50 mmHg) until haemorrhage control, to avoid clot disruption (contraindicated in TBI)
- Avoid crystalloids - large volumes worsen coagulopathy, hypothermia, acidosis, and abdominal compartment syndrome
- Haemostatic resuscitation - early transfusion of blood components in 1:1:1 ratio (FFP : Platelets : PRBCs)
- Massive Transfusion Protocol (MTP) activation - predefined triggers (e.g., >10 units PRBCs in 24h; Shock Index >1; assessment of blood consumption [ABC] score ≥2)
- Tranexamic acid (TXA) - 1g IV over 10 minutes within 3 hours of injury (CRASH-2 trial); prevents fibrinolysis; significantly reduces haemorrhage-related mortality; a second 1g dose given over 8 hours
- Calcium replacement - hypocalcaemia is common after massive transfusion; calcium chloride 1g IV
- Prevent hypothermia - fluid warmers, forced air warming, warm theatre
- Correct acidosis - haemorrhage control + resuscitation; sodium bicarbonate only if pH <7.1
- Mulholland & Greenfield's Surgery, 7e, p. 1044-1046
Damage Control Surgery (DCS) - "Stop the Bleeding"
When the lethal triad is established or when patients cannot tolerate prolonged surgery:
- Abbreviated laparotomy - rapid entry, early bleeding control, temporary contamination control
- Temporary abdominal closure (TAC) - wound VAC or Bogota bag
- ICU resuscitation - 24-48 hours to correct physiology
- Return to OR for definitive repair once stabilised
Indications for DCS include:
-
Temperature <35°C
-
pH <7.20
-
Base deficit >14
-
SBP persistently <80 mmHg
-
Blood transfusion >10 units PRBCs
-
Estimated blood loss >4 L
-
Inability to achieve haemostasis
-
Mulholland & Greenfield's Surgery, 7e, p. 1036
The Five Sources of Significant Blood Loss
In blunt polytrauma, bleeding is confined to 5 anatomical locations (essential for the Golden Hour assessment):
- Pleural space (haemothorax - CXR/FAST)
- Intra-abdominal (FAST examination, diagnostic peritoneal aspiration)
- Pelvis / retroperitoneal space (pelvic X-ray; pelvic binder)
- Soft tissues at long bone fracture sites (clinical exam)
- External (visible - control directly)
FAST Examination - Bedside Tool of the Golden Hour
Focused Assessment with Sonography in Trauma (FAST):
- Rapid bedside USS to detect free fluid (blood) in pericardial, perihepatic, perisplenic, and pelvic spaces
- Extended FAST (eFAST) adds pleural assessment for pneumothorax/haemothorax
- In a hypotensive patient with positive FAST = emergent laparotomy justified
- False-negative rate varies; Diagnostic Peritoneal Aspiration (DPA) can be performed in 1 minute and is superior to FAST for haemodynamic instability with suspected abdominal source
Role of the Anaesthesiologist in the Golden Hour
- Airway management - RSI is the standard; modified RSI in haemodynamically unstable patients (ketamine preferred over propofol; avoid agents causing vasodilation)
- Haemodynamic resuscitation - arterial line, large-bore IV/IO access, point-of-care coagulation monitoring (TEG/ROTEM)
- Anaesthesia for damage control surgery - short, haemostasis-focused operations under total IV anaesthesia; maintain normothermia
- MTP management - coordinate blood bank, administer components, TXA, calcium
- Temperature management - active warming measures
- Neurological protection - avoid hypotension and hypoxia in TBI (SBP >90 mmHg, SpO2 >95%)
- Communication - team leader role in resuscitation bay
Injury Scoring Systems
| Score | Type | Details |
|---|---|---|
| ISS (Injury Severity Score) | Anatomic | Sum of squares of 3 worst AIS scores (0-75); ISS >15 = ~10% mortality |
| NISS (New ISS) | Anatomic | Top 3 AIS scores regardless of region; more predictive |
| RTS (Revised Trauma Score) | Physiologic | GCS + SBP + RR |
| TRISS | Combined | ISS + RTS + age |
| APACHE II | Physiologic | Used in ICU for late deaths |
Key Points for the Exam
- Golden Hour concept = R. Adams Cowley (1975); operationalised by ATLS
- Trimodal distribution - 1st peak (immediate, unpreventable), 2nd peak (early, preventable - the target), 3rd peak (late, MOF/sepsis - now flattened by modern ICU care)
- The two main killers during the Golden Hour = haemorrhage + TBI
- Lethal triad = Hypothermia + Coagulopathy + Acidosis
- TIC is present in 25% of major trauma patients on arrival - independent predictor of death
- DCR = permissive hypotension + haemostatic 1:1:1 resuscitation + TXA (within 3 hours)
- DCS = abbreviated surgery to stop bleeding + ICU resuscitation + return to OR
- 5 sites of significant blood loss: chest, abdomen, pelvis, long bones, external
- FAST/eFAST = primary imaging tool; DPA = rapid bedside alternative
- Platinum 10 minutes = pre-hospital scene time limit
Sources: Schwartz's Principles of Surgery 11e; Mulholland & Greenfield's Surgery 7e; Morgan & Mikhail's Clinical Anaesthesiology 7e; Rockwood & Green's Fractures in Adults 10e; ATLS 10th Edition
This is a shared conversation. Sign in to Orris to start your own chat.