Hey can you explain me about synclitism
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Now I have solid material to give a thorough, well-structured answer. Let me compile everything.
Synclitism (and Asynclitism) in Obstetrics
Definition
Synclitism is the normal, ideal alignment of the fetal head as it engages and descends into the maternal pelvis during labor. Specifically, it means the sagittal suture of the fetal skull lies exactly midway between the pubic symphysis (anteriorly) and the sacral promontory (posteriorly). In this position:
- Both parietal bones (right and left) present equally to the pelvic inlet
- The fetal head is perfectly perpendicular to the plane of the pelvis
- The biparietal diameter is optimally aligned with the transverse diameter of the pelvic inlet
Think of it as the head entering the pelvis in a perfectly "level," undilted posture.
How It Fits into Labor (Engagement)
Synclitism is most relevant during engagement - the first cardinal movement of labor - when the greatest transverse diameter of the head (the biparietal diameter) passes through the pelvic inlet. Engagement is said to have occurred when the presenting part reaches 0 station.
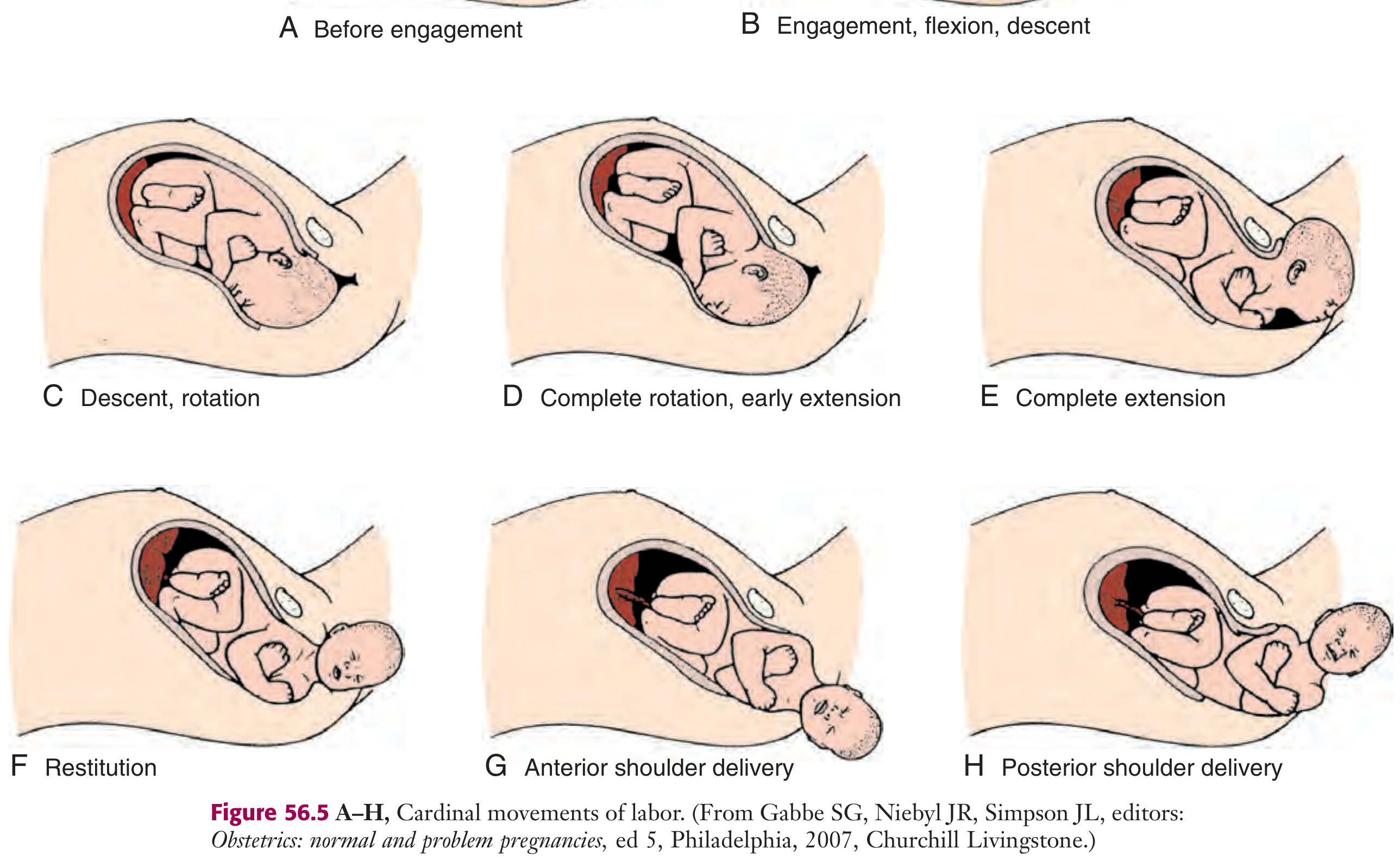
The full sequence of cardinal movements is:
- Engagement (synclitism is the normal state here)
- Flexion
- Descent
- Internal rotation
- Extension
- External rotation / restitution
- Expulsion
(Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1351)
The Opposite: Asynclitism
When the sagittal suture shifts away from the midpoint, the head is said to be asynclitic. This is a lateral tilting of the fetal head. There are two types:
| Type | Sagittal Suture Shift | Which Parietal Bone Leads |
|---|---|---|
| Anterior asynclitism (Naegele's obliquity) | Shifts toward sacrum | Anterior (pubic) parietal bone leads |
| Posterior asynclitism (Litzmann's obliquity) | Shifts toward symphysis | Posterior (sacral) parietal bone leads |
A mild degree of asynclitism is normal and even physiologically helpful in some cases, as the fetal head can use a slight lateral tilt to navigate the curved birth canal. However, marked asynclitism is abnormal.
Clinical Significance
- Marked asynclitism is associated with prolonged labor, arrest of descent, and failure of rotation - even in the presence of adequate uterine contractions. (Creasy & Resnik's Maternal-Fetal Medicine, p. 944)
- It also leads to overestimation of fetal station on vaginal examination, which can result in inappropriate decisions about assisted delivery (forceps, vacuum). (Pfenninger and Fowler's Procedures for Primary Care)
- Asynclitism can complicate vacuum extractor placement, as the fetal head is in a laterally deflected position, making correct cup placement harder. (Textbook of Family Medicine 9e)
- It is associated with brow presentation and posterior presentation as conditions that can lengthen the second stage.
How to Assess It Clinically
On vaginal examination during labor:
- Palpate the sagittal suture and determine its position relative to the symphysis and sacrum
- If the suture is central: synclitism (normal)
- If the suture is deviated anteriorly or posteriorly: asynclitism (abnormal if marked)
- The fontanelles (anterior = diamond-shaped, posterior = triangular) help confirm head position and degree of flexion
Summary Table
| Feature | Synclitism | Asynclitism |
|---|---|---|
| Sagittal suture position | Central (equidistant) | Deviated anterior or posterior |
| Parietal presentation | Equal | One parietal leads |
| Clinical significance | Normal, favorable | Marked = prolonged labor, arrest |
| Labor outcome | Optimal descent | May require intervention |
In short, synclitism describes the ideal neutral alignment of the fetal skull in the pelvis. It is the benchmark against which asynclitism - a deviation that ranges from physiologic to pathologic - is measured.
This is a shared conversation. Sign in to Orris to start your own chat.