I'm attending a workshop on ecg in mysore medical College and they have asked us to atleast know the basics . Give me all the information about ecg from standard physiology books
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the material needed to write a comprehensive, well-illustrated answer. Let me compile everything.
ECG — Basics from Standard Physiology Textbooks
Sources: Guyton & Hall Textbook of Medical Physiology, Ganong's Review of Medical Physiology (26th ed.), Costanzo Physiology (7th ed.)
1. What is an ECG?
The electrocardiogram (ECG or EKG) is a recording of the tiny electrical potential differences on the surface of the body that reflect the electrical activity of the heart. Body fluids are good conductors (the body acts as a "volume conductor"), so electrical currents generated by cardiac depolarization and repolarization spread all the way to the skin surface, where they can be detected by surface electrodes.
"When a cardiac impulse passes through the heart, electrical current also spreads from the heart into the adjacent tissues surrounding the heart. A small portion of the current spreads all the way to the surface of the body." — Guyton & Hall
2. Physiological Basis — Why Does the ECG Exist?
The ECG exists because the entire myocardium does not depolarize at once:
- The atria depolarize before the ventricles
- The ventricles depolarize in a specific sequence (endocardium → epicardium, apex → base)
- The atria repolarize while the ventricles are still depolarizing
- The ventricles repolarize in a sequence
This timing creates potential differences between different regions of the heart, which appear as waves on the ECG.
Key principle: When a depolarization wave moves toward an active electrode, it produces a positive (upward) deflection. When it moves away from the electrode, it produces a negative (downward) deflection.
3. The Cardiac Conduction System (What Generates the ECG)
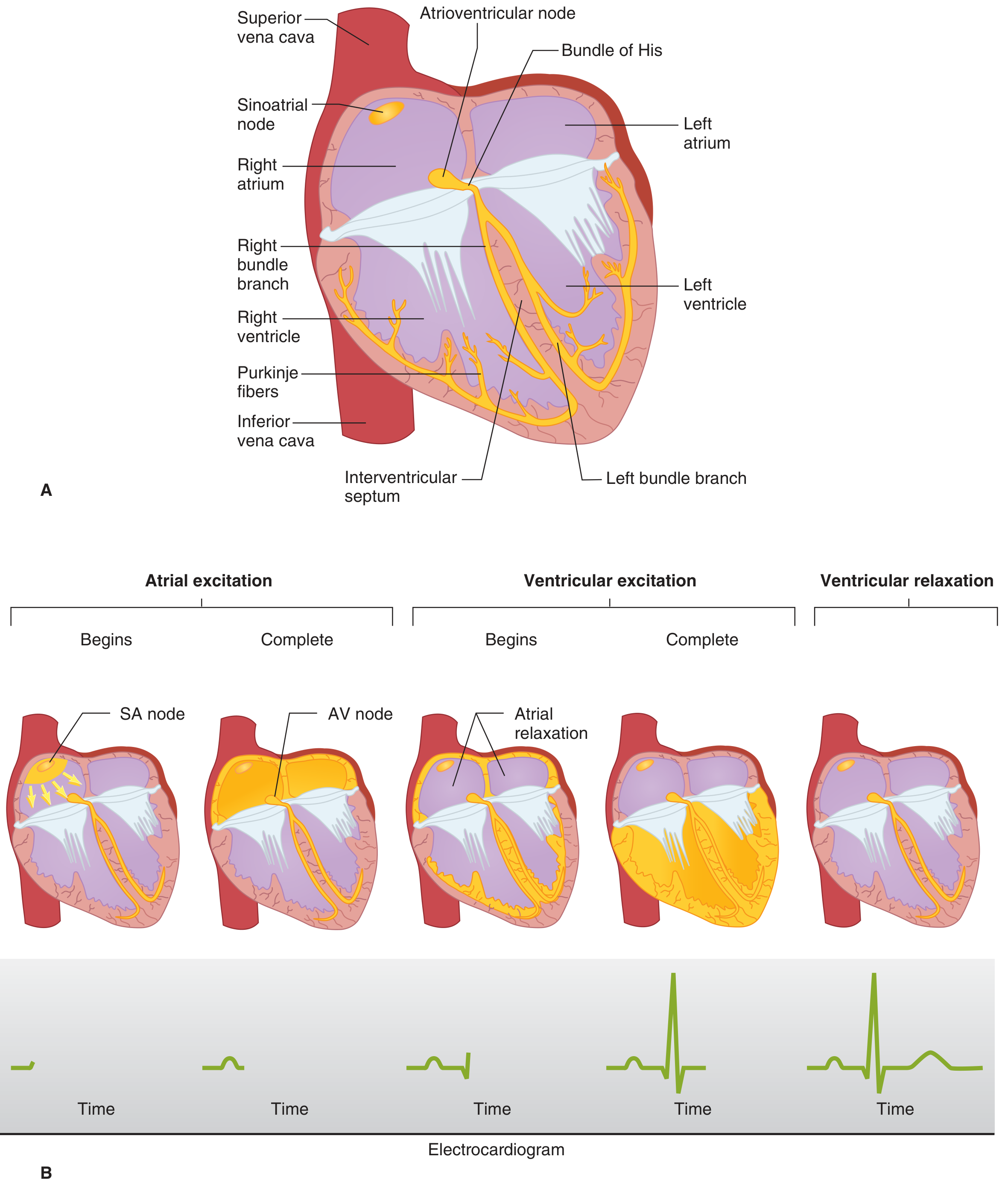
Ganong's Review of Medical Physiology — Conducting system of the heart (A) and sequence of cardiac excitation with the corresponding ECG below (B)
The impulse travels:
- SA node (pacemaker, right atrium) → spreads across both atria → P wave
- AV node (base of right atrium) → conduction slows here (built-in delay) → PR segment / isoelectric line
- Bundle of His → right and left bundle branches → Purkinje fibers → ventricular muscle → QRS complex
- Ventricular muscle repolarizes → T wave
4. Waveforms of the Normal ECG
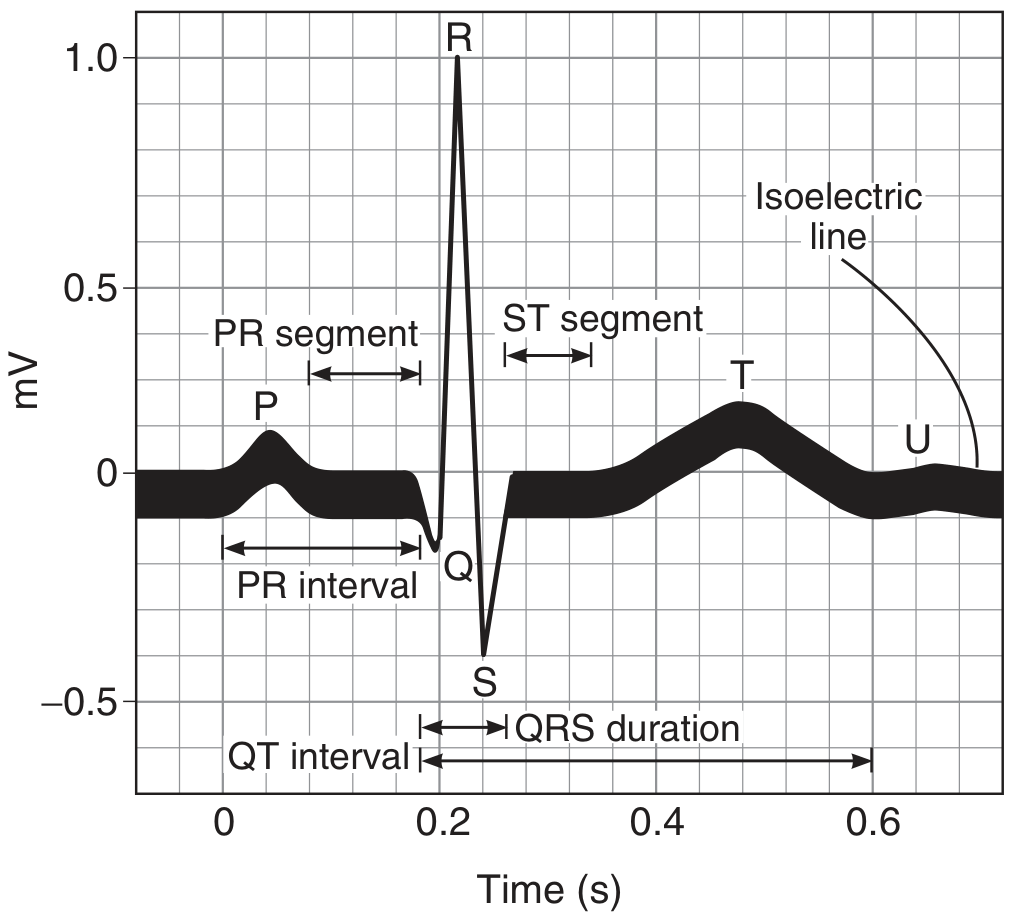
Ganong's Review of Medical Physiology — Standard names for waves, segments, and intervals of the ECG

Costanzo Physiology — The ECG measured from lead II
P Wave
- Represents depolarization of the atria
- Atrial repolarization is not seen on normal ECG — it is buried under the QRS complex
- Duration reflects conduction time through the atria
PR Interval
- Measured from the start of P wave to the start of QRS complex
- Represents conduction time from atria → AV node → bundle of His → ventricles
- Normal: 0.12–0.20 seconds (averages ~0.18 s at 70 bpm)
- PR segment (isoelectric flat line between P and QRS) = AV node conduction time
- Shortened by sympathetic stimulation; prolonged by parasympathetic stimulation
QRS Complex
- Represents depolarization of the ventricles
- Three components: Q (initial small downward deflection), R (tall upward), S (final downward)
- Although ventricles are much larger than atria, QRS duration is similar to P wave duration because the His-Purkinje system conducts extremely fast
- Normal QRS duration: up to 0.10 seconds
- Atrial repolarization is buried in this complex
ST Segment
- Isoelectric portion between end of QRS and start of T wave
- Corresponds to the plateau phase of the ventricular action potential (all ventricular cells are depolarized — no current flows between them)
- Should be on the isoelectric line (elevation or depression is clinically significant)
T Wave
- Represents repolarization of the ventricles
- Normally occurs 0.25–0.35 seconds after depolarization (Guyton)
- T wave is upright in most leads because repolarization proceeds in the opposite direction to depolarization (epicardium repolarizes before endocardium)
QT Interval
- From start of QRS to end of T wave
- Represents entire ventricular action potential (depolarization + repolarization)
- Normal: up to 0.43 seconds (corrected for heart rate)
- Increases at slower heart rates; decreases at faster heart rates
U Wave
- Small wave after the T wave; inconstant finding
- May be due to ventricular myocytes with long action potentials (Ganong)
5. ECG Intervals — Summary Table
(From Ganong's Review of Medical Physiology, Table 29-2)
| Interval | Average | Normal Range | Cardiac Event |
|---|---|---|---|
| PR interval | 0.18 s | 0.12–0.20 s | AV conduction (atria → ventricles) |
| QRS duration | 0.08 s | up to 0.10 s | Ventricular depolarization |
| QT interval | 0.40 s | up to 0.43 s | Ventricular action potential |
| ST segment | 0.32 s | — | Plateau of ventricular AP |
6. ECG Leads — The Recording System
An ECG lead is simply a pair of electrodes (or an electrode + reference point) that looks at the heart from a particular angle. The standard 12-lead ECG uses three sets of leads.
A. Standard Bipolar Limb Leads (Einthoven's Leads I, II, III)
These record the potential difference between two limbs:
| Lead | Positive Electrode | Negative Electrode |
|---|---|---|
| Lead I | Left arm | Right arm |
| Lead II | Left leg | Right arm |
| Lead III | Left leg | Left arm |
Einthoven's triangle: The heart sits in the center of an equilateral triangle formed by the three limb electrodes. The sum of voltages at the three points equals zero at all times. Einthoven's law: Lead II = Lead I + Lead III.
Einthoven's law: Upward deflections are recorded when the positive electrode becomes positive relative to the negative.
B. Augmented Unipolar Limb Leads (aVR, aVL, aVF)
In augmented leads, two limbs are connected to the negative terminal and the third limb is the positive (exploring) electrode:
| Lead | Positive Electrode | "Looks At" |
|---|---|---|
| aVR | Right arm | Right shoulder / base of heart |
| aVL | Left arm | Left shoulder |
| aVF | Left foot | Inferior heart (diaphragmatic surface) |
These increase amplitude by 50% compared to non-augmented unipolar leads. aVR is inverted relative to the others because it "looks away" from the main direction of depolarization.
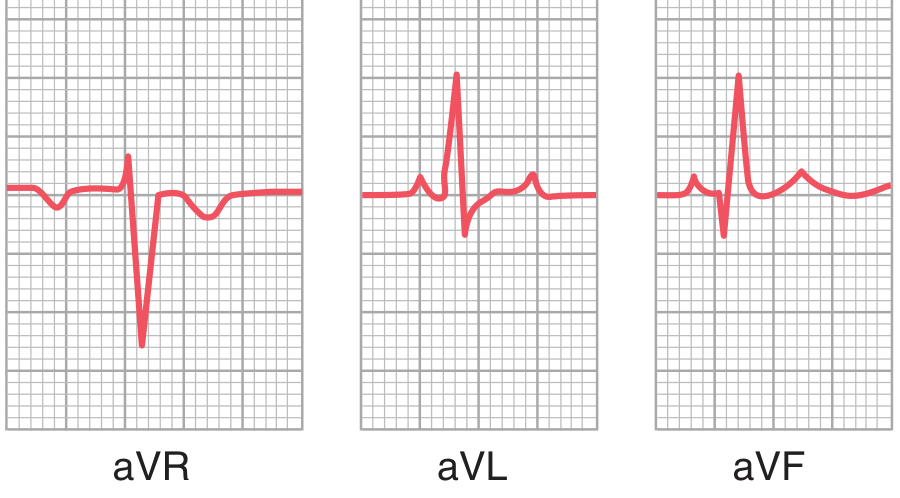
Guyton & Hall — Normal ECGs from the three augmented unipolar limb leads. Note aVR is inverted.
C. Precordial (Chest) Leads (V1–V6)
Six electrodes placed on the chest wall, each "looking" at the heart from in front:
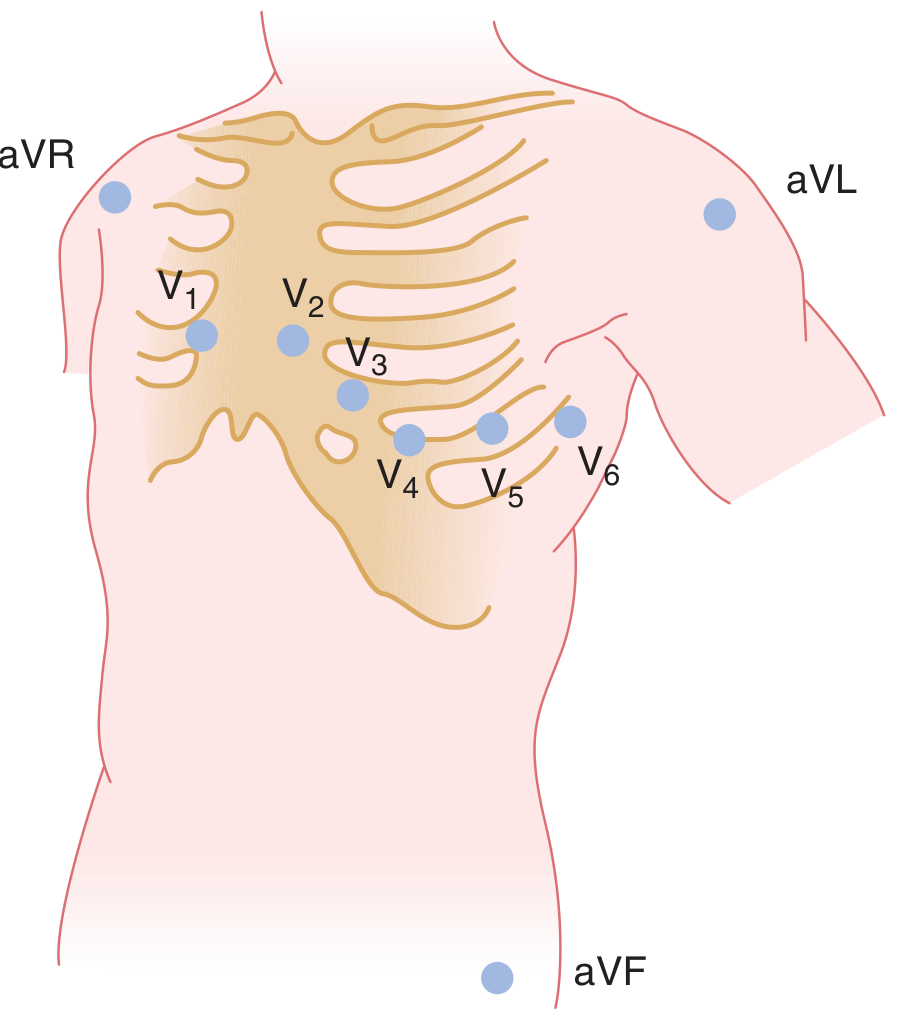
Ganong's Review — Placement of precordial leads V1–V6 and augmented limb leads
| Lead | Position |
|---|---|
| V1 | 4th intercostal space, right sternal border |
| V2 | 4th intercostal space, left sternal border |
| V3 | Between V2 and V4 |
| V4 | 5th intercostal space, mid-clavicular line |
| V5 | Anterior axillary line, same level as V4 |
| V6 | Mid-axillary line, same level as V4–V5 |
Key patterns in precordial leads:
- V1–V2: QRS mainly negative (electrode is near the base — electronegativity end during depolarization)
- V4–V6: QRS mainly positive (electrode is near the apex — electropositivity end during depolarization)
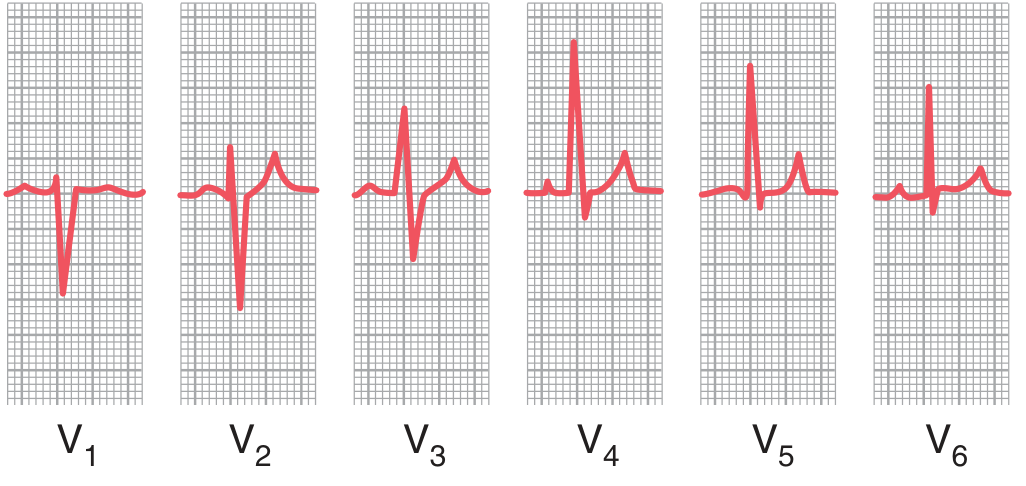
Guyton & Hall — Normal ECGs from leads V1 through V6. Note the transition from predominantly negative in V1 to predominantly positive in V4–V6.
7. ECG and the Cardiac Cycle — Timing Relationships
| ECG Event | Mechanical Event |
|---|---|
| P wave | Atrial depolarization → atrial contraction follows |
| PR segment | AV nodal delay |
| QRS complex | Ventricular depolarization → ventricular systole begins |
| ST segment | All ventricles depolarized, plateau phase; no contraction difference |
| T wave | Ventricular repolarization → ventricular relaxation begins |
"The QRS complex begins slightly before the onset of ventricular systole... The T wave occurs slightly before the end of ventricular contraction." — Guyton & Hall
8. Heart Rate from the ECG
- Count the number of QRS complexes (R waves) per minute
- At standard paper speed of 25 mm/s:
- Each large square = 0.2 s (5 mm)
- Each small square = 0.04 s (1 mm)
- Quick method: Divide 300 by the number of large squares between two consecutive R waves
- e.g., 4 large squares between R–R → 300 ÷ 4 = 75 bpm
9. Electrical Axis of the Heart
The direction of the mean electrical vector of ventricular depolarization is the electrical axis. Normally it points downward and to the left (0° to +90°, with +60° as the average), because the left ventricle dominates and the apex points down-left.
- Normal axis: 0° to +90°
- Left axis deviation: 0° to −90° (left ventricular hypertrophy, left bundle branch block)
- Right axis deviation: +90° to +180° (right ventricular hypertrophy, right bundle branch block)
10. Depolarization vs. Repolarization Waves — Why the T Wave is Upright
This is a classic exam point: the T wave is caused by repolarization, so why is it upright (same direction as the R wave)?
- In depolarization, the wave travels endocardium → epicardium (inside → outside)
- In repolarization, the wave travels epicardium → endocardium (outside → inside — reversed order)
- Because both direction and sign are reversed, the net deflection is the same direction as the QRS
- This produces an upright T wave that correlates with the QRS polarity
11. Clinical Significance of Key ECG Changes (Brief Overview)
| Finding | Possible Cause |
|---|---|
| Prolonged PR interval (>0.20 s) | First-degree AV block |
| Wide QRS (>0.12 s) | Bundle branch block, ventricular ectopy |
| ST elevation | Myocardial infarction (STEMI), pericarditis |
| ST depression | Myocardial ischemia, posterior MI |
| Prolonged QT | Hypocalcemia, drugs, risk of torsades de pointes |
| Tall peaked T waves | Hyperkalemia |
| Inverted T waves | Ischemia, ventricular hypertrophy |
| Absent P waves + irregular rhythm | Atrial fibrillation |
12. Quick Revision Summary
| Feature | Description |
|---|---|
| P wave | Atrial depolarization |
| PR interval | AV conduction time (0.12–0.20 s) |
| QRS complex | Ventricular depolarization (<0.10 s) |
| ST segment | Ventricular plateau (isoelectric) |
| T wave | Ventricular repolarization (upright) |
| QT interval | Total ventricular electrical activity (<0.43 s) |
| 12 leads | I, II, III + aVR, aVL, aVF + V1–V6 |
| Normal axis | 0° to +90° |
| Paper speed | 25 mm/s; large square = 0.2 s |
| Heart rate | 300 ÷ R-R in large squares |
All content compiled from: Guyton and Hall Textbook of Medical Physiology (Chapters 11–13), Ganong's Review of Medical Physiology, 26th edition (Chapter 29), and Costanzo Physiology, 7th edition (Chapter 4).
This is a shared conversation. Sign in to Orris to start your own chat.